


INTRODUCTION
It is well established that at least 50% of knees with severe osteoarthritis (OA) involve principally one of the three compartments of the knee, yet in the USA only about 4% of knee arthroplasties performed are unicondylar knee arthroplasty (UKA) (Mohammad et al. 2022).
I am a general orthopedist in practice 40 years, and for the last 25 years I have increasingly focused on perfecting and promoting a minimally invasive resurfacing UKA system that utilizes a muscle sparing incision, requires removal of a minimal amount of bone, and has an ease of recovery like arthroscopic knee surgery. In my practice, I perform approximately 70% UKA to 30% total knee arthroplasty (TKA). Collaborating with Dr. Peter Fennema (Advanced Medical Research, GmbH, Männedorf, CH), we published a 10-year minimum follow-up study of 344 patients (366 UKAs) that showed a 94.6 survival rate (95% CI: 90.9 – 96.8%), and with Forgotten Joint Score (FJS) and Oxford Knee Score (OKS) comparable to other UKAs using this method (Redish and Fennema 2018).
The purpose of this article is threefold:
-
Discuss why we aren’t doing more UKAs
- Especially in those patients >70 years with medical compartment disease
-
Share my experience gained and opinions from 25 years and roughly 5,000 UKAs
-
How UKA use, particularly with this surgical method, could possibly change practice patterns.
SO, WHY ARE UKAs UNDERUTILIZED?
There are a small percentage of surgeons who are “UKA Lovers” like me. We all wonder why more surgeons don’t do UKAs? I have spoken to countless surgeons about their feelings about UKAs, and it is surprising the negative reaction that I get when I ask about it. On the other hand, my patients often ask me, “why didn’t my other surgeon tell me about this?” Or “why isn’t everybody doing this procedure?” Is it for financial resons? I think not for the surgeons!
-
Reimbursement is not much different between UKA and TKA
-
Recovery and follow-up are much less time consuming with UKA
-
The UKA procedure is an excellent complement within the surgeon owned ASC
-
And contributes positively to the number of outpatients that can be done safely.
For the implant companies, the cost and time to manufacture and deliver a packaged and sterile TKA implant is significantly greater than a UKA, especially a low-cost, all-poly tibial implant like what I use. This is certainly a disincentive to promote a less expensive UKA system that could possibly “cannibalize” a more costly TKA and a “so-called” value added robotic system.
For surgeons, in my opinion, the “FEAR OF DOING HARM” is the principal reason to look for why not to do a UKA. In addition, and similarly to teaching good cement techniques, UKAs are rarely taught in fellowship programs. Moreover, since there is such a low volume of these cases in the US, surgeons fear being the “only kid on the block” performing and defending this procedure to their partners and local peer community.
I can best illustrate this point by describing my own first attempt to be a hero and do a UKA in my own practice.
Despite never seeing a UKA in my residency, I had a 47-year-old female with isolated bone on bone medial OA that I determined to be a good UKA candidate. I think every orthopedic surgeon toys with the idea of doing a UKA, and I had been to a conference where the use of UKA was debated. At that time, I was using a Whiteside TKA, non-cemented, with good success. Whiteside had a UKA, also non-cemented, utilizing a TKA incision, which was basically half of a TKA. I did the case without much difficulty and the x-rays looked good. She hurt like hell medially and was no better, if not worse with her original medial pain. It didn’t get better and after over one-year I was now faced with a difficult revision. Thus, my attempt to do something better had turned into something worse than if I had done a TKA to begin with, which no one would have criticized me for doing.
Moreover, I did a conversion of my unsuccessful first resection UKA utilizing a medial augment and long stem revision TKA, and at the same time did a resurfacing UKA (Repicci) on her other knee. She really did terrific with the resurfacing UKA!
BRIEF HISTORY OF RESURFACING UKA
I learned this technique in 2000 when Biomet and Dr. John Repicci were promoting resurfacing UKA on a large scale, and there was great enthusiasm for it (Repicci and Eberle 1999). The Repicci implant was widely used, but very poorly taught and supported following the large meetings promoting the procedure and device. Nonetheless, the reported results were mixed, and absolutely technique dependent. Four years later in 2024, Biomet all but abandoned promoting the Repicci UKA in favor of the Oxford mobile bearing UKA. There was a surge of UKA use during this period (reaching 12%) but it has died down over the last two decades to approximately 4% of all knee arthroplasty cases.
I have championed the resurfacing UKA system, developed new jigs and cutting tools, and taught this surgical technique which has made it an easily learned, accurate, and reproducible procedure (Freedom® Renew Knee, Maxx Orthopedics, Norristown, PA) (Figure 1). I have also worked with Biomet, Zimmer-Biomet, Mako (an assisted “Repicci operation” with the application of robotics and haptic guidance), and Maxx orthopedics. My goal all along has been to educate my colleagues and make them aware of performing numerous unnecessary TKAs in lieu of UKA, especially in the older age groups. A TKA is just that, a TOTAL knee, in which approximately 50% of the time one sacrifices two uninvolved knee compartments (Mohammad et al. 2022). In my experience (and other’s), minimally invasive resurfacing UKA recovery has been compared to that of arthroscopy.

RESECTION VS RESURFACING
I think of UKAs as either:
-
A RESECTION procedure (which includes most performed today)
-
Or a RESURFACING procedure (like I prefer)
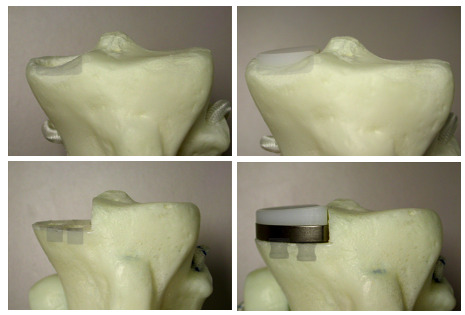
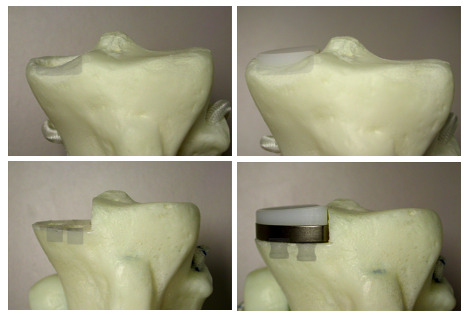
A resection UKA requires a flat saw cut of the tibia and chamfer cuts of the distal femur. A resurfacing UKA utilizes high speed burrs and rasps to remove minimal bone or “patch” the surface of the femur and create a pocket in the surface of the tibial plateau for containing an all-poly wafer-surface inlaid. (Figure 2)
Resection UKA
A resection UKA is basically half a TKA. The surgical approach involves at least subluxation if not dislocation of the patella laterally. For lateral unis some surgeons perform a TKA medial approach, others make a lateral incision.
-
A tibial sawcut is made, taking care to get proper posterior slope and coronal alignment, with the help of either external guides or robotics.
-
A femoral distal sawcut is made, as the femoral component must be at least 6 mm thick to avoid failure at the sharp corners of the femoral component.
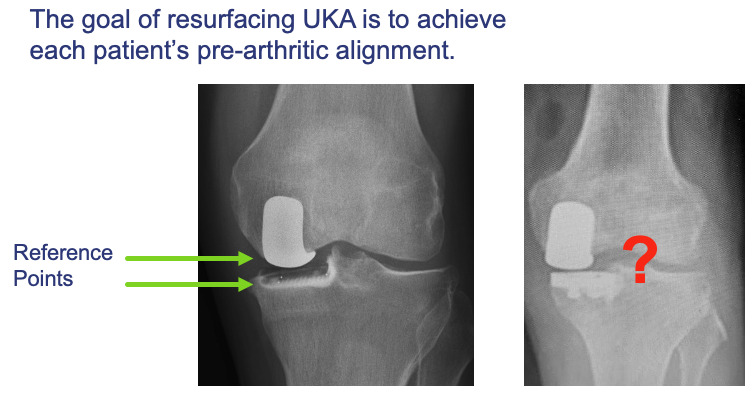
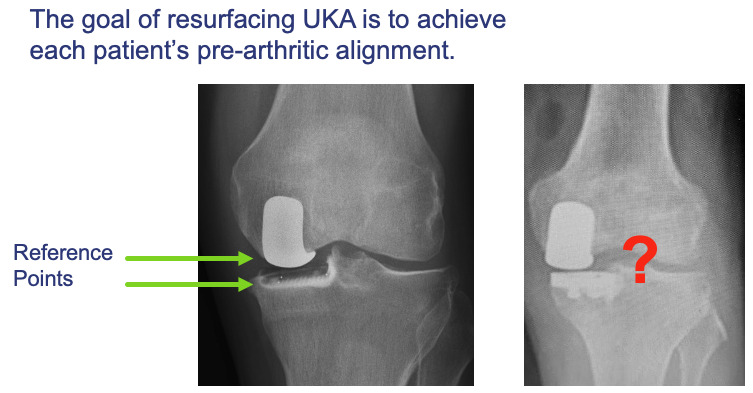
NOTE: Both tibial and femoral bone cuts remove the native surface reference points and knee balancing requires subjective “feel” or robotic references (fit the patient to the component). (Figure 3)
-
Proper knee alignment and ligament balance is determined using spacer blocks and achieved depending on the “feel” of ligamentous stability, tension or laxity, with or without the help of robotics.
-
Most fixed bearing UKAs are resection, utilizing a 6mm femoral components that matches with chamfer cuts and two pegs using a 2 mm metal baseplate with two pegs antero-medially and a keel posterolaterally.
-
The modular polyethylene wafer of varying thicknesses is locked into the metal baseplate.
Resurfacing UKA
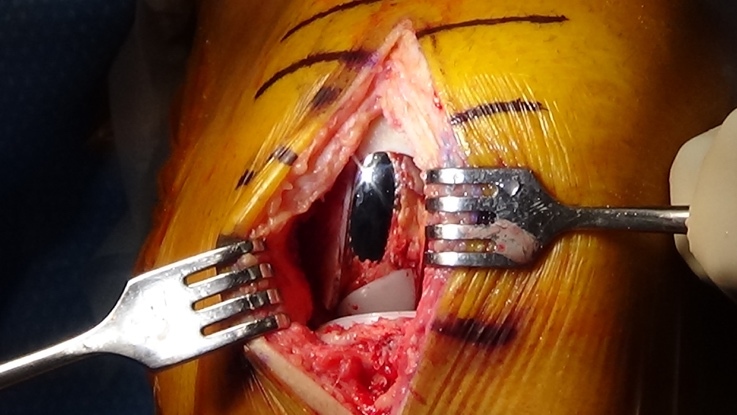
A resurfacing UKA utilizes a short, muscle-sparing 3 to 4-inch incision with no need for patellar subluxation. The all-poly wafer is inlayed into a “pocket” within the tibial plateau, preserving a peripheral ring of cortical bone and retaining tibial surface reference.
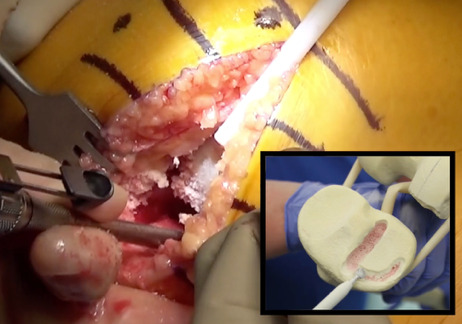
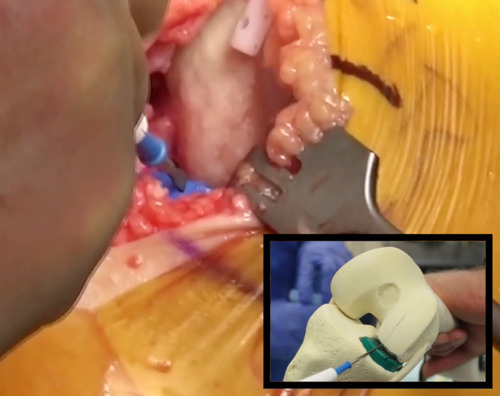
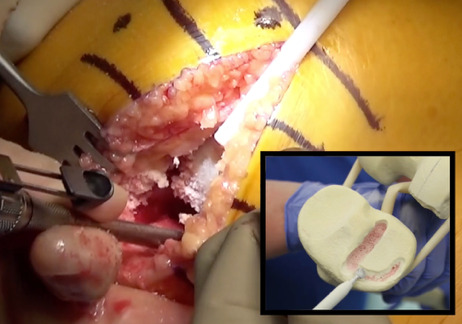
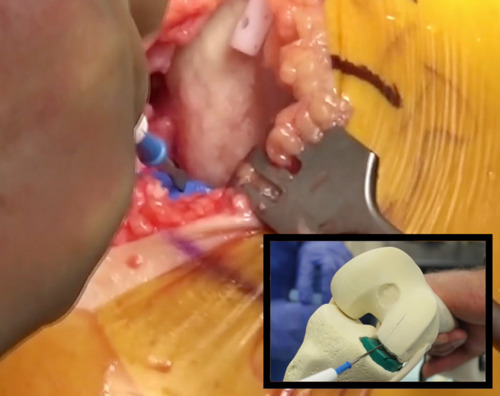
- The “pocket” for the inlay is created with a high-speed burr to outline and “rough in” the D shape and decorticate the surface inside the “D.” (Figure 4)
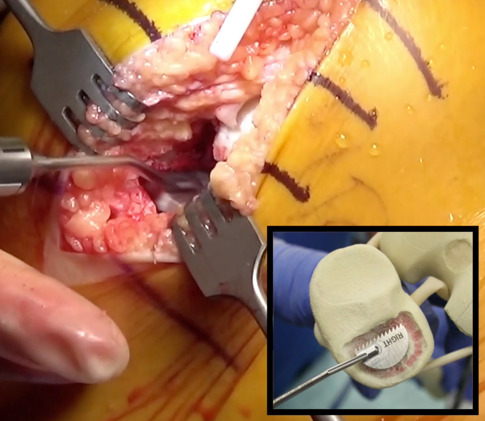
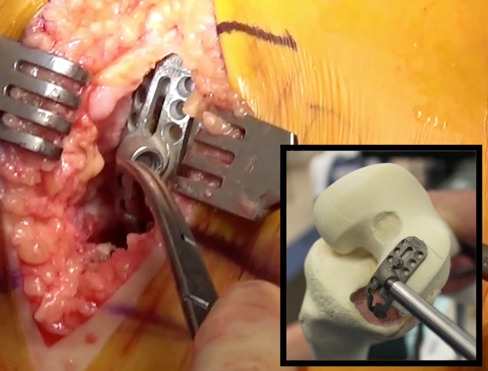
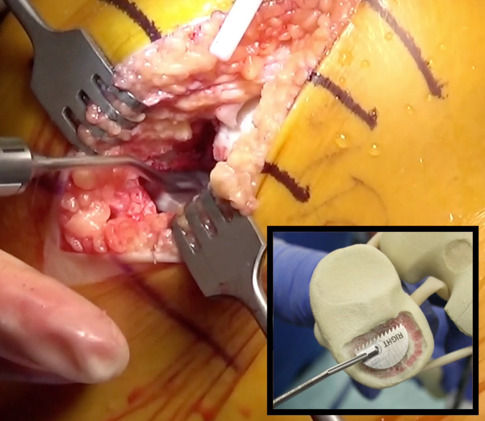
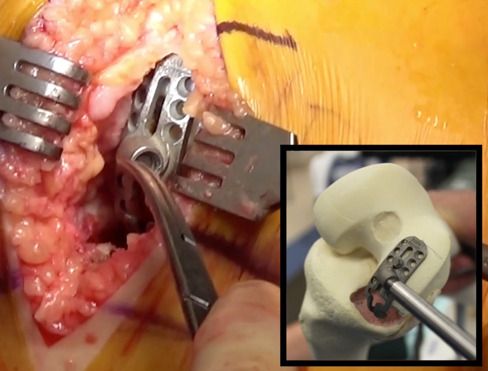
- A “D” shaped offset oscillating rasp then flattens out the surface of the pocket, and the largest size implant trial is placed. (Figure 5)
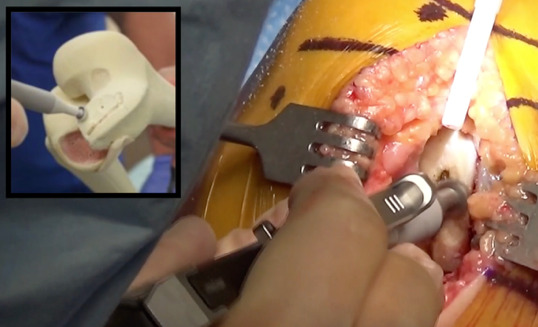
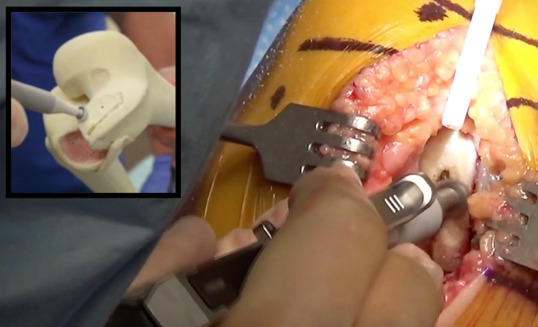
- A groove in the trial sits roughly in the middle into which a Bovie is placed. With flexion and extension of the knee a Bovie line is made in the femoral condyle, which will become the midportion of the femoral component. (Figure 6)
- Using a jig sited on this Bovie line, a parallel groove is made corresponding to the medial border of the femoral component. (Figure 7)
- The cortex is then burred away from the medial border to the notch but the bone medial to site of the implant is preserved, which is native joint line. (Figure 8)
- Knee alignment is achieved by simply observing how proud the trial implants sit and adding the proper amount of thickness to the native joint line, with the intent of returning the knee to the pre-disease native alignment. No dependence on the subjective feel of ligamentous laxity is needed, nor are spacer blocks or robotics to achieve knee balance.
The patient’s pre-diseased joint line is restored which optimizes their natural ligament tension and joint alignment (fit the component to the patient). (Figures 3, 9-10)

THE INLAYED TIBIAL COMPONENT
In an arthritic knee the subchondral bone can be very dense, whereas the density of this bone diminishes 50% at 1 cm under the joint surface. Preserving this strong and dense bone is the key to the success of the inlay (Thompson et al. 2010). Proper technique of cementation increases the depth of penetration to further support the implant. Loosening of an inlaid tibial component is extremely rare.
Surgeons can’t help but be concerned that an inlay with no cortical support will subside. In my experience actual subsidence was only seen once in the large cohort of patients that was studied, and that in a 320-pound male who was up to 370 pounds 4 years after his surgery. Through my 25 years of experience, I have seen an incidence of subsidence that I would estimate at maybe < 0.5 percent. Having medial pain under the implant that persists to the point of subsequent surgery has happened at a rate of 1-2 %, and many of these were converted to an on-lay tibial component, which continues to maintain the native soft-tissue envelope (and can also be done after subsidence).
WHAT HAPPENS IF A UKA FAILS?
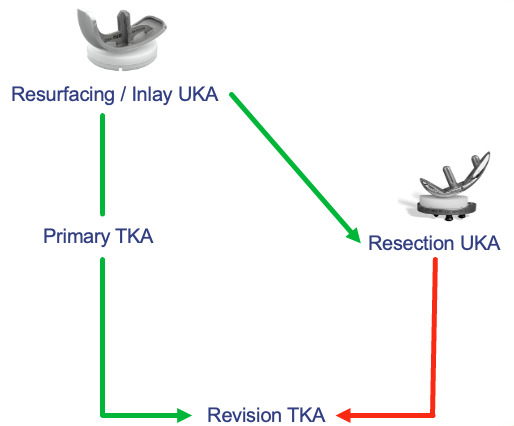
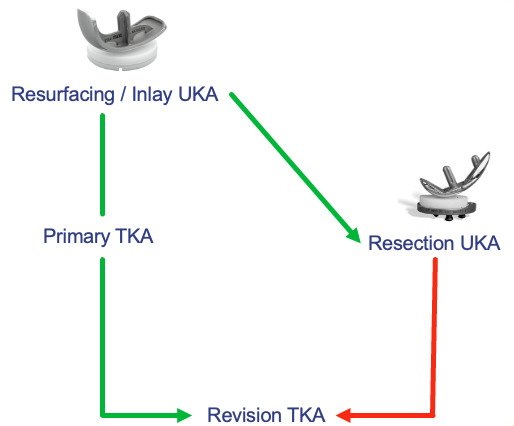
A RESECTION UKA has the initial medial baseplate positioned like that of a TKA and may require block augments and a stem in the revision. It has been recommended that a resection UKA not be revised to another UKA. Resection compromises bone that would be used for a primary TKA, most studies show the results of converted resection UKA to TKA fall somewhere between result of primary TKA and revision TKA, with the majority requiring stems and/or augments. (Figure 11)
A true RESURFACING UKA utilizes a 6.5 mm all poly, cemented inlay, and can be easily revised to a resection UKA. Also, since the depth of the tibial insert plus cement is less than the standard thickness of a primary TKA tibial component baseplate plus insert, a resurfacing UKA can be easily converted to a standard primary TKA without augments or long stems. (Figure 11)
When disease progression to the opposite compartment following either UKA does occur, a second UKA can be placed in the opposite weight bearing compartment for a “Bi-UKA” (still retaining the cruciate ligaments).
BROADENING THE INDICATIONS BY CHANGING THE ALGORITHM
Let’s examine the decision-making process in three groups of patients with unicondylar OA. Let’s say the need for a revision TKA in the patient’s lifetime is the result to avoid.
-
Under 55: Any procedure may need to be revised. Reasons to do a UKA are to have a more natural feel, decrease recovery time in a working population, and preserve bone stock for future surgeries. Resurfacing allows more options if a second surgery is needed.
-
55-69: A total knee has a decent chance of lasting, and in higher BMI individuals especially, there are valid reasons to do TKA. A UKA of any kind has not been proven to be as durable as TKA. So, if UKA is chosen, it should be easily revisable. With resurfacing, a failure of the tibial component can be revised successfully from inlay to onlay. (Figure 11)
-
>70: A successful UKA of any kind will most likely will be the last surgery needed. In the over 80 group, the ease of recovery and safety of the resurfacing UKA becomes important. In general, elderly patients require more rapid rehabilitation and the lowest possible intraoperative and postoperative morbidity as well as mortality.
IN SUMMARY
Minimally invasive resurfacing UKA has been shown to yield results comparable to that of other fixed bearing UKAs, with a high survival rate beyond 10-years (Mohammad et al. 2022; Redish and Fennema 2018). The inlayed tibial component preserves good bone in the subchondral area by removing minimal thickness of bone. The native joint surfaces of both tibia and femur are preserved, making proper knee alignment easy to achieve for each patient regardless of their native ligamentous laxity. Using this technique greatly reduces the surgeon’s fear of doing harm, and the result is a desire to look for reasons to do more UKAs instead of looking for reasons not to.