


When presented with an ankle fracture, one of the most important things you can communicate to your patient is what happens after you fix the fracture: when you allow them to start walking, when they can weightbear, and when they should start range of motion. I would argue rehabilitation is a more important predictor of patient outcomes, versus which plate or screw system you used fix the injury.
We don’t necessarily operate on all ankle fractures. The following x-ray demonstrates a stable ankle fracture (Figure 1).

This patient can start immediate, protected, weight bearing in a boot or air cast. If you’re not practicing that, you should! I still see elderly patients with a small “crack” like this, that are kept non-weight bearing for two months. Don’t do that! These are stable injuries. They can start immediate, protected, weight bearing in a boot, and can wean out of the boot as tolerated.
The more interesting question is, “what about unstable ankle fractures, and what do you do after surgical fixation, in terms of when do you allow them to start weight bearing and start ankle range of motion?”

There’s much controversy in terms of should we wait or should we allow acute weight bearing following fixation of an unstable ankle fracture. Traditionally, patients were kept non-weightbearing for 6-12 weeks in some kind of cast or a boot. Nowadays, more contemporary approach is to allow earlier mobilization and protected weight bearing. Additionally, there’s many differences between North American and European schools of thought. When I give this talk to Europeans, they say “yeah we start immediate weight bearing all the time, that’s the standard.” But it’s certainly not the view in North America. I still see patients that have a beautiful x-ray with everything fixed and they’re kept in a cast for two months, which potentially defeats the whole point of surgical fixation. The benefit of surgery is to allow early mobilization and protected weight bearing. This practice can accelerate your patient’s return to work and return to life. However, nobody wants to see this x-ray in their clinic, especially with the staples still in (Figure 3).
This example is the fear that drives behavior amongst most orthopaedic surgeons who do not allow patients to move early.
So, what does the evidence say? There’s many studies looking at early versus delayed weight-bearing ankle fractures, many of which are RCTs. There are also several systematic reviews which demonstrate better outcomes with early weight bearing.
I was involved in a randomized controlled study when I was a young resident (Dehghan N, et al. J Orthop Trauma. 2016;30(7)). We randomized 110 patients, half started early weight bearing at two weeks, and the other half started weight bearing at six-weeks. These were all unstable ankle fractures, bi-malleolar equivalent, and tri-malleolar fractures with a small posterior malleolus where only the medial and lateral malleoli were fixed. Our study showed that at six-weeks patients in the Early weightbearing group had better range of motion, which makes sense because they were allowed to start moving earlier. However, there was no difference in the long-term. When you look at Olerud-Molander Ankle Scores, again, at six weeks there was clinically and statistically improvement with the early weight bearing group. When you look at the SF-36 health outcome scores, the early weight bearing group had better scores early on. And even in the long term they had better scores, but the difference was a lot less. And when you look at the mental component scores, again, early weight bearing did better. Patients liked it; they’re happier when they can get back to life sooner, which makes sense. And even in the long term there was some improvement with the early weight-bearing group.
Regarding complications, there were no fixation failures, and no malunions or non-unions in either group. Infection was the same between groups. Surprisingly, the delayed weight-bearing group had a higher proportion of patients with symptomatic hardware who underwent hardware removal. The study was conducted in Canada, where it’s difficult to get access to the OR, and hardware removal is not routine practice. We don’t just operate on everyone for symptomatic hardware removal, and these were patients that kept coming back complaining of hardware irritation. In speaking with other surgeons, I think the thought is that when you allow early range of motion, there is less scaring of the peroneal tendons and soft tissues to the implants and there’s easier glide. Potentially, that’s why there’s less irritation if you allow immediate range of motion.
So, what was the conclusions of our study?
-
There was no difference in terms of complications or fixation failure.
-
The early weight-bearing group had better early ankle scores, motion, and function.
We also later published a systematic review compiling 10 randomized control trials that have been published so far with the endpoint of overall outcomes (Dehghan N, et al. Int J Adv Research Ortho. 2024;6(1)). And again, even in a systematic review there’s better outcomes early on acutely and delayed when you look at early weight bearing compared to delayed weight bearing. This is for the OMA, the ankle Molander scores. Days off work is less with early weight bearing, which makes sense. People can get to work sooner. No difference in terms of nonunion and malunion and reoperations again trended towards less with early weight bearing.
Now, what about ankle fractures with syndesmosis injuries?
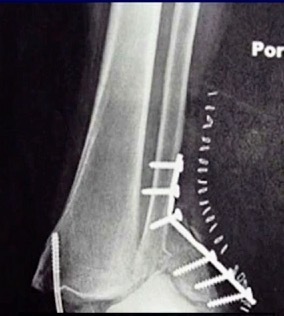
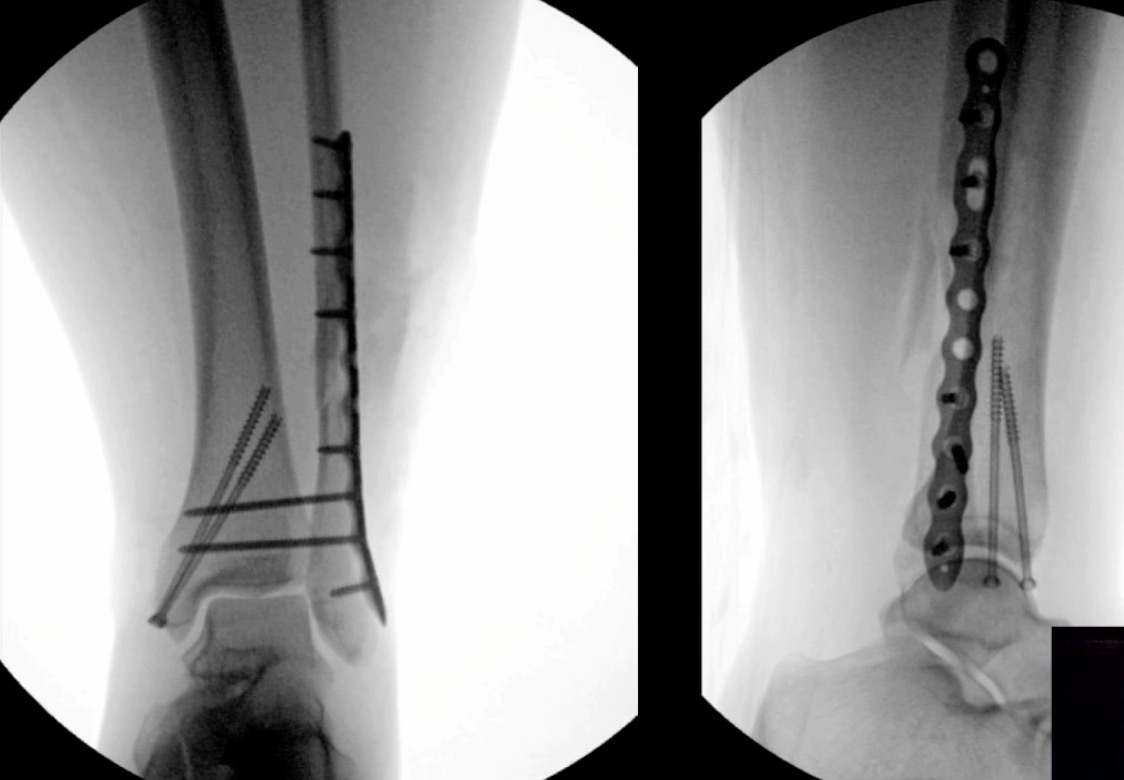
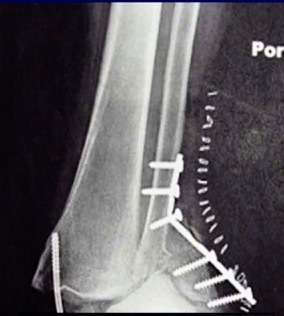
Our Randomized Controlled Trial specifically excluded those, because when I was a resident, syndesmosis injury was kept non-weight-bearing for three months, that was the standard (three months in a cast). Unfortunately, the treatment is sometimes worse than the disease. There is much controversy in terms of weight bearing for syndesmosis injuries, and not as much evidence on this specific injury compared to previously discussed ankle fractures. Figure 7 is a type of fracture we’re referring to: After you fix it, what do you do next?

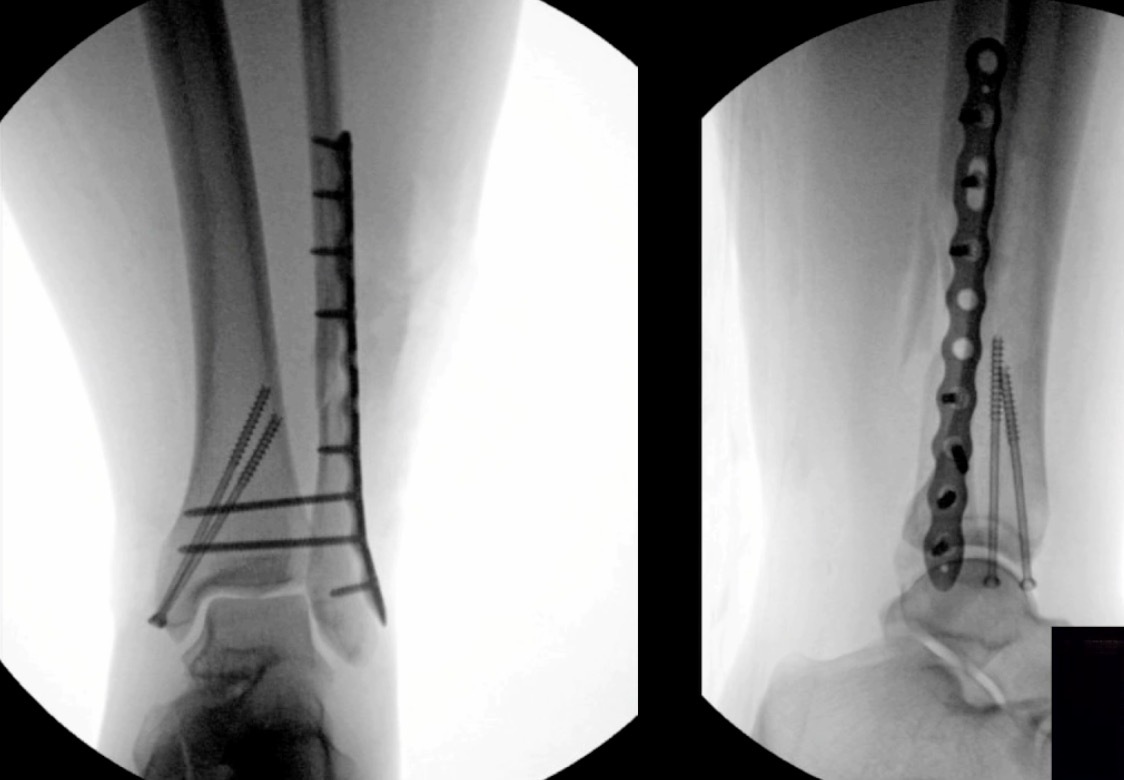
A small RCT (Khaleel M, et al. Foot Ankle Orthop. 2024;9(4)) was conducted assessing syndesmosis injuries comparing early versus delayed weight-bearing. They had a relatively small sample size: only 16 patients in one group, 23 in the other group, but they did show that there was potential improvement in range of motion with the early group, and there was no catastrophic failure. This raises an interesting question: “can we allow early weightbearing after syndesmosis fixation?”, and we need more studies on this specific topic.
Lastly, hot off the press, just published in JBJS last month, (Khojaly R, et al. J Bone Joint Surg. 2025;107-A) was a randomized controlled trial looking at immediate weight bearing. Fix the fracture, close the skin, give them a boot, they’re allowed to immediately weight bear. And this included all ankle fractures: bi- malleolar, tri- malleolar, syndesmosis, everything.
This study included160 patients, randomized to immediate weight bearing versus delayed weightbearing at six weeks. The results demonstrated that the immediate weight bearing group had much better scores in every outcome that you could think of. Range of motion was better, they got back to work sooner, their functional outcomes were better, and there was no difference in terms of complications. I believe this is the holy grail and what we need to focus on to improve patient outcomes. There’s no point spending all this time in the OR fixing things, and then keeping them in a cast or delay weightbearing for 6 weeks, especially in geriatric patients. An 80-year-old geriatric patient who is not allowed to weightbear as tolerated is basically going to be in a wheelchair for a prolonged length of time. We know from hip fracture studies that elderly patients don’t do well when they are kept immobile. They need to mobilize, which is potentially a life-saving measure. This may sound dramatic, but mobilization is really critical for these elderly patients. The body doesn’t know whether the ankle that’s broken or the femur or the hip. If you keep them non-weight-bearing in a wheelchair, it’s bad. Thus, I encourage all of you to allow immediate weight-bearing or early weight-bearing, especially for your geriatric fractures.
Now one caveat is that we are not talking about diabetic patients with neuropathy. In this select group of patients who lack protected sensation, it’s generally recommended to keep them off for a longer amount of time to protect the fixation. But in general, early weight bearing is safe and has better outcomes for all other patients.
In summary, immediate weightbearing after a stable ankle injury is safe and should be the standard practice. Regarding unstable ankle fractures that need surgery, early weight-bearing after ankle fracture fixation is safe, and recent studies suggest that even immediate weight-bearing is safe. In addition, patients have better functional outcomes as well. In geriatric patients, it’s even more critical to allow early mobilizing.