INTRODUCTION
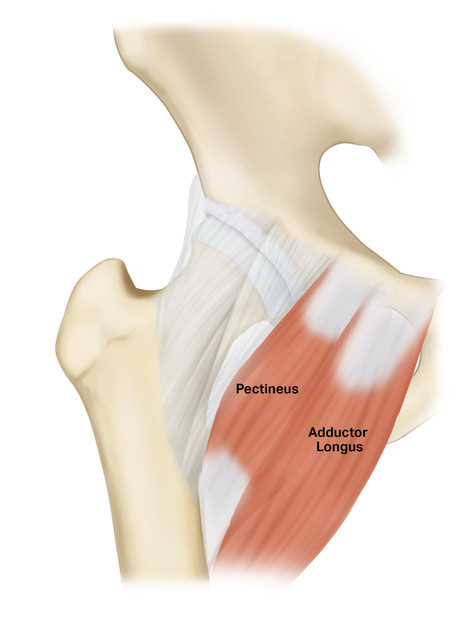
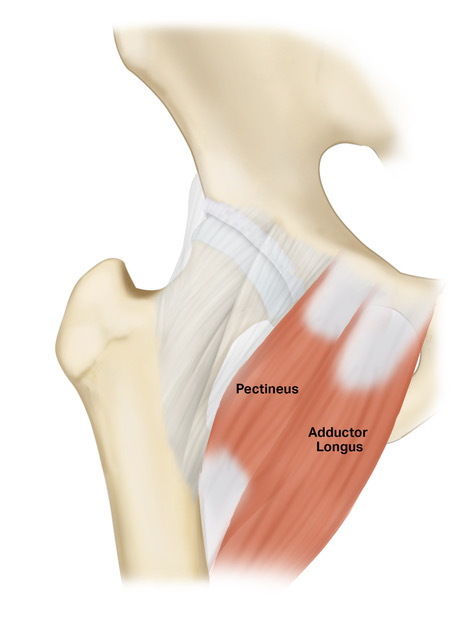
Adductor-related groin pain is a common injury among athletes and represents a significant source of morbidity within this population (Pizzari, Coburn, and Crow 2008). This is particularly common in athletes engaged in sports that require abrupt changes in direction and kicking, such as polo, soccer and hockey (Weir, Brukner, Delahunt, et al. 2015; Ramazzina et al. 2019). The yearly incidence of groin injuries in male soccer players, for instance, ranges from 10% to 18%, resulting in substantial time lost from sports participation and a majority of injuries in the study (68%) were adductor related (Mosler, Weir, Eirale, et al. 2018). The primary association with adductor-related groin pain is adductor tendinopathy, predominantly affecting the adductor longus, representing one of the various etiologies of groin pain syndrome (Figure 1) (Pesquer et al. 2015). Adductor tendinopathy can be both acute and chronic, with acute injuries generally presenting at less than or equal to 5 weeks from injury and chronic injuries presenting greater than 5 weeks from injury. To effectively manage groin pain, an accurate diagnosis is essential. This requires the exclusion of alternative conditions, including inguinal or femoral hernia, bursitis, osteoarthritis, stress fractures, or femoroacetabular impingement which can generally be determined based on history, exam, and advanced imaging findings (Sheen, Stephenson, Lloyd, et al. 2014). Adductor tendinopathy typically manifests with pain at the insertion site of adductor longus and pain with adduction of the leg against resistance (Forlizzi et al. 2023).
Conservative management is typically the first line treatment for adductor tendinopathy. However, up to 10% of patients do not adequately respond to conservative treatment and are indicated for surgical intervention (Hölmich, Uhrskou, Ulnits, et al. 1999; Schilders et al. 2013; Mehin et al. 2006). Conservative measures include physiotherapy, non-steroidal anti-inflammatories (NSAIDs), and minimally invasive procedures, such as steroid or biologic injections (Schilders et al. 2009). The most commonly utilized biologic is platelet rich plasma (PRP) (Unlu et al. 2017; Dallaudière, Pesquer, Meyer, et al. 2014). However, there are few higher level studies highlighting PRP or other biologics and their potential benefits for adductor tendinopathy. Surgical interventions, on the other hand, may include adductor tenotomy or adductor release (Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012). While previous reviews have investigated the efficacy of both conservative and surgical approaches in managing adductor tendinopathy, with a primary focus on return-to-sport rates and resumption of daily activities, these reviews have not provided comprehensive assessments of outcome measures, complication rates, or the impact of injury chronicity (King et al. 2015; Paajanen et al. 2015).
Therefore, the purpose of this study was to systematically evaluate outcomes and complications of different treatment modalities for adductor tendinopathy (conservative or surgical approaches) with a specific focus on return-to-sport (RTS) rate in acute and chronic injuries. We hypothesized that both conservative and surgical treatment, when indicated, would lead to improved clinical and functional outcomes, allowing patients to return to sports at their pre-injury level.
METHODS
Search Strategy and Study Selection
A literature search was conducted in adherence to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Page, McKenzie, Bossuyt, et al. 2021). A database search was executed, encompassing PubMed, Embase, and CENTRAL databases for studies reporting on the treatment of chronic or acute adductor tendinopathy with data retrieval up to September 18, 2023. The search criteria included “(adductor OR “adductor longus”) AND (tendinopathy OR tendinitis OR groin) AND (athlete* OR sport*) AND (treatment OR management OR rehabilitation OR surgical OR conservative OR tenotomy OR repair OR release) AND (outcome* OR “return to sport” OR “return to play”)”. The inclusion criteria was limited to studies reporting on patients who were 18 years of age and older, who experienced chronic or acute adductor tendinopathy, and discussed treatment modalities such as conservative treatment including intra-articular injections and physical therapy, or surgical interventions. Articles published in English or Spanish were included, while cadaveric, animal, and biomechanical studies were excluded. Additionally, case reports, systematic reviews, meta-analyses, expert opinions, and technique papers were also excluded from the analysis.
Two independent reviewers (initials blinded for review) assessed article eligibility based on their titles and abstracts. In situations where abstracts did not provide adequate information to make an eligibility determination, a thorough examination of the complete text was undertaken. Any disparities or uncertainties arising between the reviewers were thoughtfully deliberated upon through the participation of a third author (initials blinded for review). Subsequently, a full-text evaluation of the included articles was carried out for data extraction.
Data Extraction
Data was extracted from the relevant studies and entered into a Microsoft Excel spreadsheet (version 16.63; Microsoft, Redmond, WA) for analysis. Extracted data included the first author’s name, publication year, level of evidence, type of study, patient demographic characteristics, mean follow-up time, sport played by patients and level of sport (recreational or competitive), and injury characteristics such as laterality, chronicity, and etiology. Information pertaining to treatment such as conservative or surgical management, use of intra-articular injections, surgical approach, and rehabilitation protocols was also collected. Chronicity was established by considering the duration of symptoms prior to initiating treatment, spanning from 4 to 20.4 weeks. Finally, data pertaining to clinical outcome scores, return-to-play rates, and complications were also registered. The selected articles were not blinded regarding author, affiliation, or source.
Risk of Bias Assessment
To appraise potential biases in the included studies, two authors (initials blinded for review) independently conducted a methodological quality assessment employing the Methodological Index for Non-Randomized Studies (MINORS) criteria. Any discrepancies encountered during this evaluation were resolved with the input of a third investigator (initials blinded for review).
The MINORS Criteria is a numerical scale featuring eight areas tailored for noncomparative, nonrandomized studies and twelve inquiries designed for comparative, non-randomized studies (Slim et al. 2003). The maximum score is 15 for a comparative study and 12 for a noncomparative study (Slim et al. 2003).
Statistical Analysis
Data pooling was avoided due to increased level of heterogeneity, high risk of bias, and lower level of evidence of the included studies. However, a weighted calculation of means was used to analyze mean age, follow-up time, and the percentage of athletes returning to sport.
RESULTS
Literature search
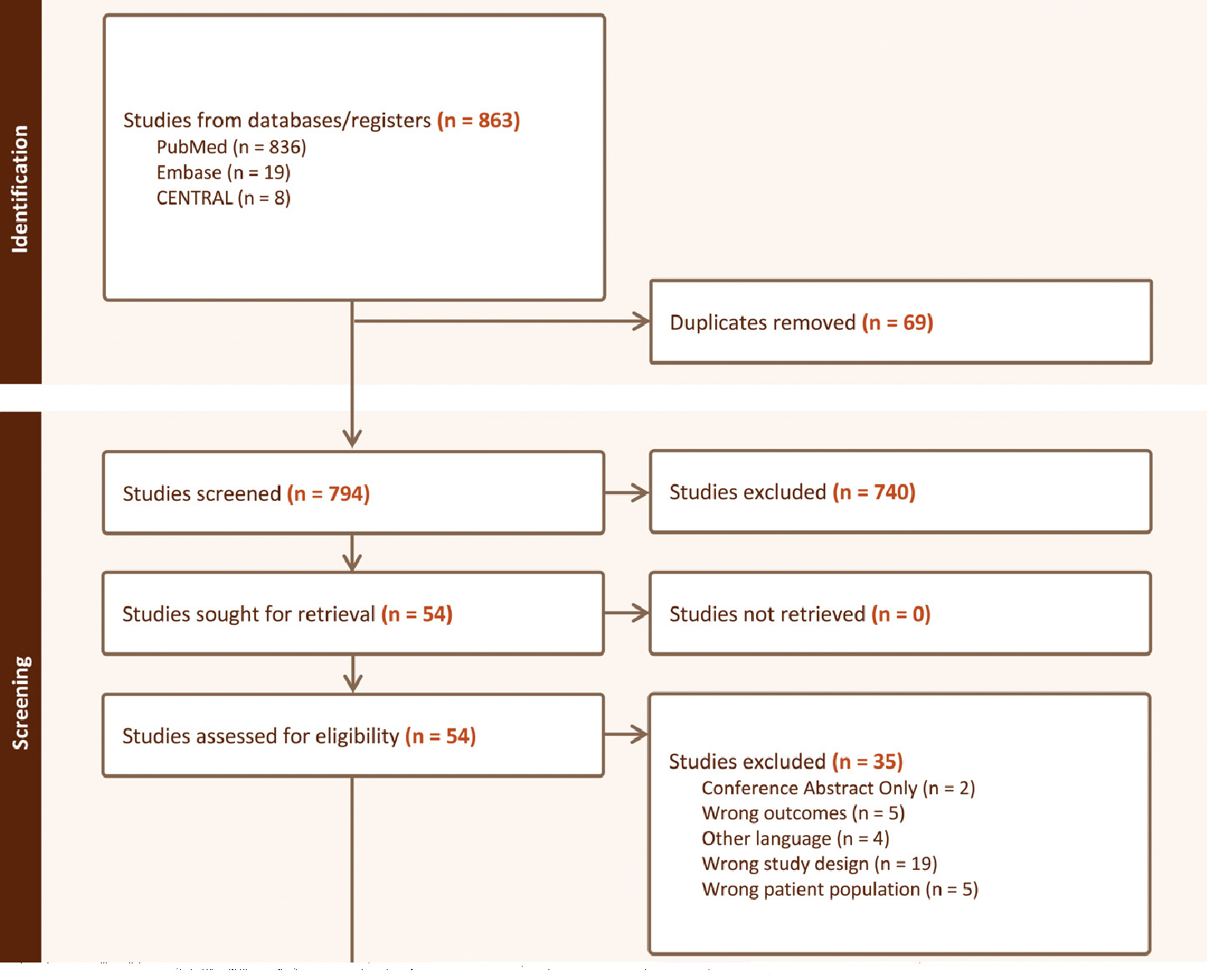
A total of 794 relevant articles were initially identified according to the search strategy. Fifty-four full-text articles were assessed for eligibility, and ultimately nineteen studies were included (Figure 2) (Schilders et al. 2013; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Moreno et al. 2017; Dojčinović et al. 2012; Robertson et al. 2011; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Serner et al. 2021; Bharam et al. 2018; Ueblacker, English, and Mueller-Wohlfahrt 2016; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013; Weir et al. 2011). Among the included studies, all were clinical studies including three randomized control trials (15.8%), thirteen case series studies (68.4%), two prospective studies (10.5%), and one retrospective case-control study (5.3%). One level of evidence I study (5.3%), two level of evidence II studies (10.5%), three level of evidence III studies (15.8%), and thirteen level of evidence IV studies (68.4%) were included (Table 1).

All studies were published between 2005 and 2021, with 68.4% of studies being published between 2013 and 2021. The mean MINORS score was 13.6 (range, 12-15) for the six included comparative studies, demonstrating low quality, and 8.3 (range, 5-12) for the thirteen non-comparative studies, demonstrating low quality (Figure 3).
Demographics
A total of 730 patients, 695 male and 35 female, were included within the 19 studies. The mean patient age was 25.6 years (range, 22-39 years). The mean follow-up time, reported in 18 studies (Schilders et al. 2013; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Moreno et al. 2017; Dojčinović et al. 2012; Robertson et al. 2011; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Serner et al. 2021; Bharam et al. 2018; Ueblacker, English, and Mueller-Wohlfahrt 2016; Hopp et al. 2013; Weir et al. 2011), was 16.7 months (mean range, 4-72 months). One study did not report average patient follow up (Mei-Dan, Lopez, Carmont, et al. 2013). Each included study formally reported the cause of the injury as being related to sports (Table 1).
Thirteen studies focused on chronic adductor-related groin pain (Schilders et al. 2009; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Moreno et al. 2017; Dojčinović et al. 2012; Robertson et al. 2011; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013; Weir et al. 2011), and six studies examined acute injuries of the adductor tendon (Table 2). (Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Serner et al. 2021; Bharam et al. 2018; Ueblacker, English, and Mueller-Wohlfahrt 2016) Among these thirteen papers that examined chronic injuries, ten studies (Schilders et al. 2009; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Moreno et al. 2017; Robertson et al. 2011; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013; Weir et al. 2011) specifically explored the duration of symptoms prior to the initiation of treatment, which ranged from 4 to 20.4 weeks.
Diagnostics
In all studies assessing acute cases, the confirmation of diagnosis was consistently achieved through a combination of patient history, physical examination, and MRI (Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Serner et al. 2021; Bharam et al. 2018; Ueblacker, English, and Mueller-Wohlfahrt 2016). The authors examined avulsion injuries and reported the degree of tendon retraction using MRI, revealing a range from 0.8 cm to 5 cm (Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Serner et al. 2021; Bharam et al. 2018; Ueblacker, English, and Mueller-Wohlfahrt 2016).
The predominant imaging modality employed for diagnostics, as noted by 10 studies, was MRI of the pelvis, which most commonly included findings of enthesopathy of the adductor longus, bone marrow edema in the pubic bone and tendon avulsion from the superior pubic ramus (Schilders et al. 2009; Maffulli et al. 2012; Moreno et al. 2017; Dojčinović et al. 2012; Robertson et al. 2011; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Emblom, Mathis, and Aune 2018; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013). One study indicated that the diagnosis was established based on clinical indications of chronic adductor-origin pain (Gill, Wall, Gwathmey, et al. 2020).
Conservative treatment
Four studies evaluating acute injuries reported on conservative management (Table 2) (Best et al. 2020; Schlegel et al. 2009; Serner et al. 2021; Ueblacker, English, and Mueller-Wohlfahrt 2016). Best et al. implemented nonoperative treatment for patients with less than 2 cm retraction of the tendon stump, involving two to three weeks of non-weight bearing with crutches, gradually resuming activity if symptom-free (Best et al. 2020). Schlegel et al. reported non-operative treatment for 14 of 19 adductor longus injuries (79%), incorporating a phased progression of activities over 3 to 4 weeks, along with anti-inflammatory medication, ice and heat application, and mild electrical stimulation (Schlegel et al. 2009). Serner et al. conducted a 1-year follow-up on non-surgical treatment for adductor longus avulsions, involving an exercise-based rehabilitation program encompassing specific groin exercises aimed at maintaining a pain rating of 2 on a numerical scale ranging from 0 to 10 (Serner et al. 2021; Serner, Weir, Tol, et al. 2020). Injection therapies were not administered as part of the treatment protocol (Serner et al. 2021). Principio del formularioUeblacker et al. detailed conservative treatment for six athletes with adductor injuries, involving ultrasound evaluation, drainage of hematomas or seromas, and a rigorous rehabilitation protocol after complete avulsion (Ueblacker, English, and Mueller-Wohlfahrt 2016).
Four studies discussing chronic injuries reported conservative treatment options (Table 2) (Moreno et al. 2017; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Weir et al. 2011). Moreno et al. detailed an intratendinous percutaneous electrolysis technique in combination with an active physical therapy program (Moreno et al. 2017). A randomized clinical trial by Weir et al. compared exercise therapies (ET) to a multi-modal treatment (MMT) involving heat, manual therapy, and a gradual return to running (Weir et al. 2011). Topol et al. explored prolotherapy with a solution of 12.5% dextrose and 0.5% lidocaine applied to the ischiopubic ramus (Topol, Reeves, and Hassanein 2005). Masala et al. conducted a prospective nonrandomized single-group study where pulse-dose radiofrequency was performed on 32 patients with a chronic pain refractory to conservative therapies during the last 3 months (Masala, Fiori, Raguso, et al. 2017).
Surgical treatment indications and technique
Four studies reported patients who underwent surgical treatment for acute injuries (Table 2) (Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Bharam et al. 2018). Best et al. employed surgical treatment when adductor longus muscle retraction exceeded 2 cm (Best et al. 2020). Schlegel et al. utilized suture anchors for surgical repair in 5 out of 19 adductor longus muscle cases (26%). Across all four studies, the chosen surgical technique involved reattaching the adductor longus tendon using one to four suture anchors, varying based on the specific case (Best et al. 2020; Schlegel et al. 2009; Lempainen et al. 2021; Bharam et al. 2018). Lempainen et al. added a transverse release of the superficial fascial layer of the adductor longus to their procedure to mitigate postoperative adductor longus tightness (Schilders et al. 2013; Lempainen et al. 2021).
Nine studies reported surgical management of chronic injuries (Table 2). (Schilders et al. 2009; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Dojčinović et al. 2012; Robertson et al. 2011; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013) Six studies reported on complete adductor tenotomy through a 2 to 3 cm incision, with Maffulli et al. and Dojčinović et al. performing tenotomies on both sides, addressing both symptomatic and asymptomatic sides (Maffulli et al. 2012; Dojčinović et al. 2012). Four studies exclusively released the affected side (Gill, Wall, Gwathmey, et al. 2020; Robertson et al. 2011; Sansone, Ahldén, Jonasson, et al. 2014; Mei-Dan, Lopez, Carmont, et al. 2013). Schilders et al. and Emblom et al. performed a partial tenotomy on the affected side, focusing exclusively on the superficial fibers of the adductor longus (Schilders et al. 2009; Emblom, Mathis, and Aune 2018). Hopp et al. described an alternative surgical approach, involving arthroscopic pubic symphysis curettage and adductor reattachment using two suture anchors (Hopp et al. 2013).
Return-to-sport
Out of nineteen studies, 14 (73.6%) investigated return-to-sport (RTS) metrics (Table 2) (Schilders et al. 2013; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Dojčinović et al. 2012; Robertson et al. 2011; Emblom, Mathis, and Aune 2018; Schlegel et al. 2009; Lempainen et al. 2021; Serner et al. 2021; Bharam et al. 2018; Ueblacker, English, and Mueller-Wohlfahrt 2016; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013; Weir et al. 2011). The RTS for conservatively and surgically treated injuries were 12.5 and 13.4 weeks, respectively (Table 3). Six studies reported information about RTS following acute injuries. Schlegel et al.'s found a mean RTS of 6.1 weeks for the nonoperative group and 12.0 weeks for the operative group, with a RTS rate of 100% (Schlegel et al. 2009). Best et al. demonstrated 57.1% of patients treated conservatively returning to pre-injury sport level, while 85.7% achieved this outcome following surgical repair (Best et al. 2020). Bharam et al. noted a RTS rate of 100% and mean RTS time of 4.8 months following reattachment of the avulsed proximal adductor (Bharam et al. 2018). Lempainen et al. found 91% returned to preinjury activity level, with only 10% returning at a lower level (Lempainen et al. 2021).
Two studies (Serner et al. 2021; Ueblacker, English, and Mueller-Wohlfahrt 2016) reported a median RTS time of 9.9 and 12.7 weeks after strict rehabilitation protocol. This protocol continued until patients achieved a state of being pain-free, after which they advanced to a carefully monitored sports training phase (Serner et al. 2021; Ueblacker, English, and Mueller-Wohlfahrt 2016).
Eleven studies investigated RTS following treatment for chronic adductor tendinopathy. Eight studies provided information on RTS after surgical treatment (Schilders et al. 2009; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Dojčinović et al. 2012; Robertson et al. 2011; Emblom, Mathis, and Aune 2018; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013).
Maffulli et al. reported 69% returning to preinjury levels, 7% to higher levels, and 14% to lower levels, with a median return time of 18 weeks (range, 16-26 weeks) (Maffulli et al. 2012). Four studies found RTS time between 11.6 and 14.4 weeks after surgical repair of the adductor tendon (Gill, Wall, Gwathmey, et al. 2020; Dojčinović et al. 2012; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013). Gill et al (Gill, Wall, Gwathmey, et al. 2020). reported 96% returning to play and 94% at their previous level, and Schilders et al. who demonstrated 97.6% returning to the same level of sports after partial release, with an average of 9.21 weeks (Schilders et al. 2013). Moreover, Emblom et al. reported a RTS time of 4.1 months, with 96% returning to their pre-injury level (Emblom, Mathis, and Aune 2018). Robertson et al. used a 1 to 4 scale to gauge chronic groin pain and athletes’ ability to play, with 1 indicating pain-free play and 4 denoting an inability to play. Of the 38 patients at level 4 pre-surgery, 91% returned to level 1 within 15 weeks. Overall, 91% improved, with 74% returning to pre-injury performance (Robertson et al. 2011).
One study (Weir et al. 2011) performed by Weir et al. reported on the association between RTS and conservative treatment, where they recorded significant differences in RTS time between multi-modal treatment (MMT) and exercise therapies (ET) groups (p=0.043) (Weir et al. 2011).
Patient-Report Outcomes
Hip Outcome Score-Activities of Daily Living and Hip Outcome Score-Sport Specific (HOS-ADL and HOS-SS)
From the studies evaluating patients with acute tendinopathy, two studies reported Hip Outcome Score (HOS) values post-treatment. Bharam et al. compared preoperative and postoperative HOS scores, revealing significantly improved postoperative scores for all patients (HOS-ADL: 99.0 vs 43.2, HOS-SS: 98.9 vs 8.3; P < .001 for all) (Bharam et al. 2018).
Best et al. noted a higher HOS-SS in the non-operative group (33.9) compared to the surgical group (35.7), with no differences in HOS-ADL (both groups scored 68 out of 68) (Best et al. 2020).
Among the studies treating chronic injuries, Emblom et al. performed a partial tenotomy on the affected side and presented post-treatment HOS scores, showing a mean HOS-ADL of 99.1 ± 3.7 (range, 76-100) and a mean HOS-SS of 96.4 ± 9.7 (range, 42-100) (Emblom, Mathis, and Aune 2018). Also, the study observed higher HOS-ADL and HOS-SS scores in male athletes when compared to female athletes (Emblom, Mathis, and Aune 2018).
Tegner score
Three studies reported Tegner scores (Lempainen et al. 2021; Mei-Dan, Lopez, Carmont, et al. 2013; Weir et al. 2011). In the acute injury group, Lempainen et al. conducted adductor tendon repair and provided preinjury Tegner scores with a median of 9 (range, 5-10) (Lempainen et al. 2021).
In the chronic injury group, Mei Dan et al. compared Tegner scores before and after adductor tenotomy surgery, finding that the mean postoperative score remained the same as the preoperative score (8.2±1.9 vs 8.3±0.6). Only 2.8% (4/140) of patients experienced a reduction in their score, while 7.8% (11/140) achieved an increased Tegner score postoperatively, going up by at least one level compared to their baseline Tegner score (Mei-Dan, Lopez, Carmont, et al. 2013). Weir et al. reported only preinjury Tegner scores of 8.7 in both studied groups (Weir et al. 2011).
Modified Harris Hip Score (MHHS)
In studies focusing on acute adductor-related groin pain, two groups reported postoperative measurements of Modified Harris Hip Score (MHHS). Best et al. compared conservative and surgical groups and found no difference in MHHS, with both groups achieving excellent outcomes (100 out of 100) (Best et al. 2020). Furthermore, Bharam et al. compared MHHS before and after surgery, revealing significantly improved postoperative scores for all patients compared to their mean preoperative scores (97.1 vs. 44.6, respectively; p < .001) (Bharam et al. 2018).
Visual analog scale (VAS)
In the acute injury group, Bharam et al. used a 100-point Visual Analog Scale (VAS) to assess patients’ pain, with 0 indicating no pain and 100 indicating severe pain. They observed a significant improvement in mean postoperative VAS scores for all patients, decreasing from 89.2 to 2.2 (p < .001) (Bharam et al. 2018)
In the chronic injury group, seven studies provided VAS scores, with three comparing preoperative and postoperative scores after surgery (Schilders et al. 2009; Gill, Wall, Gwathmey, et al. 2020; Dojčinović et al. 2012; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Hopp et al. 2013; Weir et al. 2011). These studies showed a significant reduction in pain levels post-surgery, as reflected by decreased VAS scores (Schilders et al. 2009; Dojčinović et al. 2012; Hopp et al. 2013). Gill et al. reported only postoperative VAS scores, noting that 75% of patients were asymptomatic during follow-up (Gill, Wall, Gwathmey, et al. 2020).
Three studies on conservative treatment showed a significant improvement in pain, as evidenced by a decrease in VAS scores after treatment (p < .001) (Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Weir et al. 2011). Weir et al., however, did not find a significant difference in VAS scores between the multi-modal treatment (MMT) and exercise therapies (ET) groups (Weir et al. 2011).
Nirschl Pain Phase Scale (NPPS)
Two studies presented both pre and postoperative values of the NPPS score (Topol, Reeves, and Hassanein 2005; Hopp et al. 2013). Hopp et al. demonstrated that following arthroscopic pubic symphysis curettage and adductor reattachment, at the latest follow-up after surgery, all patients fell within the range of being either pain-free or experiencing only mild symptoms before or during activity, with an NPPS score of 3 (Hopp et al. 2013). Furthermore, Topol et al. reported that patients treated with prolotherapy experienced an improvement in their NPPS score, decreasing from 5.3±0.7 to 0.8±1.9 (p < .001) (Topol, Reeves, and Hassanein 2005).
Self-reported outcome score
Three studies documented self-reported outcome scores. Lempainen et al. detailed outcomes for patients with acute injuries who underwent surgical repair, with results rated as excellent in 57.5%, good in 32.5%, and moderate in 10%. Athletes achieving excellent outcomes underwent surgery sooner than those with good or moderate outcomes (2.4 ± 1.8 vs. 11.4 ± 11.0 weeks; p < 0.01) (Lempainen et al. 2021)
Mei Dan et al. employed a 5-point scale for subjective scoring, demonstrating a postoperative score of 4.4±0.9. They also introduced a combined score considering subjective evaluation, return to play, and Tegner score, with a mean score of 85.1±18.2 out of 100 (Mei-Dan, Lopez, Carmont, et al. 2013).
Conversely, Emblom et al. assessed overall hip and sports function, revealing male patients report significantly higher scores than females in both categories, after undergoing partial tenotomy. Male patients were significantly more likely to report normal hip function (p = .047) (Emblom, Mathis, and Aune 2018).
Hip Disability and Osteoarthritis Outcome Score (HOOS), Short Form Health Survey (SF-36), and European Quality of Life–5 Dimensions scale (EQ-5D)
Maffulli et al (Maffulli et al. 2012). compared HOOS, SF-36, and EQ-5D scores before and after surgery, revealing significant improvements across all scales (p < .0001). They observed a substantial increase in the percentage of patients able to engage in sports at their pre-injury level (from 0% to 75%; p < .0001), a significant decrease in those fully unable to participate in any sport activity (from 55% to 10%; p < .0001), and a reduction in patients limited to reduced sports activities (from 45% to 14%; p < .0001). In contrast, Sansone et al. utilized the EQ-5D score but did not observe a significant difference in the score (Sansone, Ahldén, Jonasson, et al. 2014).
Complications
The rate of complications for conservatively versus surgically treated injuries were 0% and 5.5%, respectively (Table 3). In the context of acute injuries, three studies (Schlegel et al. 2009; Lempainen et al. 2021; Bharam et al. 2018) provided information on complications following treatment (Table 2). Among these, two studies analyzed complications after surgical treatment, while one study focused on complications following a comparison between conservative and surgical treatments.
Schlegel et al. reported a reinjury at 4 weeks after one patient returned to sport following conservative treatment. In addition, one patient in the surgical repair group experienced complications, including a draining wound and heterotopic ossification, both of which were successfully resolved (Schlegel et al. 2009). Furthermore, Lempainen et al. identified postoperative complications in 3 patients (7.5%). Specifically, wound infections were observed in 3 cases, with 2 of them resolving successfully with oral antibiotics, while the third required treatment involving scar removal and partial adductor release (Lempainen et al. 2021). These findings are consistent with those reported by Bharam et al, who noted a single patient (16.6%) experiencing persistent wound drainage. In this case, wound re-exploration with scar removal was required at 6 weeks postoperatively (Bharam et al. 2018).
Three studies (Best et al. 2020; Serner et al. 2021; Ueblacker, English, and Mueller-Wohlfahrt 2016) reported that no complications occurred following the management of acute adductor-related groin pain.
Five studies reported complications following surgical management of chronic injuries (Maffulli et al. 2012; Robertson et al. 2011; Emblom, Mathis, and Aune 2018; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013). Maffulli et al. performed 58 tenotomies in 29 patients and documented 10 complications, all successfully managed conservatively, encompassing 5% wound infections, 3% unilateral weakness, 2% hematoma, 2% numbness, 2% skin puckering, 3% painful scar, and 3% painful intercourse (Maffulli et al. 2012). Hopp et al. evaluated 5 cases of osteitis pubis and adductor longus tendinopathy by resecting the degenerative tissue and reattaching the tendon with suture anchors, and noted a single intraoperative complication (20%) during the repositioning of an anchor, which resulted in damage to the corona mortis, requiring vessel ligation (Hopp et al. 2013). Robertson et al. reported ten patients (9%) with persistent or worsening pain following surgical intervention, and two patients (1.8%) developed hematomas which required evacuation (Robertson et al. 2011). Mei Dan et al. reported one hematoma in the adductor tenotomy group (Mei-Dan, Lopez, Carmont, et al. 2013). Emblom et al. presented an overall complication rate of 7% (6/85 patients), involving 2 retears, 2 superficial wound infections, 1 hematoma, and 1 reoperation for heterotopic ossification (Emblom, Mathis, and Aune 2018).
Five studies reported no complications. Three (Schilders et al. 2013; Gill, Wall, Gwathmey, et al. 2020; Dojčinović et al. 2012) found no complications after surgical treatment for patients with chronic adductor-related groin pain, while two (Topol, Reeves, and Hassanein 2005; Weir et al. 2011) found no complications after conservative treatment.
DISCUSSION
The main findings of this study were that both conservative and surgical management are effective in treating patients with adductor tendinopathy and are successful in allowing athletes to return to sports. Conservative care has been shown to improve clinical outcomes as does surgery, particularly in cases of acute partial tears, potentially expediting return to play. For chronic injuries, surgical intervention appears to reduce the risk of persistent pain and may facilitate the return to sports. Regarding patient reported outcome scores, there is evidence supporting both surgical and non-surgical management, with no clear superior method in either the acute or chronic setting of adductor tendinopathy. The prevailing focus in adductor tendinopathy management has been on return-to-sport rates, neglecting comprehensive assessments of outcomes, complications, and the impact of injury chronicity. This systematic review aimed to fill this gap by thoroughly examining both surgical and non-surgical strategies, delving into patient-reported outcomes, complication rates, and the nuanced influence of injury chronicity on treatment effectiveness. Nevertheless, significant limitations persist in the current literature.
The literature emphasizes the efficacy of conservative approaches in the acute phase, with rehabilitation protocols demonstrating median RTS times of 2.3-2.9 months (Serner et al. 2021; Ueblacker, English, and Mueller-Wohlfahrt 2016). The current study found similar trends, revealing positive outcomes with conservative measures in acute cases, consistent with Schlegel et al. (6.1 weeks nonoperative vs. 12.0 weeks operative) and Best et al. (57.1% return at pre-injury level with conservative, 85.7% with surgical repair) (Best et al. 2020; Schlegel et al. 2009). Surgical interventions, specifically repair procedures, showed high success rates, as noted by Bharam et al., reporting a 100% return with an average time of 4.8 months (Bharam et al. 2018). Lempainen et al. reported a 91% return to preinjury activity level, emphasizing the rarity of returning at a lower level (10%) (Lempainen et al. 2021). This demonstrates the effectiveness of surgical intervention in acute adductor tendinopathy, despite the potential for a longer recovery time compared to conservative management.
Studies evaluating chronic adductor tendinopathy revealed a significant disparity in RTS times between different conservative treatments. Notably, Weir et al. found that multimodal therapy yielded significantly faster RTS than exercise therapy (12.8 weeks vs. 17.3 weeks, p=0.043) (Weir et al. 2011). A recent systematic review by Bisciotti et al (Bisciotti, Chamari, Cena, et al. 2021). specifically examined conservative treatment options for chronic adductor-related groin pain, and demonstrated that compression clothing and manual therapy, coupled with strengthening exercises, exhibited the most compelling evidence for potential benefits (Bisciotti, Chamari, Cena, et al. 2021). However, the authors noted limitations such as small sample sizes and literature bias, which is consistent with the present study’s findings. Surgical interventions in chronic cases, such as bilateral adductor release, demonstrated promising results, with Maffulli et al. reporting a 69% return to preinjury levels following bilateral adductor release, and some patients returning at lower levels (14%) (Maffulli et al. 2012). Notably, Gill et al. and Schilders et al. demonstrated high RTS rates (96-97.6%) after surgical procedures, underscoring the efficacy of surgical interventions (Schilders et al. 2013; Gill, Wall, Gwathmey, et al. 2020).
Comparing acute and chronic cases, the literature generally supports shorter RTS times for conservatively treated acute injuries (Schlegel et al. 2009; Serner et al. 2021; Ueblacker, English, and Mueller-Wohlfahrt 2016). Surgical interventions, involving repair or release, demonstrated high success rates in achieving pre-injury performance levels, despite potential extended recovery (Schilders et al. 2013; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Lempainen et al. 2021; Bharam et al. 2018). Careful consideration of individual patient characteristics and preferences is crucial in choosing between conservative and surgical approaches, emphasizing the need for higher quality studies directly comparing acute and chronic adductor tendinopathy management.
Previous studies by King et al. and Paajanen et al. have emphasized the necessity for higher quality research on athletic groin pain, focusing on laparoscopic repair techniques and outcomes (King et al. 2015; Paajanen et al. 2015). King et al.'s meta-analysis reported quicker return-to-play times with conservative management than surgical management for pubic-related groin pain (10.5 weeks vs. 23.1 weeks) and comparable return-to-play rates between surgical and rehabilitative intervention groups (King et al. 2015). Paajanen et al.'s findings align with the findings of the present review, showing that surgical interventions demonstrate high success rates from 70-90% (Paajanen et al. 2015).
The current study employed analysis of various patient-reported metrics, including visual analog scales, Hip Outcome Scores, and Tegner activity ratings. In acute injuries, there is limited data indicating no discernible differences in PROs between surgical and non-surgical management. However, the inconsistency and variability in reporting pose challenges to drawing firm conclusions. In chronic injuries, postoperative PRO improvements, including pain scores, hip scores, and activity levels, were observed after surgical management, with conservative treatment also leading to improvements (Schilders et al. 2009; Dojčinović et al. 2012; Topol, Reeves, and Hassanein 2005; Masala, Fiori, Raguso, et al. 2017; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013; Weir et al. 2011). It is noteworthy that Emblom et al. identified significantly greater improvements in PROs after surgery among male athletes compared to their female counterparts (Emblom, Mathis, and Aune 2018). Further research investigating this relationship may help determine the underlying reasons for these findings. Overall, surgery may offer reduced risk of persistent pain and improved function based on PROs, particularly for chronic adductor tendinopathy (Schilders et al. 2009; Dojčinović et al. 2012; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Lempainen et al. 2021; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013). Standardization of PRO reporting using validated tools at various postoperative time points will enhance the robustness of the evidence.
Complications in management of adductor tendinopathy were primarily associated with surgical management, with only one complication, re-injury, being reported for conservative treatment (Schlegel et al. 2009). Postoperative complication rates ranged from 0-10%, which were comprised of mostly minor issues such as wound drainage, heterotopic ossification, and infections (Schilders et al. 2009; Gill, Wall, Gwathmey, et al. 2020; Maffulli et al. 2012; Dojčinović et al. 2012; Robertson et al. 2011; Topol, Reeves, and Hassanein 2005; Emblom, Mathis, and Aune 2018; Sansone, Ahldén, Jonasson, et al. 2014; Mei-Dan, Lopez, Carmont, et al. 2013; Hopp et al. 2013; Weir et al. 2011). However, the lack of consistent assessment and reporting using a validated system hinders effective safety profile comparisons between treatments. Future studies should compare various surgical techniques and explicitly report complications related to these methods to inform clinical decisions.
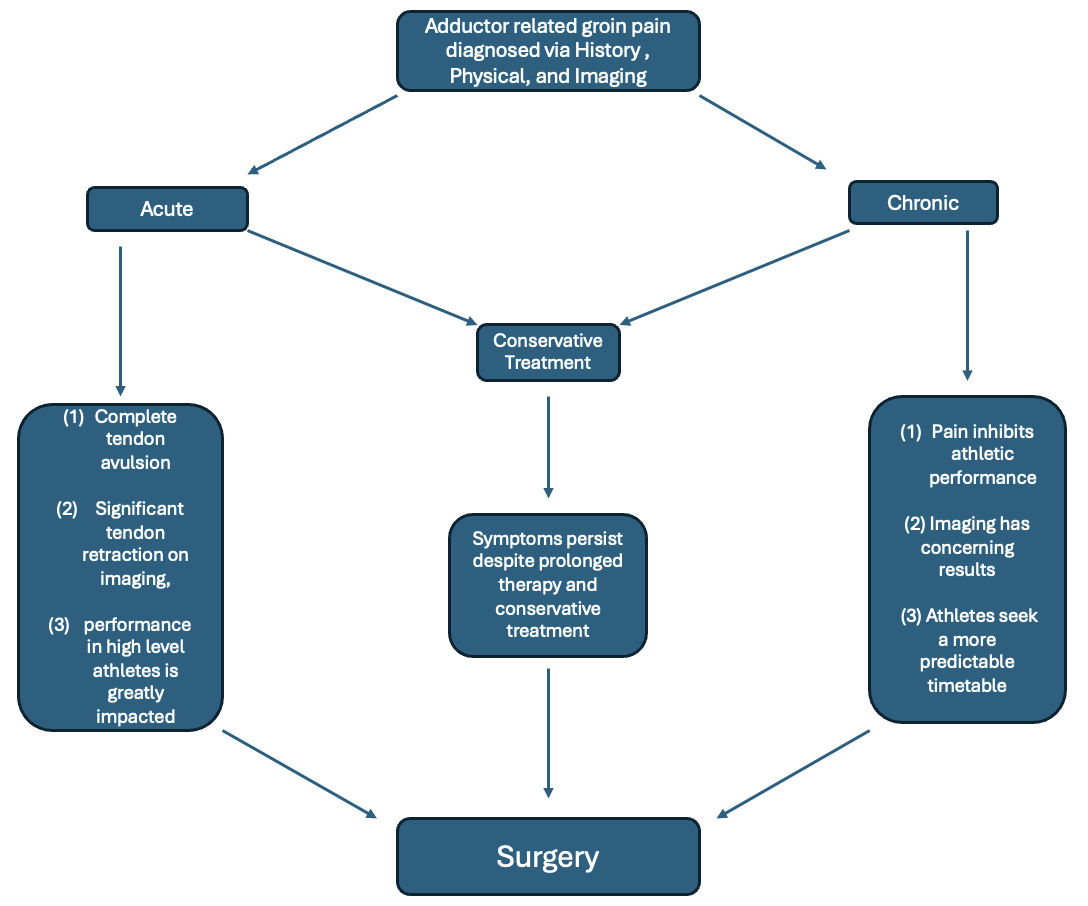
Based on the current study, acute injuries may be treated conservatively as there are similar RTS and outcomes, however, exceptions to this apply in situations such as complete tendon avulsion, there is significant tendon retraction on imaging, or performance in high level athletes is greatly impacted due to injury. Chronic adductor injuries appear to respond to conservative treat efficaciously as well; however, surgical treatment is indicated if symptoms continue to persist despite prolonged therapy and conservative treatment, pain inhibits top tier athletic performance, imaging has concerning results such as tendon degeneration, or athletes seek a more predictable timetable about when they may return to play (Figure 4). Despite these frameworks, it is important to place each patient’s unique set of circumstances and goals at the forefront of treatment. Professional athletes lean more towards an expected recovery time period and attempt to minimize poor performance, while the amateur may more readily accept a trial period of conservative treatment.

Limitations of this review include a predominance of Level IV evidence that may lead to a higher risk of bias due to limited follow-up, small sample sizes, protocol heterogeneity, variability in outcome reporting, and a limited number of studies analyzing the impact of injury chronicity on treatment outcomes. In particular, low MINORS scores may place this study at risk of bias due to poor methodological quality. Additionally, sex-based differences in outcomes could not be meaningfully compared due to the majority of patients (95%) being male and numerous studies only included male cohorts making generalizability difficult to attain. Despite these challenges, this review stands as a comprehensive synthesis of the available literature on the management of adductor tendinopathy.
Higher quality randomized controlled trials directly comparing surgical and non-surgical approaches are essential to refine treatment approaches and optimize outcomes for athletes with adductor-related groin injuries. Studies including more females to further understand gender differences of conservative vs. surgical management of adductor tendinopathy is warranted given the limited number available. These studies should aim to identify clinical and imaging factors guiding management decisions. Implementing consistent rehabilitation protocols and longitudinal patient-reported outcome assessments using validated tools is crucial. Additionally, exploring alternative therapies, such as biologics for adductor tendinopathy, holds potential benefits. However, significant limitations in the existing literature underscore the need for high-quality comparative trials to establish tailored treatment approaches definitively.
CONCLUSION
Both conservative and surgical treatments lead to improve clinical and functional outcomes for both acute and chronic tears, facilitating patients to return to sports at their pre-injury level. Conservative care demonstrates comparable outcomes to surgery in acute partial tears, potentially expediting the return to play. In chronic injuries, surgical intervention may decrease the risk of persistent pain and result in slightly higher return-to-play rates.