Introduction
Thumb carpometacarpal (tCMC) osteoarthritis is a common degenerative condition that affects millions globally every year (Sodha et al. 2005; Wilder, Barrett, and Farina 2006). The prevalence of tCMC arthritis climbs with age and has a prevalence of over 90% in people over the age of 80 (Sodha et al. 2005). Thumb CMC arthritis can be particularly debilitating and lead to significant pain and loss of hand function for those affected, especially as symptoms continue to progress over time (Higgenbotham et al. 2017). With an aging population in the United States, the prevalence of tCMC arthritis and the need for treatment will likely grow over the next decade. Understanding the pathoanatomy and treatment of tCMC arthritis is essential to provide effective care.
The tCMC joint is a saddle-shaped articulation between the trapezium and the first metacarpal of the hand. This small joint has a non-normalized mean average articular space volume of 104.02 mm3 for females and 138.6 mm3 for males (Shih, Mainprize, and Binhammer 2018). The tCMC joint assists with pinching strength and prehension of large objects in the palm (Ladd, Weiss, Crisco, et al. 2013). The anterior oblique ligament maintains primary stabilization of the tCMC joint, but the tCMC joint is also stabilized by the dorsal radial ligaments (Higgenbotham et al. 2017). Thumb function is essential for normal upper extremity function, with one study showing that thumb impairment can lead to as much as a 50% upper extremity impairment rating due to an inability to grasp and maneuver objects (Ladd, Weiss, Crisco, et al. 2013).
Thumb CMC arthritis can be treated through conservative and surgical modalities. The most common non-operative management of thumb CMC arthritis includes activity modification, orthotic usage, non-steroidal anti-inflammatory medications (NSAIDs), therapy, and intra-articular injections (O’Shaughnessy and Rizzo 2022; Billig et al. 2021). Injections remain an effective form of conservative management and can be helpful for many patients (Katt et al. 2022; Fowler, Swindells, and Burke 2015). Surgical management for tCMC arthritis often includes trapeziectomy with or without ligamentous reconstruction and tendon interposition or arthrodesis (Challoumas et al. 2022).
Injections remain a standard and effective management option for tCMC arthritis, with intra-articular injections being much more effective than extra-articular injections (Fowler, Swindells, and Burke 2015). The small size of the tCMC joint makes injections technically challenging, and it makes the success of the injection dependent on a host of factors, including the volume of joint space and physician expertise (Gershkovich, Boyadjian, and Conti Mica 2021). Many physicians utilize traditional anatomic palpation techniques for injections, while others have opted for intra-articular image-guided injections (IGI) using either ultrasound or fluoroscopy (Saha, Smith, and Hasan 2023). Currently, there is no consensus regarding which injection method most accurately and effectively guides the injection to the correct intra-articular anatomic location. This study aims to perform a systematic review to determine whether intra-articular IGI or anatomic landmark injections (ALI) are more accurate, more effective, and whether cost differences exist between the two. We hypothesize that there will be an improvement in both the clinical efficacy and accuracy with the use of intra-articular IGI compared to ALI of the tCMC joint.
Methods
Study Design
This systematic review followed the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) statement standards (Page, McKenzie, Bossuyt, et al. 2021).
Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria: 1.) Evaluated a comparison of the accuracy or efficacy of anatomic landmark-based versus image-guided CMC injections 2.) Were conducted in either human or cadaveric subjects, 3.) The manuscript was completed in English, 4.) Studies were completed on or after January 1, 2000. Reviews, commentaries, letters to the editor, technique papers, and surveys were excluded.
Search Strategy
PubMed/MEDLINE, Cochrane, and Embase databases were systematically searched for publications from January 1, 2000 to June 18, 2024. Comprehensive search strategies were developed using keywords, MeSH terms, and synonymous terms. The PubMed/Medline search was adapted to the Cochrane and Embase databases. See supplementary table 1 for a complete Pubmed Search.
One author (T.B.P.) performed the search. Three authors (T.B.P., C.R.M., V.M.D.) excluded irrelevant articles and duplicates based on title and abstract. The remaining articles underwent an independent full-text review by three authors (T.B.P., C.R.M., V.M.D.) and were assessed for eligibility based on established criteria. Any conflicts were resolved by discussion among the three authors.
Data Extraction
The study’s demographic information was collected, including the lead author and country of origin, study design and level of evidence, study type, number of patients, database used, and study follow-up length. Study results and comparisons for the following information were included: study comparison, injection type, osteoarthritis classification (if applicable), and study results.
Statistical Analysis
Statistical analysis was not performed due to a lack of level 1 evidence studies.
Results
PRISMA Flow Diagram
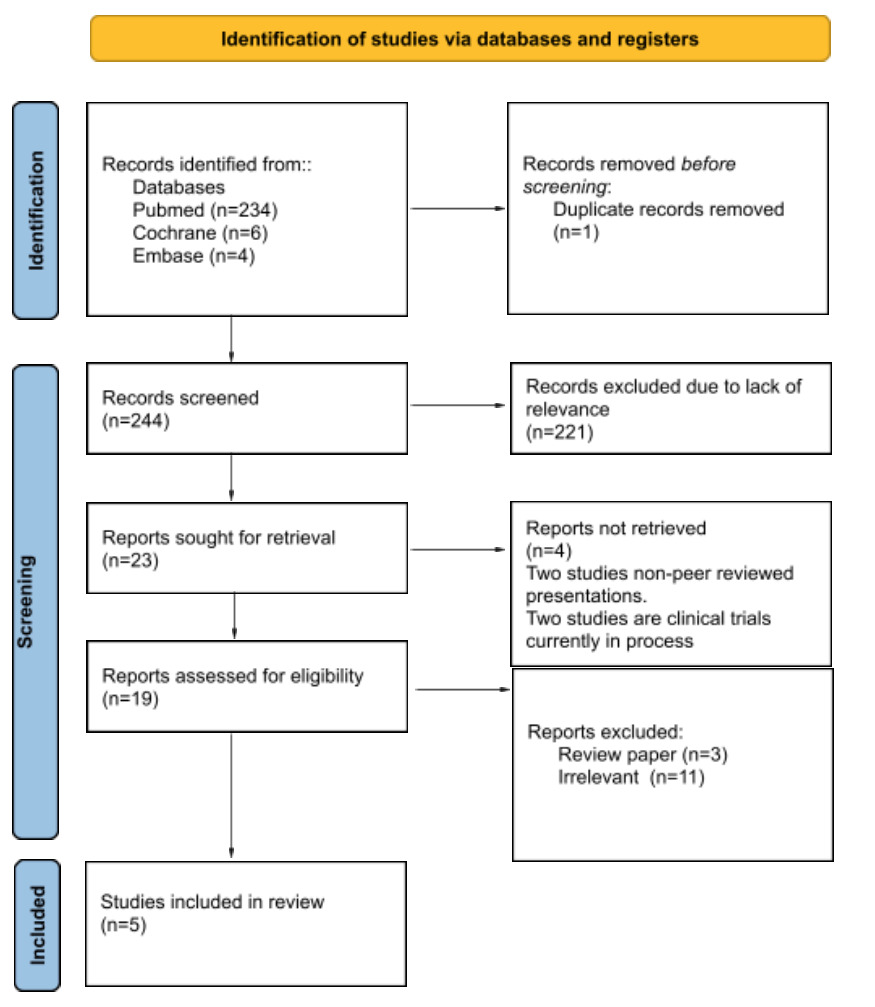
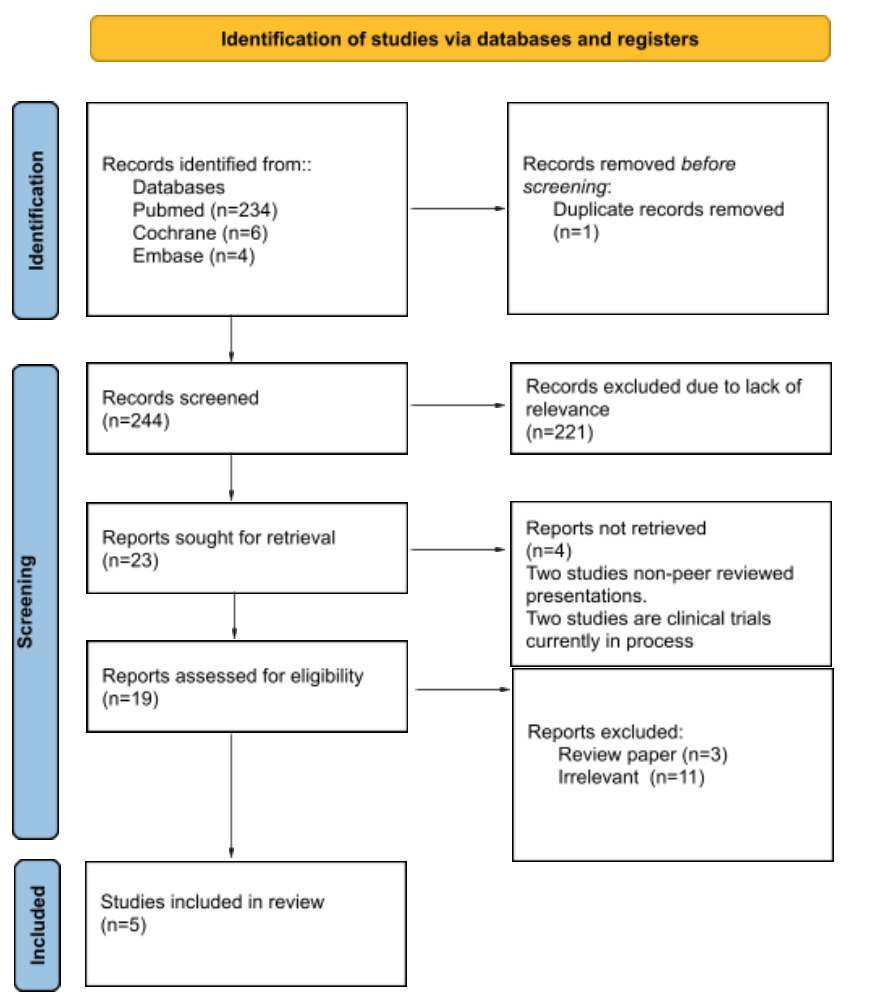
A preliminary search of three databases provided 245 studies. One duplicate was removed. 244 abstracts and titles were screened, and 221 were removed for lack of relevance. 23 reports were sought for retrieval. Five studies met the final inclusion criteria and were included in this study. See Figure 1.
Study Demographics
Al-Nokatha et al (Al-Nokhatha et al. 2023). was a level II evidence prospective cohort study out of Ireland with 33 patients. The follow-up length for this study was 12 weeks. This study used the Australian Canadian Osteoarthritis Hand Index (AUSCAN), the Visual Analog Score scale (VAS) for pain, and the 10-point scale for pain, stiffness, and hand function to compare ultrasound IGI versus ALI. Gershkovich et al (Gershkovich, Boyadjian, and Conti Mica 2021). was a level III evidence retrospective cohort study of 62,333 patients that evaluated intra-articular IGI (fluoroscopy or ultrasound) against ALI (Gershkovich, Boyadjian, and Conti Mica 2021). This study used the Truven Health Marketscan Research Databases between 2003 and 2014. Derian et al (Derian et al. 2018). was a cadaveric-based level V evidence study of 36 cadaveric samples that compared the accuracy of ultrasound versus ALI. This study used injections with dye and subsequent dissection to evaluate dye levels within the tCMC joint. Pollard et al (Pollard et al. 2007). was a cadaveric-based level V evidence study of 30 cadaveric samples that compared the accuracy of fluoroscopy IGI versus ALI. This study used radio-opaque dye for their injections, and accuracy was evaluated by using fluoroscopy to determine location of dye. To et al (To, McClary, Sinclair, et al. 2017). was a cadaveric-based level V evidence study of 40 cadaveric samples that compared ultrasound accuracy versus ALI. This study used dye and evaluated accuracy of the ultrasound or ALI with both fluoroscopy and anatomic dissection. See Table 1.
Both human participant studies had a higher percentage of females than males and a similar mean age of participants. Al-Nokotha et al. listed participants’ handedness, while Gershkovich et al. did not. The percentage of smokers was higher in Al-Nokotha et al (Al-Nokhatha et al. 2023). (27% vs 3%). See Table 2.
Study Results and Comparisons
Al-Nokatha et al (Al-Nokhatha et al. 2023). compared ultrasound versus ALI for patients with Eaton-Littler stage 2 or later. They injected 20 mg of methylprednisolone acetate and 0.5 mL of 1% lidocaine for all patients. 33 patients with a mean age of 63 years old were included, however, methodology did not specify how the groups were selected. Both groups showed statistically significant improvement over baseline at 6 and 12 weeks for Australian Canadian Osteoarthritis Hand Index (AUSCAN) scores. There was no statistically significant difference between the ultrasound or ALI groups for baseline Visual Analog Scores. There was no statistically significant difference between groups for pain, stiffness, or hand function at baseline to 6 weeks or 6 to 12 weeks.
Gershkovich et al (Gershkovich, Boyadjian, and Conti Mica 2021). utilized a large database to compare intra-articular IGI (fluoroscopy or ultrasound) versus ALI. 62,333 total study patients who underwent a thumb CMC injection with a mean age of 59.7 years old were included. When comparing intra-articular IGI versus ALI, the average number of days between a patient’s first injection and the time to a second injection was not statistically significant (237.3 days vs 266.7 days). 89.5% of participants in the ALI group did not go onto surgery, 72.2% of participants in the ultrasound group did not go onto surgery, and 82.9% of participants in the fluoroscopy group did not go onto surgery. A statistically significant difference of days from injection to surgery was found between the ultrasound and ALI, but this difference was only 14 days on average. The cost of ALI was 203 dollars less than intra-articular ultrasound-guided injections.
Derian et al (Derian et al. 2018). and To et al (To, McClary, Sinclair, et al. 2017). showed no statistically significant difference in intra-articular ultrasound accuracy versus anatomic landmark cadaver injections to the tCMC joint. Pollard et al (Pollard et al. 2007). showed that intra-articular fluoroscopic guided injections had 100% needle accuracy placement. However, there was no statistically significant difference when compared with ALI. See Table 3.
Discussion
Minimal clinical differences exist between intra-articular IGI and ALI of the tCMC joint. Pain, stiffness, functional scores, and timing for repeat injection did not differ between the two groups (Al-Nokhatha et al. 2023). There was no statistical difference in the accuracy of fluoroscopy or ultrasound-guided injections compared to traditional ALI (Derian et al. 2018; Pollard et al. 2007; To, McClary, Sinclair, et al. 2017). While no statistical difference exists, there does remain some concern that clinical accuracy may be significantly reduced by not using image guidance with wide differences in accuracy. The primary difference between IGI and ALI found in this review is cost. ALI cost less, with an average of 203 dollars less per injection than image guided ultrasound injections (Gershkovich, Boyadjian, and Conti Mica 2021). ALI were, therefore, found to be equally accurate, equally effective, and cost less when compared with image-guided injections.
One possible reason for the lack of a significant clinical difference in outcomes between IGI and ALI may be the superficial nature of the tCMC joint and the ability to easily palpate the joint in most patients. Nevertheless, due to the small size of the tCMC joint, injections are commonly performed with image-guidance. However, the present study suggests that this may be unnecessary, as several studies showed no difference between the accuracy of intra-articular IGI and ALI. A study by Mandl et al., also argues that tCMC injections can be accurately be performed in the office setting, based upon their testing of hylan G-F 20. This study recommends that imaging is not needed to perform these injections (Mandl et al. 2006). Additionally, IGI are only as effective as the physician’s skill with imaging (Saha, Smith, and Hasan 2023). Ultrasound, in particular, requires a significant learning curve (Sites et al. 2004; Barrington et al. 2012). Similarly, fluoroscopic injections may also take considerable time to master (Dias, Alves Junior, and Abdala 2017). However, early ultrasound studies such as by Umphrey et al., maintain that ultrasound imaging can produce high accuracy, and can be a successful alternative to fluoroscopy (Umphrey et al. 2008).
One important consideration of these procedures is the financial burden incurred. Gershkovich et al. showed that ultrasound injections were on average $203 more expensive than ALI (Gershkovich, Boyadjian, and Conti Mica 2021). Higher costs have been shown to increase health disparities in underserved populations, as these populations may be unable to afford additional costs (Frazier, Lopez, Islam, et al. 2023). Physicians should consider the cost increases associated with IGI and the potential consequences of those increases to their patients. While the costs may seem minimal in the overall healthcare spending across the country, it may be significant for individual patients.
The quantity of evidence regarding any potential benefits of tCMC intra-articular IGI remains very limited, and to our knowledge no level 1 studies exist comparing IGI to ALI. As imaging technology improves prospective studies can be done to determine if we can better optimize the accuracy and efficacy of intra-articular IGI. More prospective studies should also evaluate the costs of IGI.
Limitations
The most significant limitation of this study is the lack of multiple high-level evidence studies evaluating this association. This limitation is created by the limited available literature comparing these injections. Large prospective or retrospective trials could be conducted to compare IGI versus ALI. The second limitation of this study is the potential for missed literature. While our search was comprehensive and searched three major literature databases, literature in another language or a different database may exist. Future studies are needed to help physicians determine the most effective route of injection. A third limitation in this study is the limited number of studies for statistical meta-analysis to compare the current treatment methods. Future studies can aim to complete meta-analysis as additional literature becomes available, and create grouped comparisons. A fourth limitation is the lack of evaluation of complications by the current studies when using the treatment methods. This could provide significant insight into the outcomes of treatment as well. A fifth limitations is that studies do not have standardized methods for evaluating accuracy of needle placement, and several different methods are used. Standardized approaches across studies would improve the comparisons across studies. A final limitation in this study is that the retrospective studies limit the evaluation of provider or physician injector experience, as this could play a significant role in overall accuracy. Future studies should clearly provide this information.
Conclusions
While the current literature on this topic is limited, the current literature appears to show no significant difference between the accuracy or efficacy of intra-articular IGI and ALI. ALI injections appear to be a more cost-effective option without sacrificing outcome. These results also highlight that intra-articular placement may not be necessary for injection benefit, and future research and larger studies can be beneficial to improve comparisons and outcomes.
Ethical Approval
This study was determined to be exempt or excluded from Institutional Review Board
(IRB) oversight in accordance with current regulations and institutional policy. .
Funding
No funding was provided for this research.
HCA Healthcare Disclaimer
This research was supported (in whole or part) by HCA Healthcare and/ or an HCA Healthcare-affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any affiliated entities.
Disclosures
Dr. John T. Riehl, M.D. is a consultant for and receives royalties from Arthrex Inc. For the remaining authors, no potential conflicts of interest to disclosure.