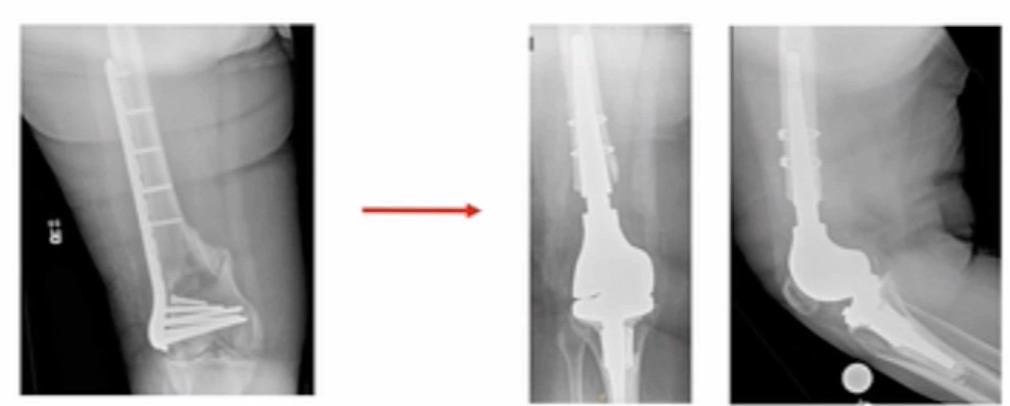

I’ve been tasked to present the Pro-Distal Femoral Replacement (DFR). It’s really not ORIF versus DFR, and which one’s better of course, that’s way too simplistic. It’s about finding the patients that are candidates for DFR and then making the decision to proceed with that. I would start with this. This is a patient I saw not too long ago; she had a distal femur fracture treated somewhere else, and she’s morbidly obese, and had a shorter steel plate implanted. (Figure 1)
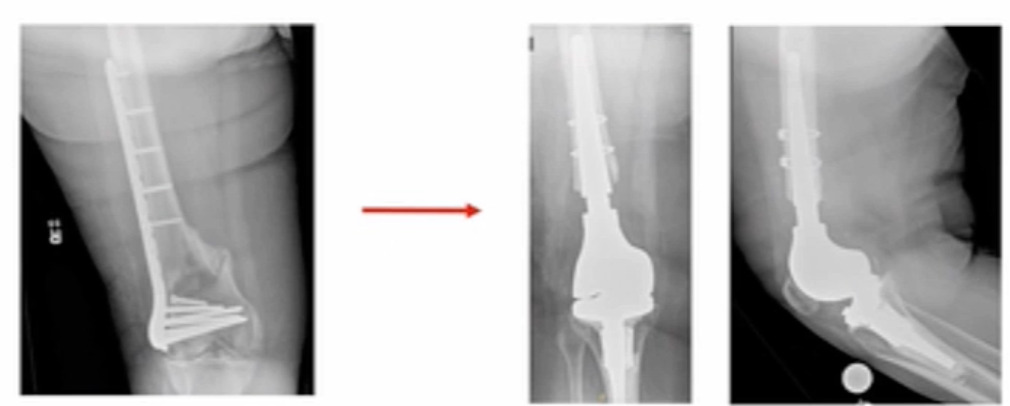
This patient is at “high risk” to develop a non-union. We ultimately converted her to a distal femur replacement about nine months after her initial surgery and she asked me, “why didn’t we just do this in the first place?” It’s hard to answer.
I think the key as we go forward is to figure out who the right patient. Across the literature, there’s a lot of selection bias. If you read Journal of Orthopaedic Trauma, ORIF is the way to go. If you read Journal of Arthroplasty, DFR is the way to go. Maybe it’s my oncology background, but I think informed decision making is important and in finding the appropriate candidates and then discussing the options with these patients.
We can see that the instances of fractures in high-risk patients are increasing, and mortality is very high. Five-year mortality rates are 57%. That’s the worse than most of my osteosarcoma patients (Walter et al. 2024). These fractures are very impactful. Making the right decision or at least having informed decisions with the patients is very important. Unfortunately, it’s not that simple (we’re not cavemen). We’ve had to be thoughtful about this. Not all fractures are the same and categorizing them is necessary.
We also had a discussion earlier about amputation, and we published a paper on this regarding “cognitive bias.” (Gurich 2020) It’s very easy to influence patients. We performed a study of patients using cognitive bias techniques to see if we could get patients to decide if they want an amputation in your limb salvage and you certainly can bias people. “Informed decision making” is very important and the World Health Organization (WHO) now has a whole body to help inform physicians how to perform informed decision making with patients. If someone is so convinced, like Dr. Meeting showed us earlier about the Mark Twain “be careful if you’re sure you’re right,” it’s not your values that matter, it’s the patient’s values. We need to bring them the information and then help them decide what they want to do.
Our AO colleagues are the experts in fixing bones. They even tell us that DFR is an option (and we know it’s certainly an option). The key is figuring with whom we should offer what option to and make certain we perform complete informed decision making as we move forward. Which fractures are we talking about? We’re not talking about simple distal femur fractures, it’s about comminuted, smashed, shattered distal femurs. Those are the patients that we’re considering these surgeries for. Osteoporosis, of course, is a risk factor for failure in non-union and re-operation, and we know it’s very common particularly in older, post-menopausal women, and in the femur (Warriner et al. 2011). There are some studies looking at high risk patients for reoperation and non-union (Sainio et al. 2023). Another study showed that elevated BMI and female patients were more predictive of reoperation, with BMI, segmental bone loss, anemia and open fractures being associated with higher risk of non-union rate (13.8%) (Cone et al. 2023).
Technique matters, and how we fix it matters (Henderson et al. 2011)!
-
You don’t want to put a screw next to the fracture.
-
You want longer plates.
-
And you don’t want to use stainless steel (higher non-union rates).
-
Use titanium because of the flexibility of the implant more closely matches bone.
With that, if you’re in an institution where you don’t have trauma surgeons or people who are experienced with doing that, then maybe arthroplasty is a better option.
Another study identified patients who are high risk for failure with ORIF (Ricci et al. 2014). The authors report that failure commonly occurs in obese patients, those with diabetes, smokers, elevated BMI, and poor reconstruction techniques (19% non-union rate and 31% re-operation rate). If you categorize them into high-risk patients, the non-union rates and re-operation rates are quite higher.
Also, consider some common-sense considerations.
-
What if someone has bilateral fractures?
-
Are you going to make them non-weight bearing on both sides?
-
What if they’re old and have heart problems or unhealthy?
-
What if their knee is severely arthritic?
-
What if they have severe arthritis and they fracture the end of the femur?
-
Are you going to fix it and then do a total knee later (maybe not)?
Maybe you’re at a center that doesn’t have trauma expertise. For our institution, we’re fortunate to have a multidisciplinary team and try to utilize multidisciplinary discussion with our trauma colleagues. When you break all that down, I think when you have a patient with a distal femur fracture, you want to see if they have any of these conditions:
INDICATIONS FOR CONSIDERING DFR
-
Fracture Type
-
Medial Comminution
-
Segmental Bone Loss
-
Multi-Fragmentary Fractures
-
-
Conditions Associated with Non-Unions
-
Osteoporosis
-
Obesity
-
Anemia
-
Diabetes
-
Advanced Age
-
-
Other Considerations
-
Severe Knee OA
-
Bilateral Fractures
-
Polytrauma
-
Lack of Experienced Trauma Team
-
This may help to narrow down the patients you want to have the conversation with. The 2022 Australian registry has reported an increase of DFR over the last 15 years for fracture (Aebischer et al. 2022). The authors reported on 305 DFRs, with an average patient age of 76.4 years, which were predominately females (85.5%), with a 97% survival at five years, 88% survival at 10 years. However, infection and aseptic loosening were the most common reported reason for failure.
Similarly, in a reported medium-term (minimum 2-year follow-up), small series (n=30), in patients with an average age of 81 years, the authors showed good outcomes following DFR with a 7.4% complication rate, and one re-operation (Matar, Bloch, and James 2021).
In a recently published meta-analysis, the authors report that the re-operation and surgical complication percentages were similar between ORIF and DRF (Bundschuh et al. 2023). (Table 1)
In another study, total complications rates were also independently reported for ORIF (14.3%) and DRF (26.1%) (Ruder et al. 2017). This was an impactful study for me. We know that the mortality rates are high, and additionally, patients who are older tend to lose ability to ambulate especially when you compare the ability to walk later. Some studies compare reoperation or complications, but one thing that’s not talked about is how quickly the patients are up and walking.
If someone has a fracture, they may be non-walking for a prolonged period. In another study of ORIF versus DRF in patients greater than 70 years-old only, the authors showed that at one-year follow-up, 25% of the patients who had received ORIF were not ambulatory while 100% of the patients who had a DFR were ambulatory (Hart et al. 2017). If you treat an older patient with cardiac disease, getting them up and moving might impact mortality rates.
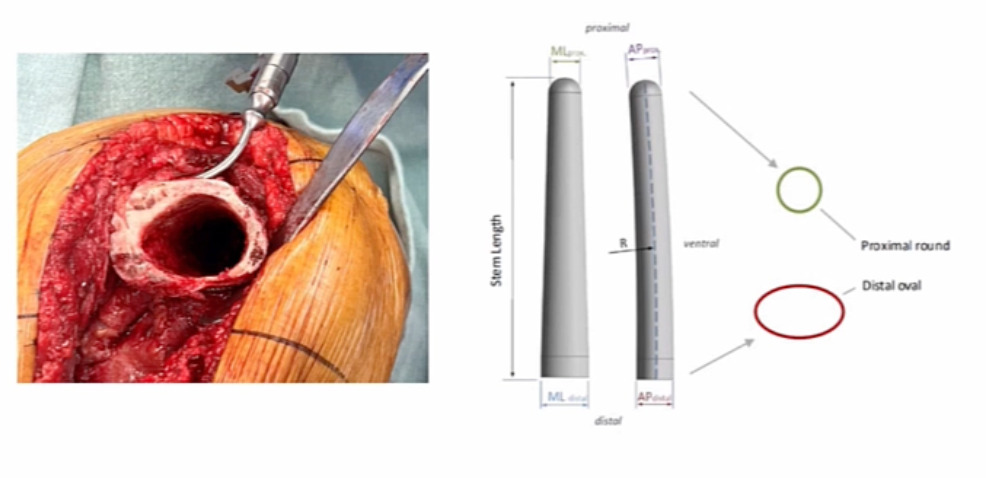
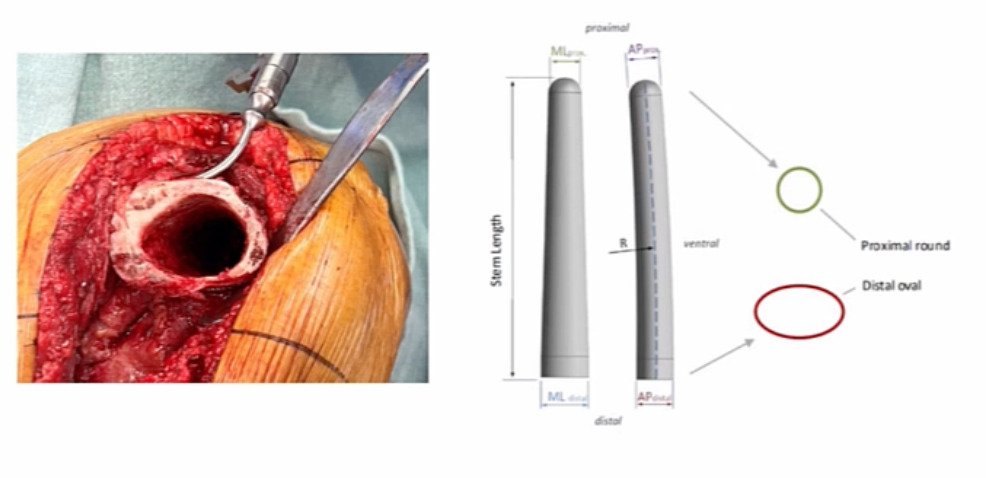
Dr. Gehrke and the ENDO-Klinik showed us that DFR can have challenges and hinges can have challenges (they can loosen) (Levent et al. 2021). If you don’t have good rotational control, they’ll spin out and loosen. However, we have solutions for that now. The OptiStem™ (Link Orthopedics, Hamburg, DE) is a newer option for us to help obtain rotational control for a number of these patients. Patients with a comminuted distal femur fracture, who’s osteoporotic, this may be a good option to help get more long-term fixation and a consistent result in the long run.
The following is a patient we cared for. (Figure 2) This was a revision setting, but you can see the end of the femur; the issue is rotational control. You can see the elliptical shape of the distal femur, and the morphology of the OptiStem on the right, and how that matches the normal anatomy of the femur for rotational control and hopefully, more long-term fixation integration.
Lastly, this is a unique case that we took care of at our institution. (Figure 3) This may have been on the aggressive side, but she had bilateral distal femur fractures and multiple medical comorbidities including severe heart disease and lung disease, which triggered a multidisciplinary team discussion and patient consultation. We had our trauma, joint replacement (me), physical therapy, and medical doctor as a team to advise the patient of all options and outcomes. We presented options for fixing versus replacing and ultimately the patient’s preference was to go for arthroplasty. We performed bilateral reconstructions using the OptiStem in this patient. She’s about six months out and doing well so far.

In summary (and with my Detroit background), I had to use a car reference. If you’re thinking ORIF or for a fixation, it’s more like a VW bug, but if you want to do a DFR, go with the Porsche.