






Osteochondritis Dissecans (OCD) may be a satellite growth plate that’s never closed, or it might be vascular dyscrasia. However, its biology is equivalent to a fracture non-union. That’s important because all the decision-making is related to that. Patients generally become symptomatic when the piece is loose, but they may remain or become symptomatic later because of the defect bed itself failing to heal. But what’s interesting is that a lot like a wide tire that drives over a pothole, you never know you drove over it. That’s how OCD behaves. Amazingly, they don’t go on to have long-term problems in any predictable way, which is surprising. The spectrum involves juvenile versus adult onset. Juvenile does well, generally speaking, not always with non-surgical management. When juvenile presents as an adult, that’s when they typically have problems.
As a medical student or a resident, you’re taking boards: What’s the most common location of OCD? The lateral aspect of the medial femoral condyle. Second, the lateral femoral condyle. Lesions in the trochlea are third, followed by the patella. Then, every once in a while, you’ll see one involving the tibial plateau. And I’ve seen all of these. The average age is around 12 to 20 years old. Males get it more frequently. But we do see OCD in other places, like the ankle; females more commonly present than males. They tend to sprain their ankles more. Maybe there’s association. Males more than females in the capitellum, and that’s because we tend to see it in our throwers, followed by our gymnasts. There are theories that associate repetitive microtrauma, genetics , obesity, and ischemia with a predisposition to OCD lesions. Early on, patients will say very non-specific, vague complaints. Then they get progressive symptoms, and then they falter on with joint-specific symptoms like mechanical loading and things like that that cause pain.
This is the overall treatment paradigm. The approach early on, when they’re juvenile, is a hiatus from activities that generate symptoms much like a stress fracture. What we don’t do and what we shouldn’t do is put them in a cast or a brace or tell them to “hang it up.” Treat it like a stress fracture. Reduce the activities to the point where they don’t have pain. These can heal in the juveniles. In the adults, they may not always heal. They probably won’t heal once they become symptomatic because they have unstable fragments. So, the surgical decision-making order is as follows. If they get a loose fragment, then they have pain, we debride it, elevate it, debride it, drill it, and put it back with screws. That’s what most commonly might or could happen.
Sometimes it gets removed, either after it’s fixed and becomes loose later, or later on in the patient’s natural history. Or, you can’t do it at all at the time zero. If that happens, we debride it, microfracture, do an OATS. If they need a salvage situation, they get a cell transplant or an osteochondral allograft.
The only other thing to know is about stability. This is probably the most important physiology tenet. This is a biologic problem, because it’s a fracture non-union. But it’s a biomechanical problem because they’ve got a pebble in their shoe when they become symptomatic. So, we talk about the MRIs showing stability. The reality is if they hurt, they probably have microscopic instability. The challenge is if you take a microscopic versus a macroscopically unstable one, the treatment will differ.
What about the natural history? So, my favorite saying by a great philosopher, Voltaire, is, “The art of medicine consists of amusing the patient while nature cures the disease.” This is totally relevant to OCD. I get second and third opinions on a weekly basis from families with young children who are incredibly anxious because their kid had anterior knee pain. They got an X-ray or an MRI, and they said they had OCD, and they’ve got to stop their sports, and they have no symptoms whatsoever. So, this is one where a lot of skillful neglect can occur.
The risk of developing arthritis downstream is very low. If they do develop arthritis, it’s hardly ever clinically relevant. The risk of arthroplasty is very low. The prognostic variables that have independent associations with outcomes in the literature include size, BMI, and the fragment characteristics (is it stable?) Does it get removed, or does it get preserved? And finally, patient age.
Who’s going to heal in the young group? It’s going to be someone who’s much younger. Non-weight-bearing location. Lateral aspect of the medial femoral condyle can often be non-weight-bearing. Smaller lesions, no MRI signs of gross macro-instability, and the absence of sclerosis in cysts. These might heal.
But if they need surgery, this is a hierarchy. We try to fix it. If we can’t fix it, we remove it. If we remove it and they become symptomatic or they have a high risk, we think we can restore it. The worst thing you can do is go in there and leave a piece there that’s unstable because you’re too afraid to take it out, because you might cause further damage, or because you’re not going to help the patient. You’ve got to do something.
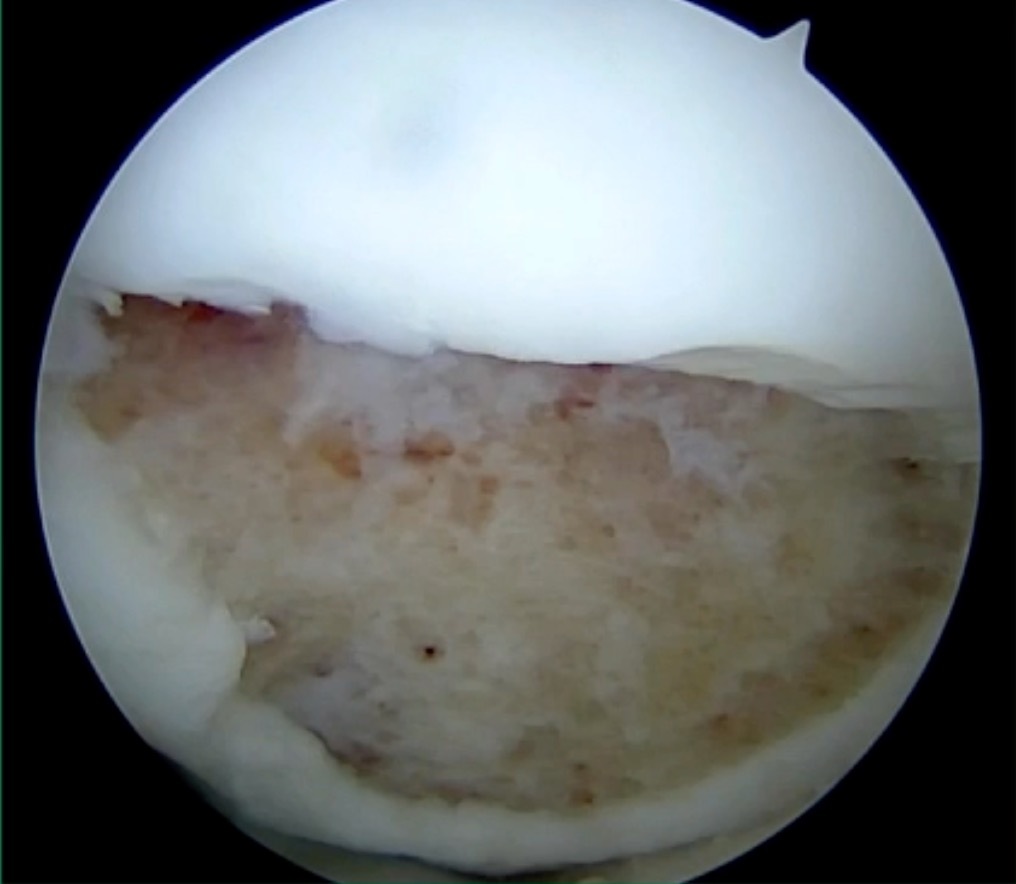
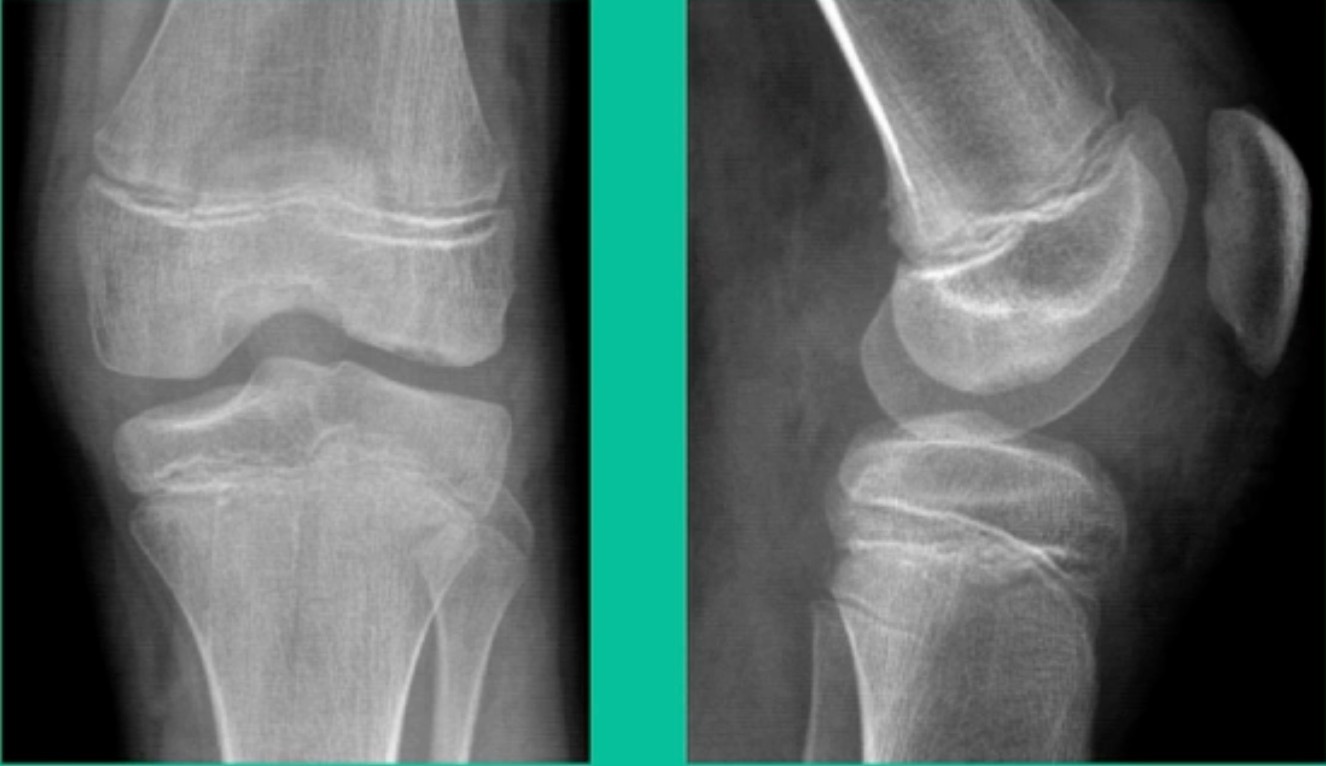
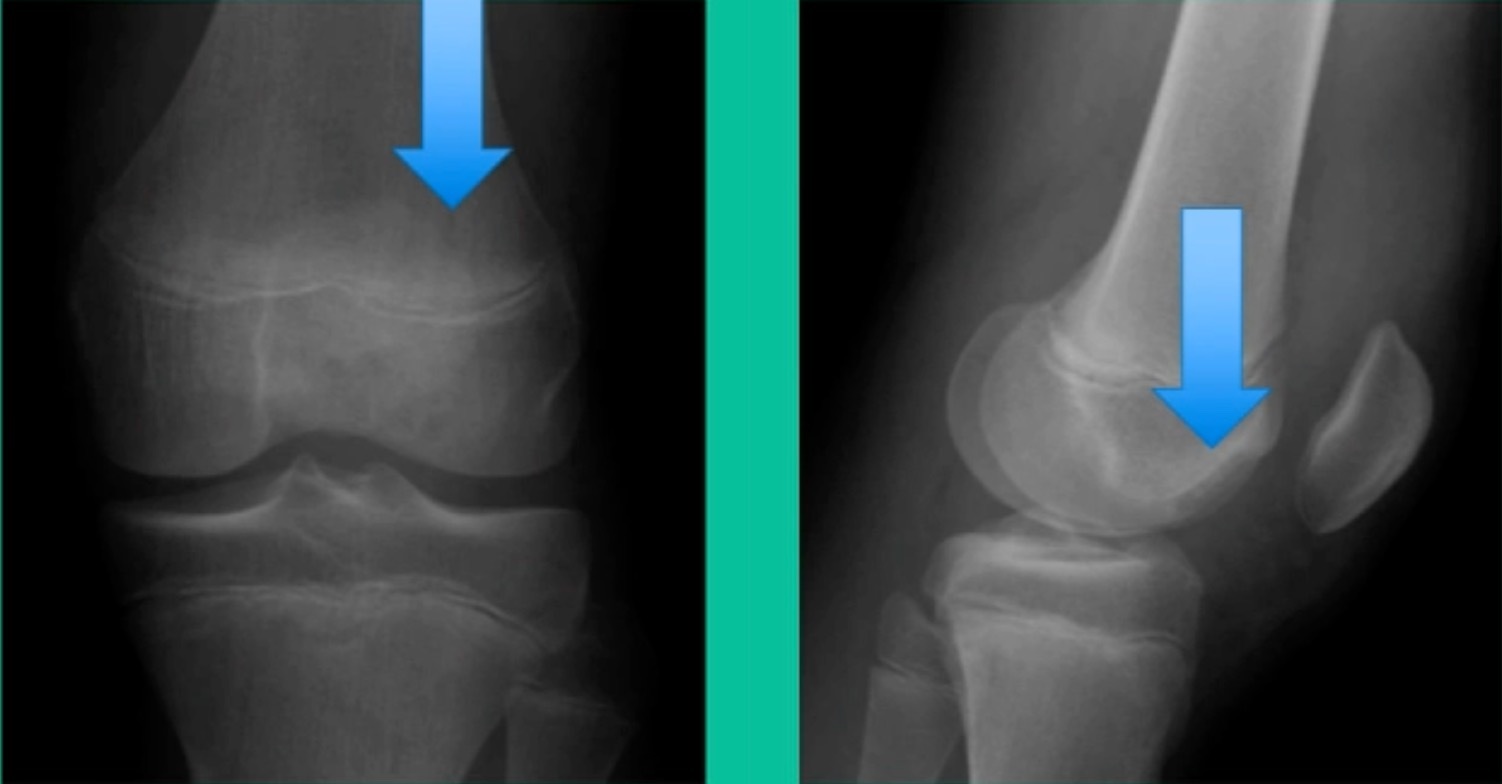
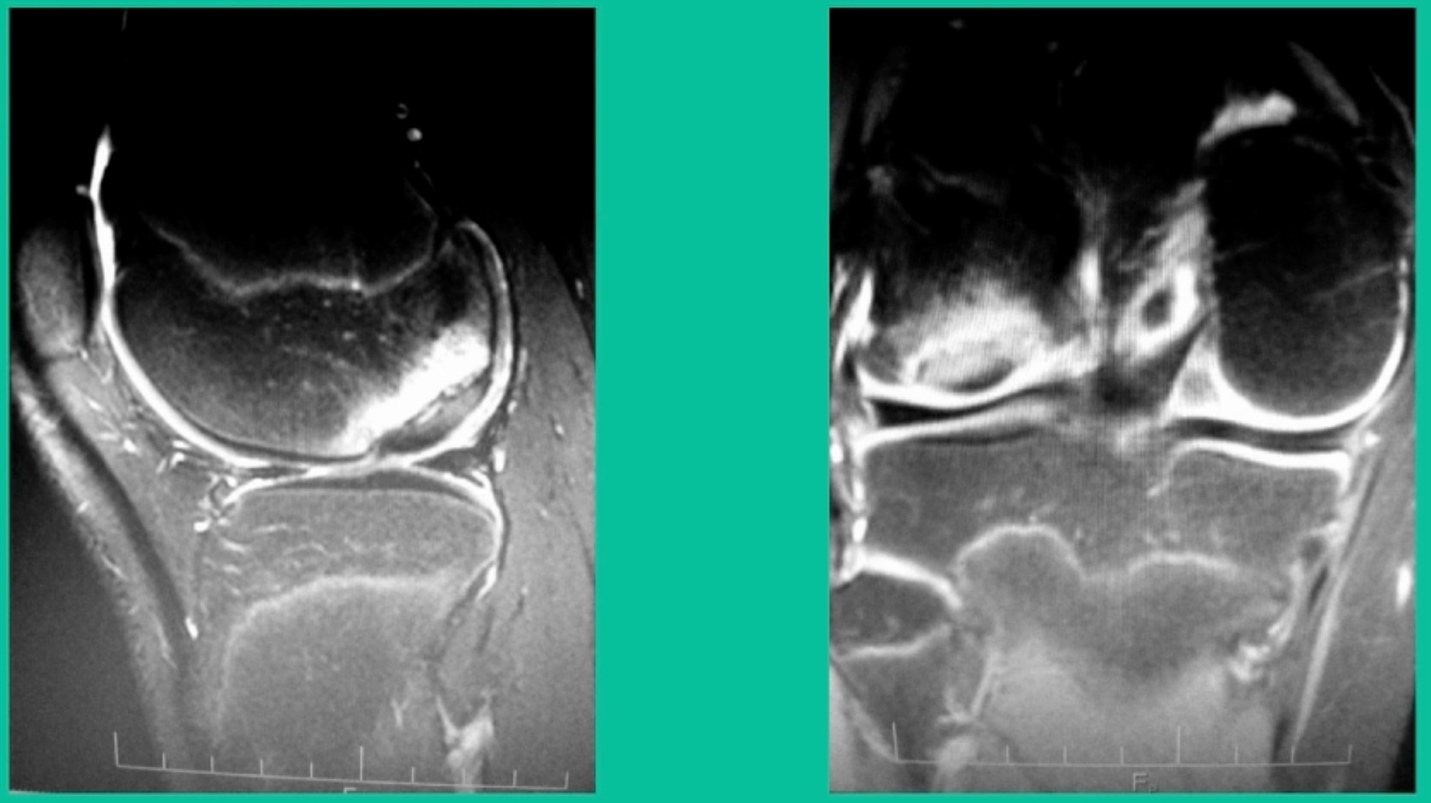
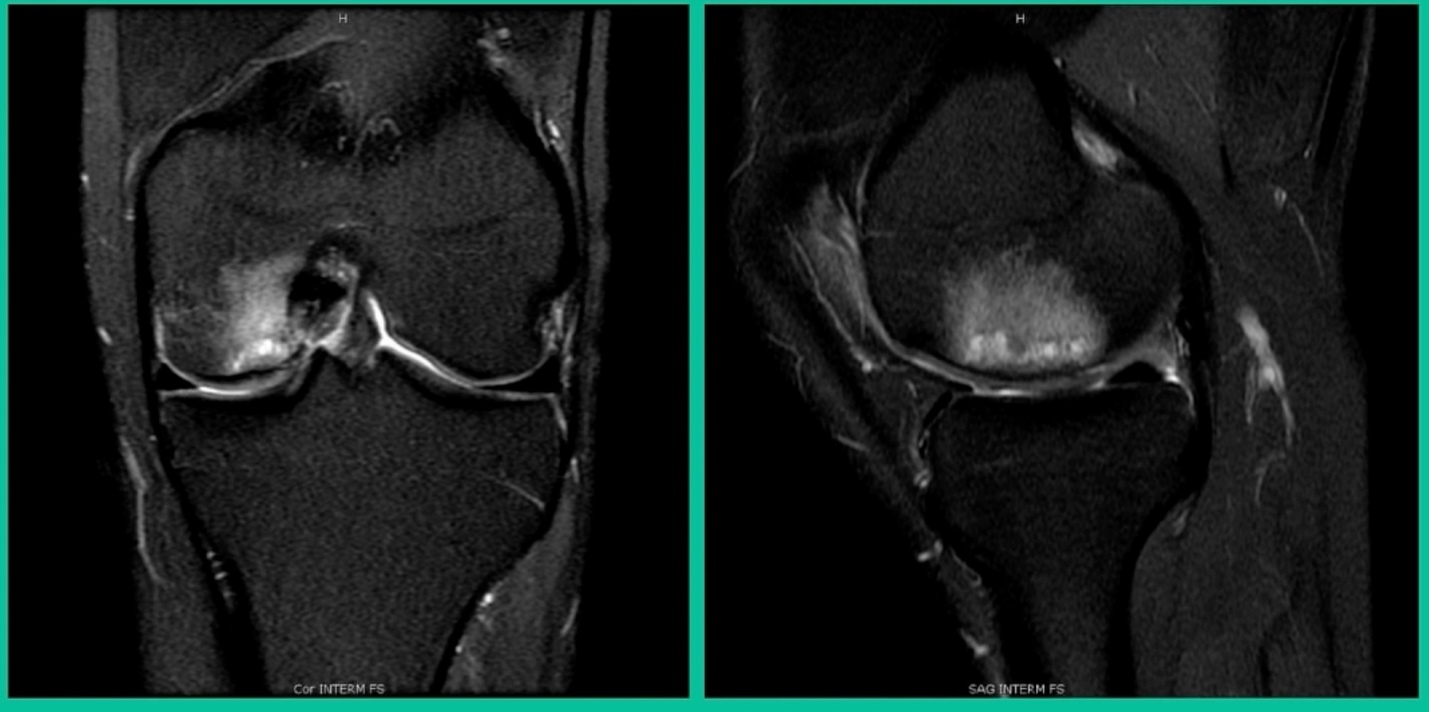
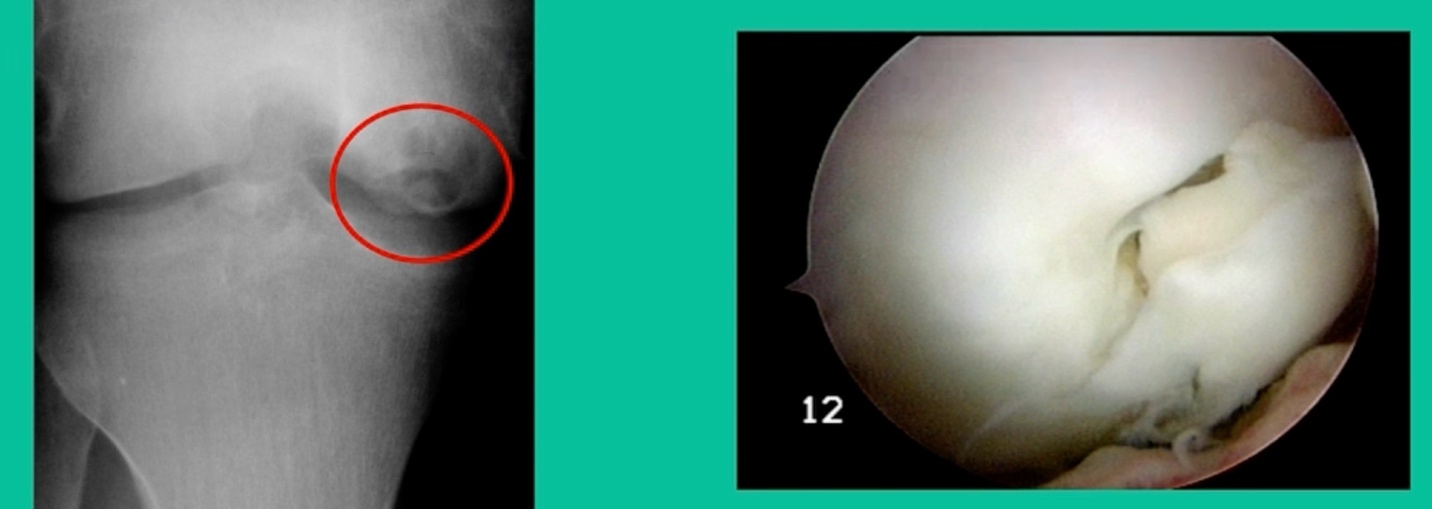
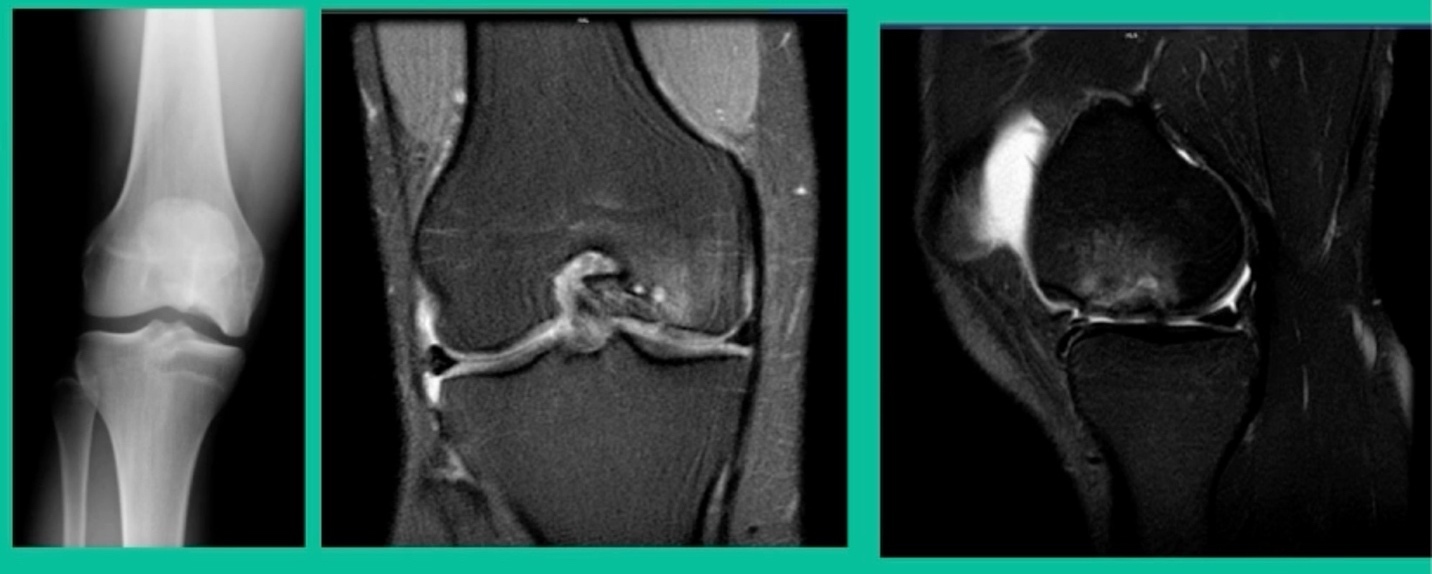
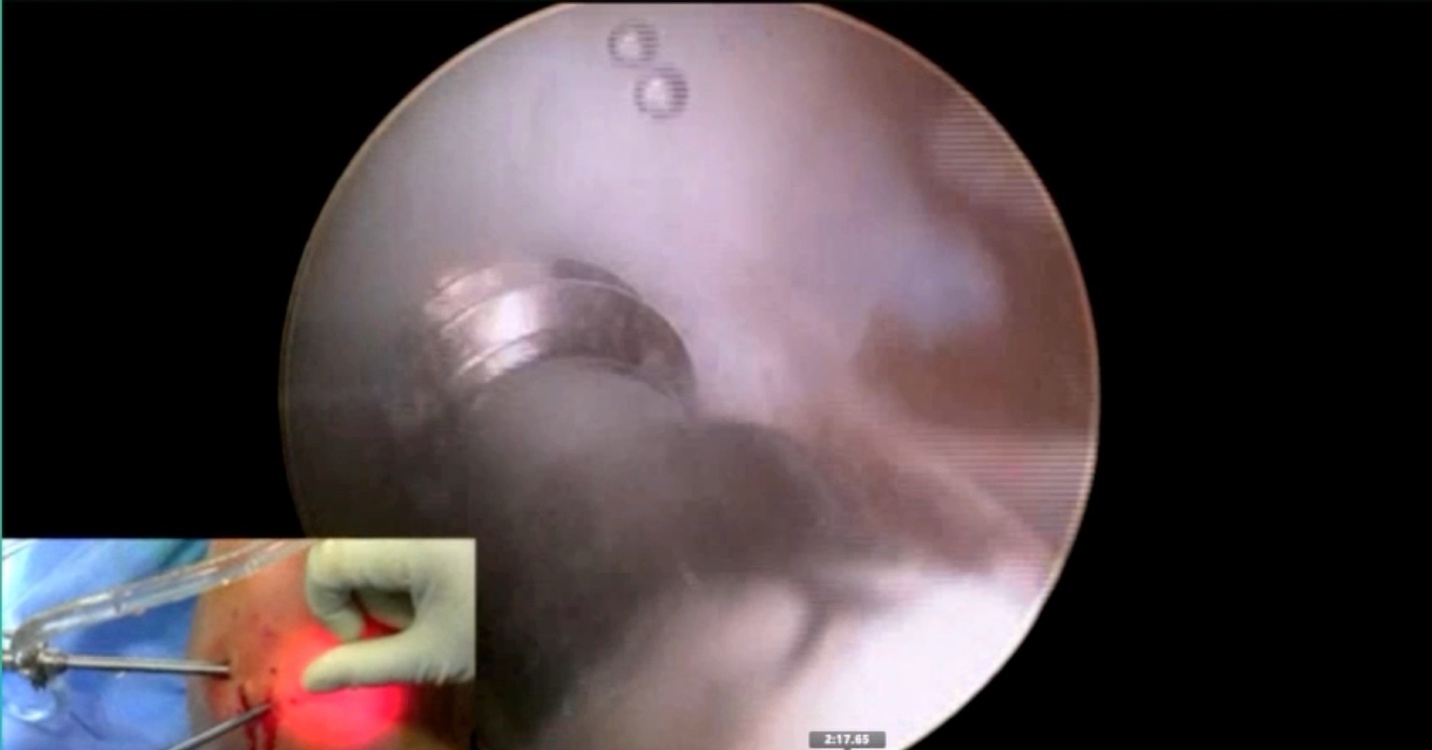
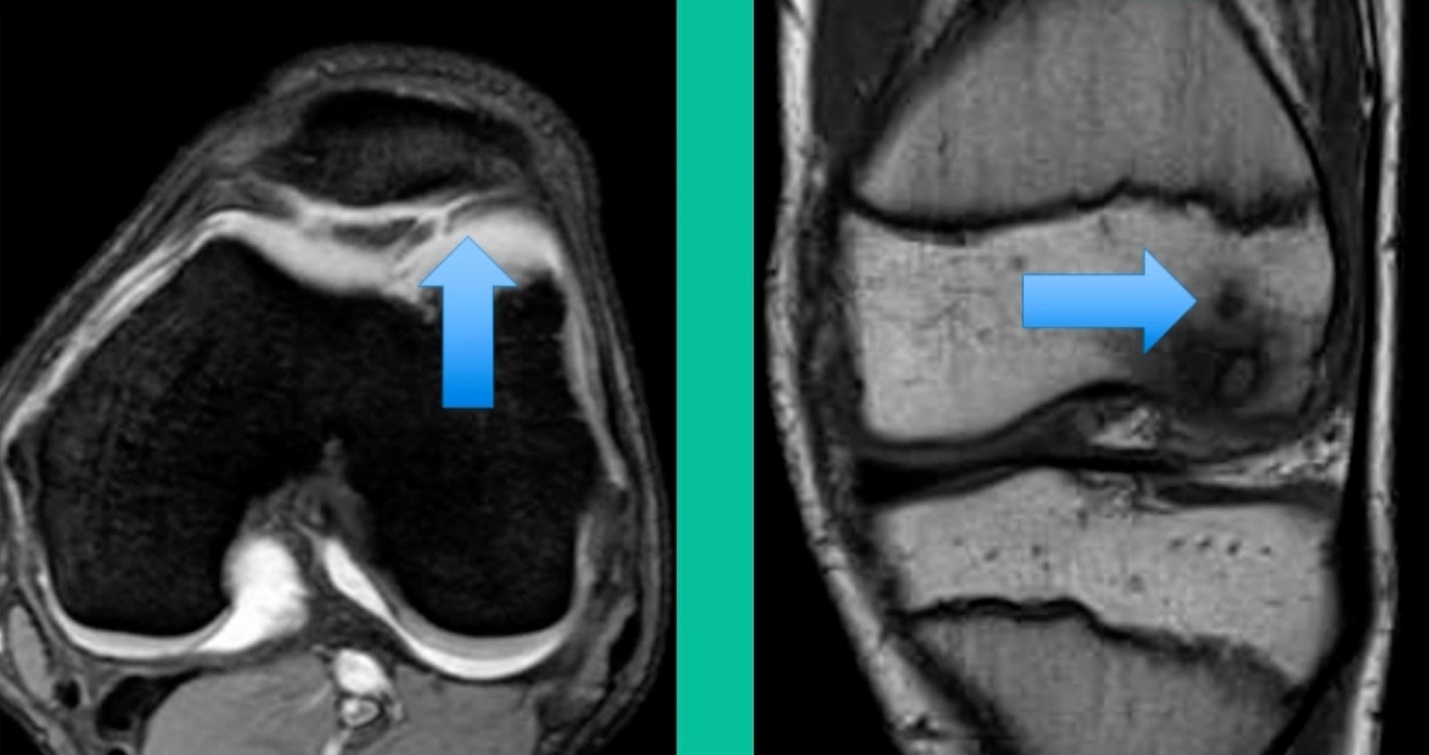
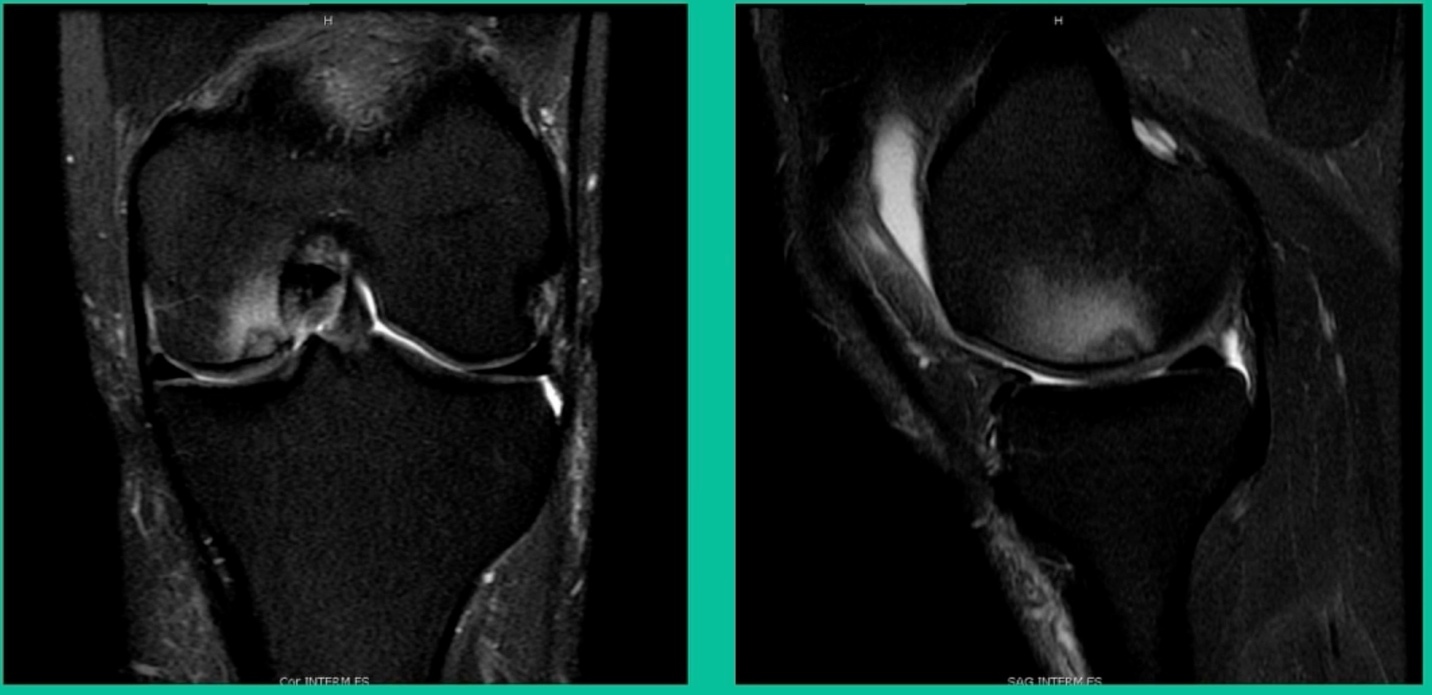
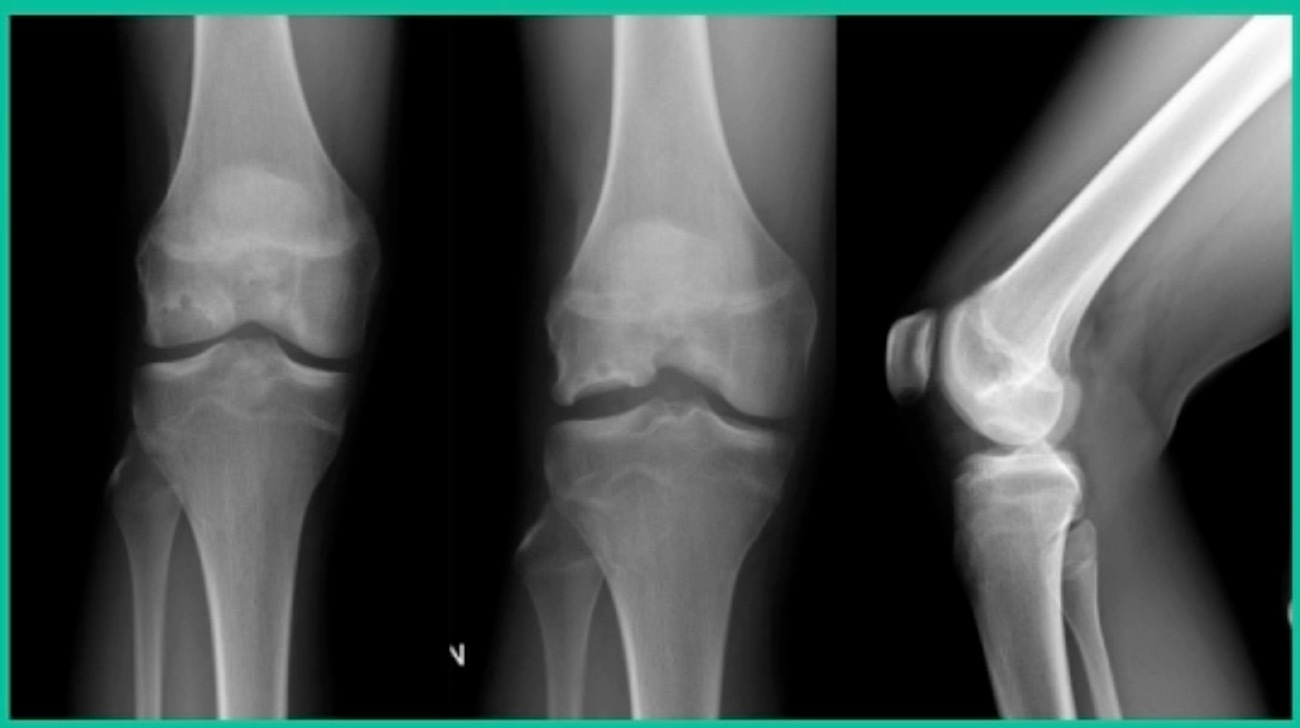
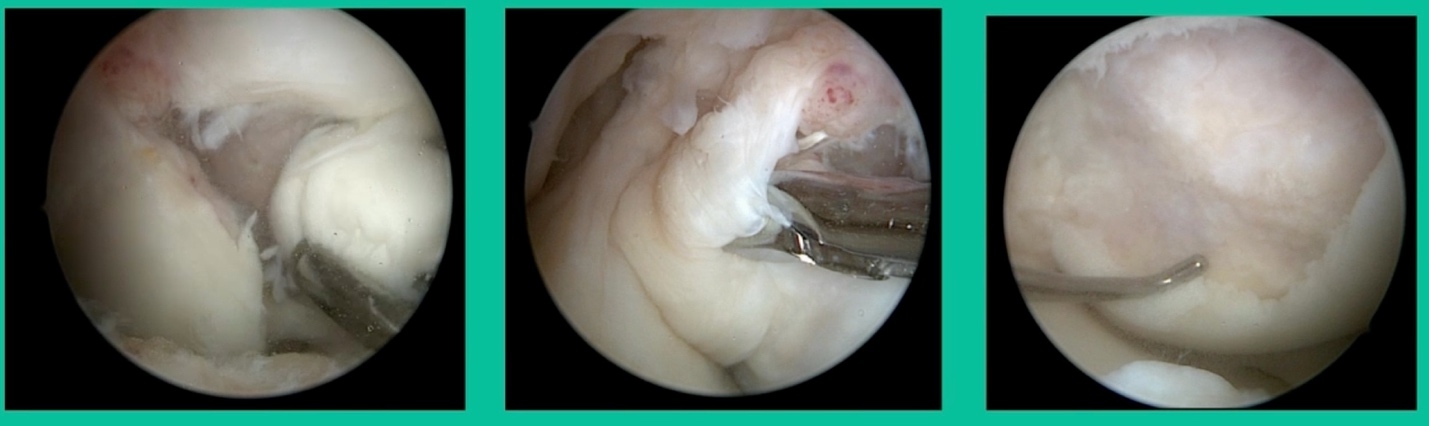
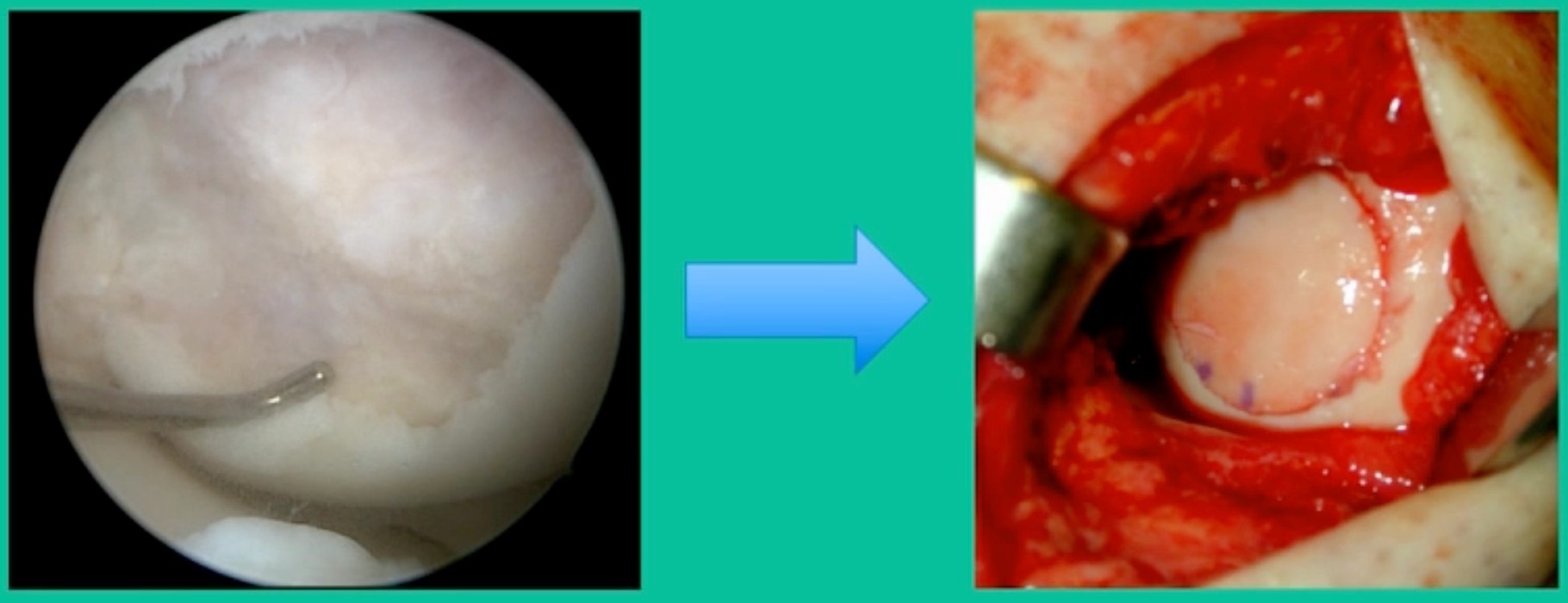
Now a couple of quick cases. This is juvenile OCD. This is the first series of three or four, just juveniles. 14-year-old, intermittent knee pain, lateral femoral condyle OCD (Figure 1).

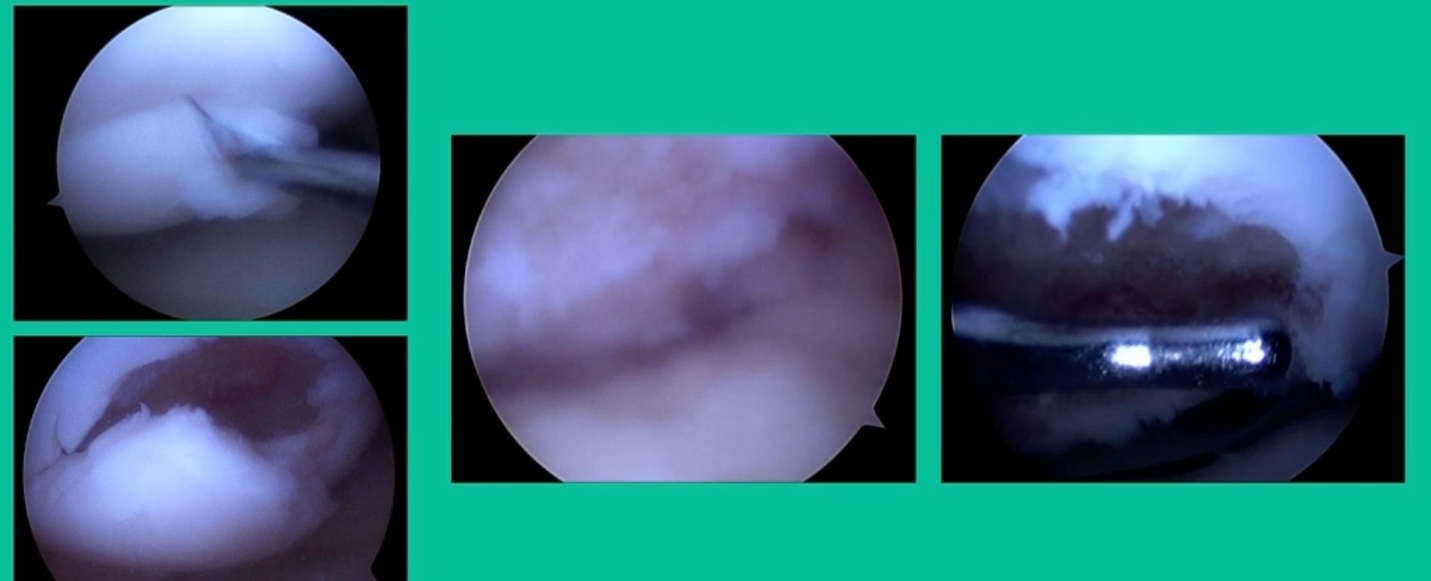
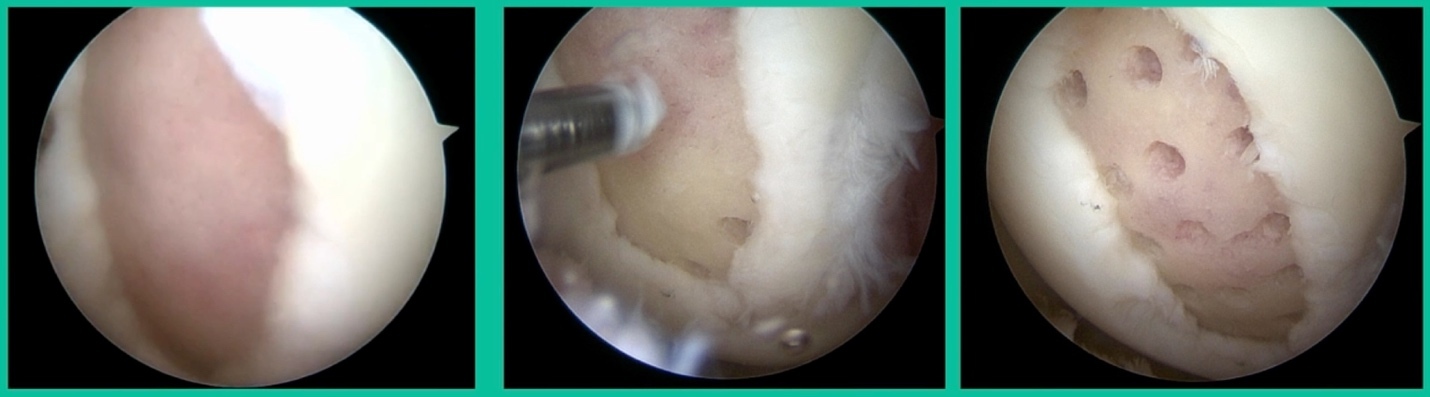
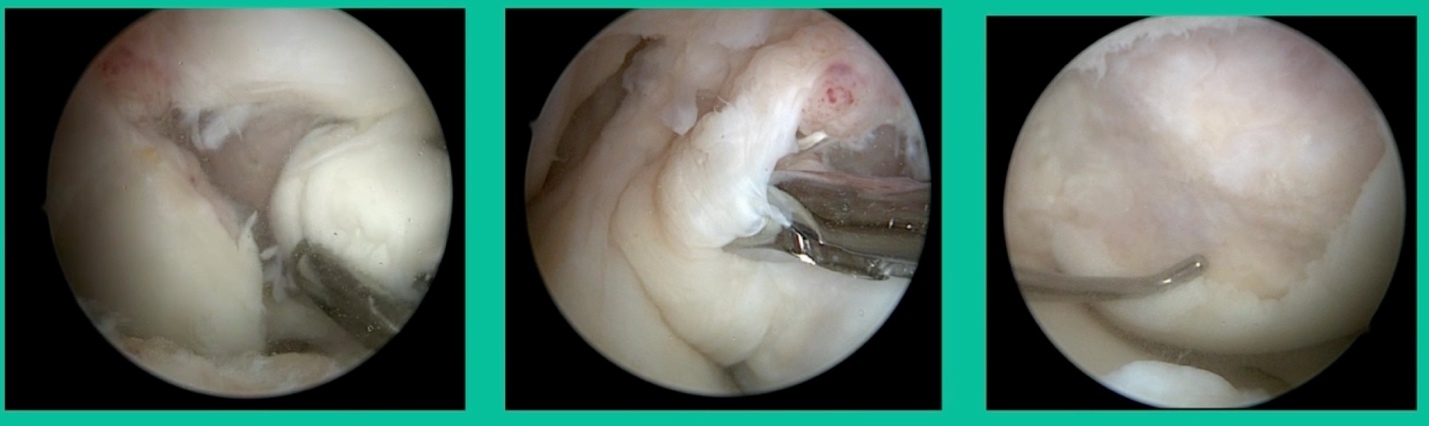
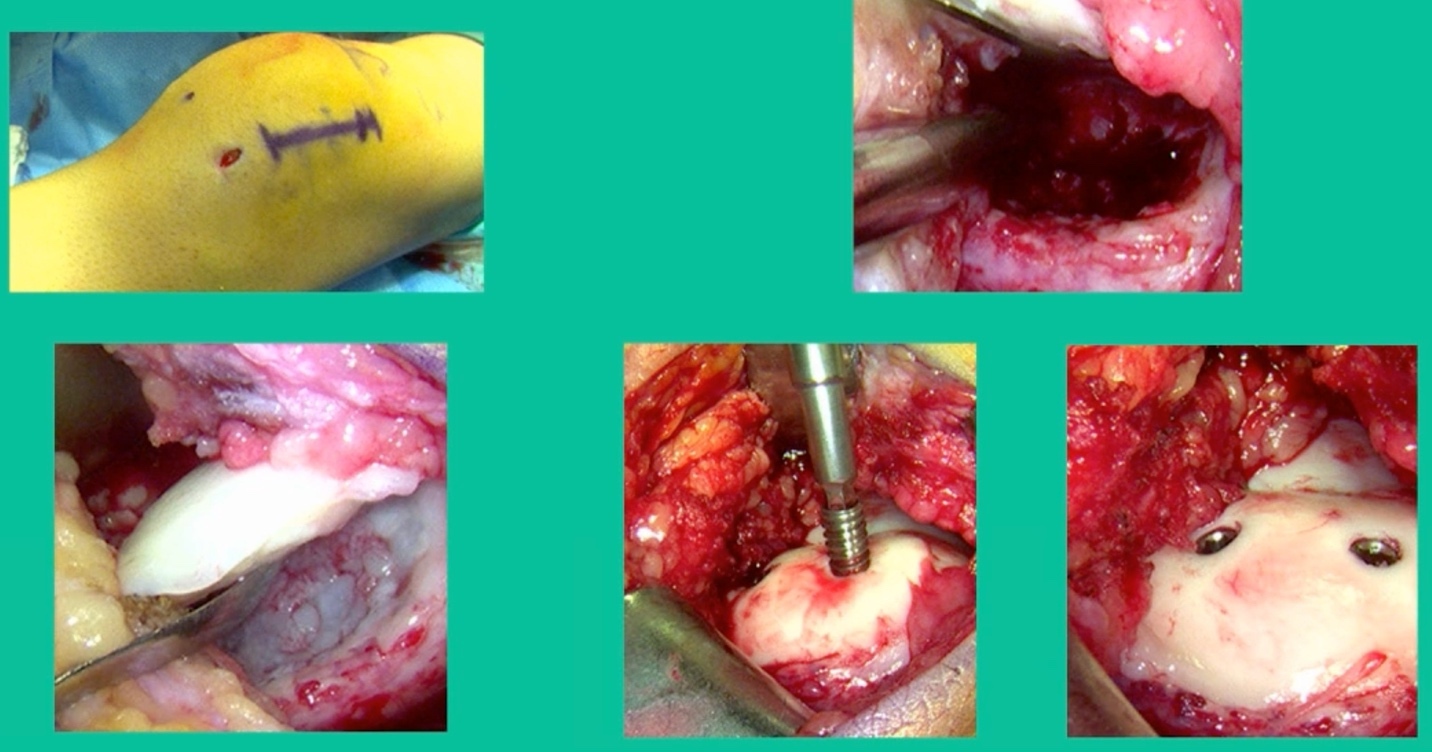
I thought I might be able to fix it. I had the conversation with the family, get in there, started taking it apart with a Vanguard elevator grasper. Behold, it’s really just cartilage fragments (Figure 2).
There’s two or three of them. We debrided it. It felt normal in six weeks, no complaints in three years. What are the results of juvenile debridement? They’re actually profoundly good. You would never expect this in the scheme of things, but the natural history of removing the piece is actually very good in the juvenile patient. However, once again, fix it if you can. Debride it, if you can’t. If they get symptoms, we restore it, and then never leave unstable fragments.
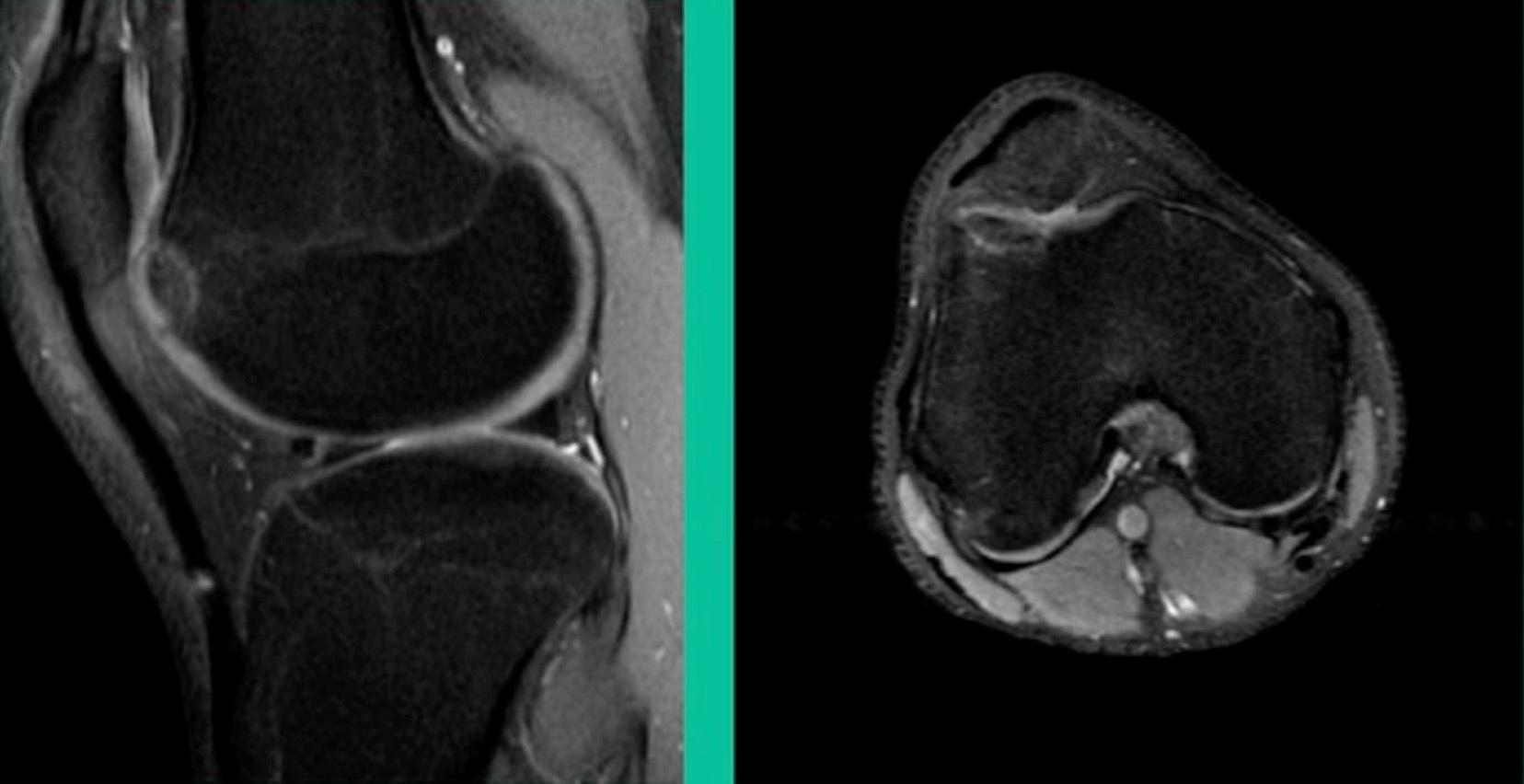
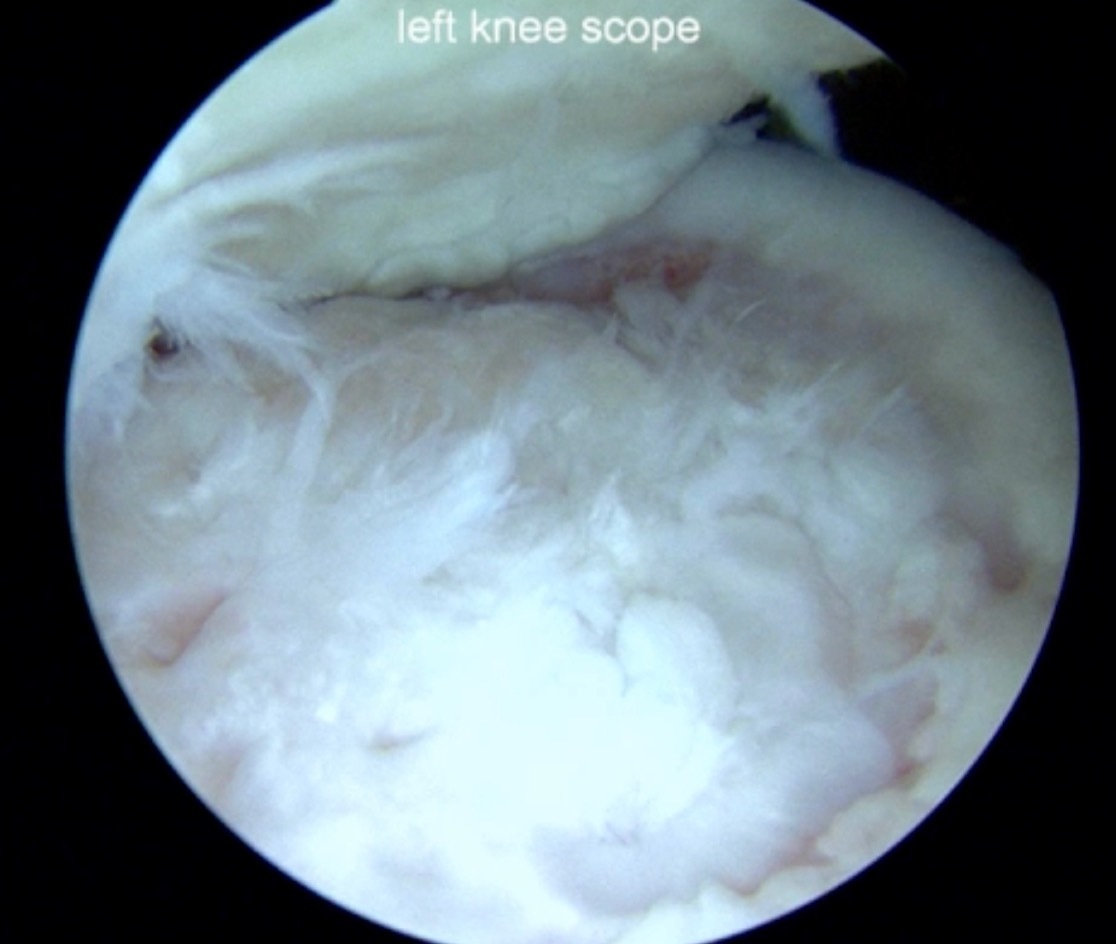
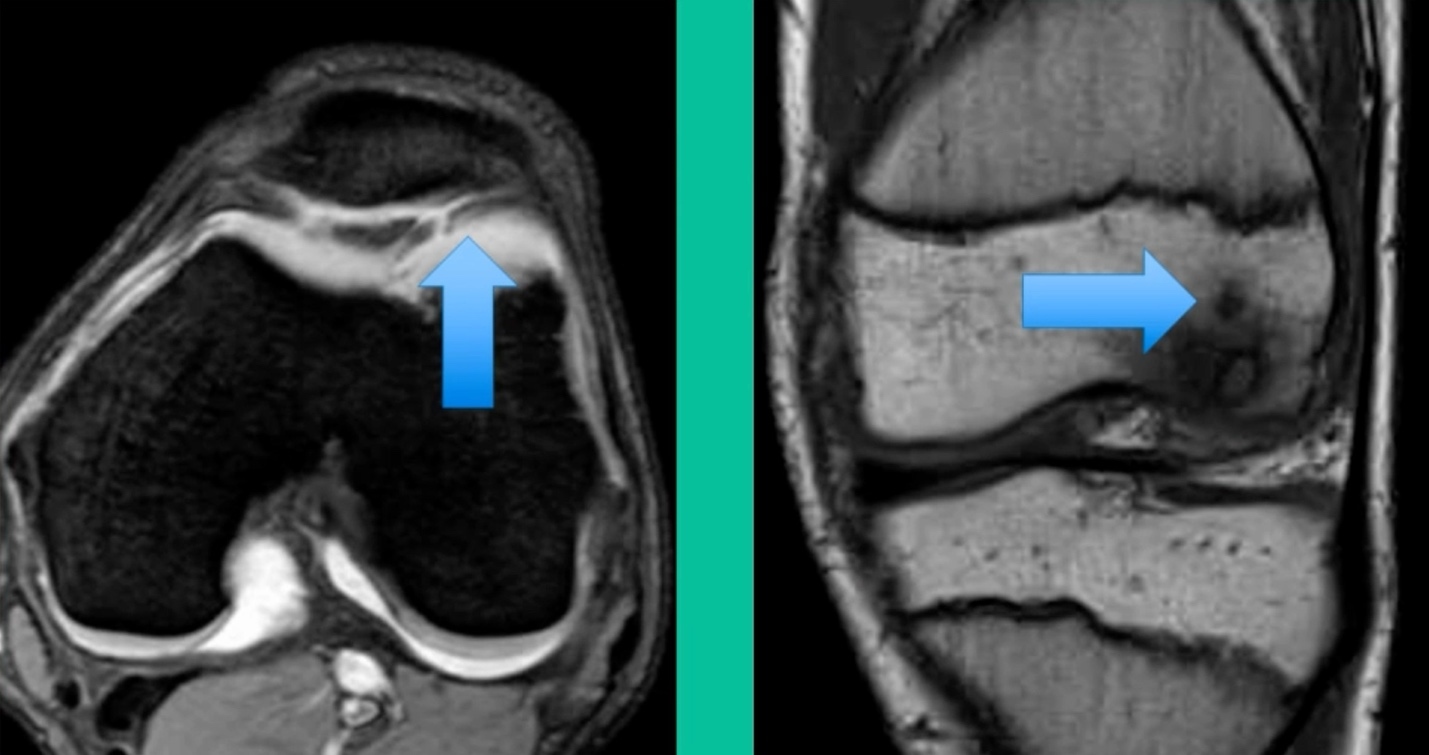
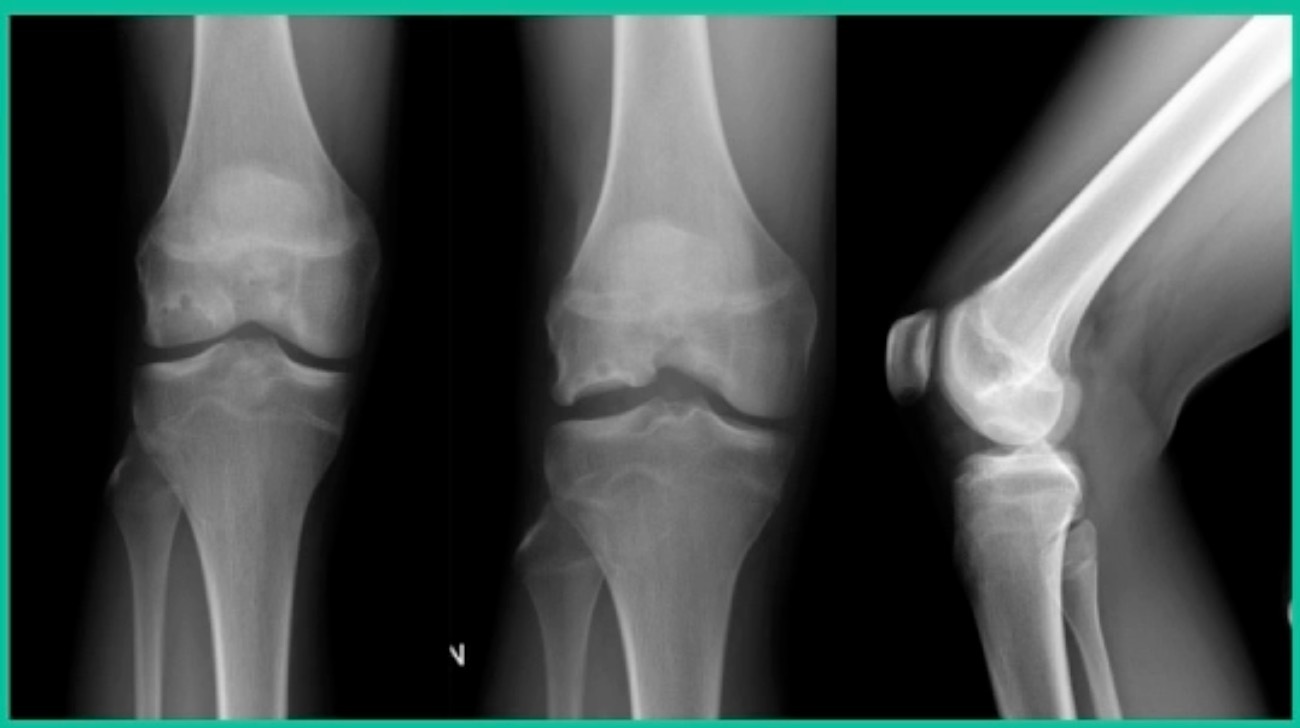
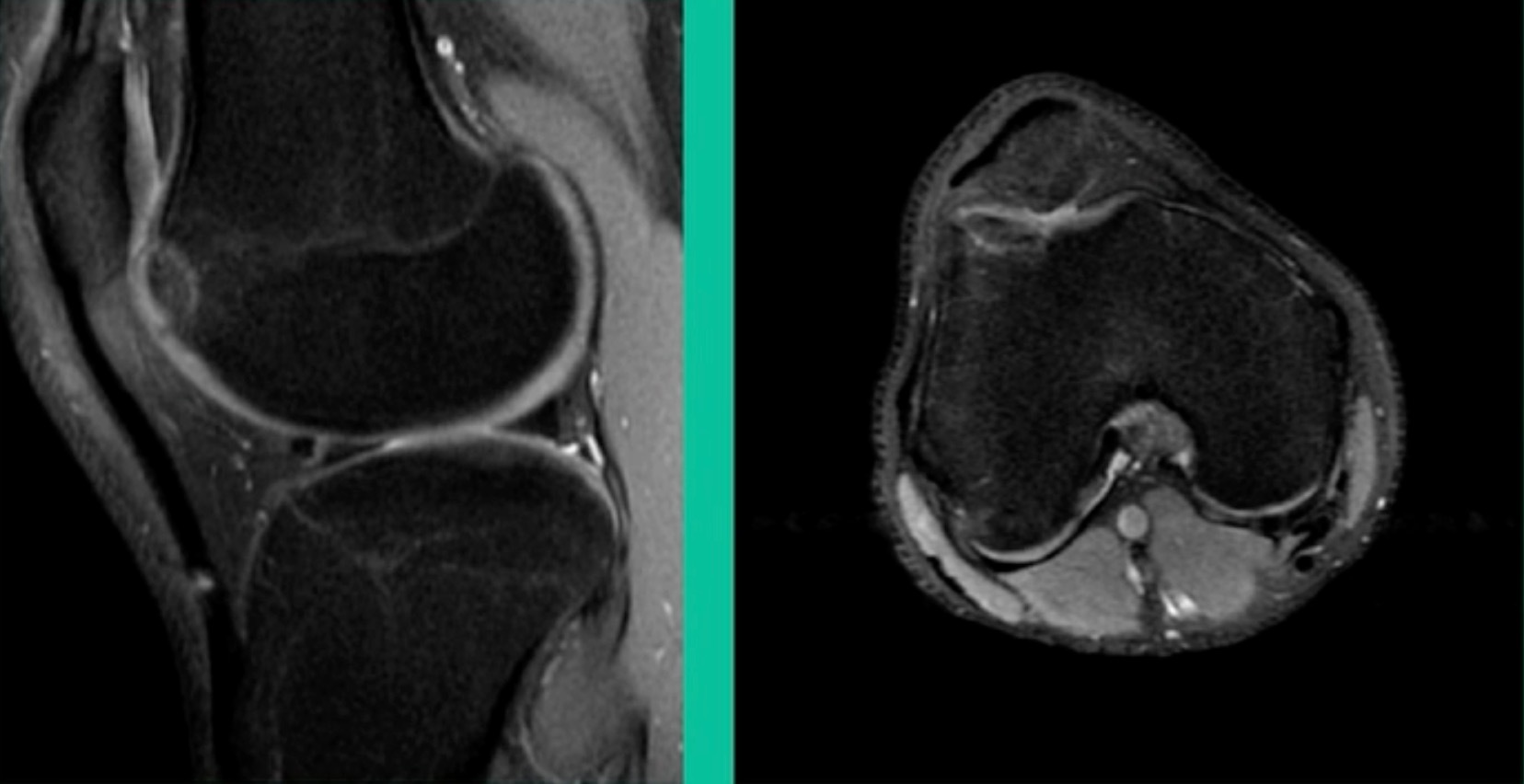
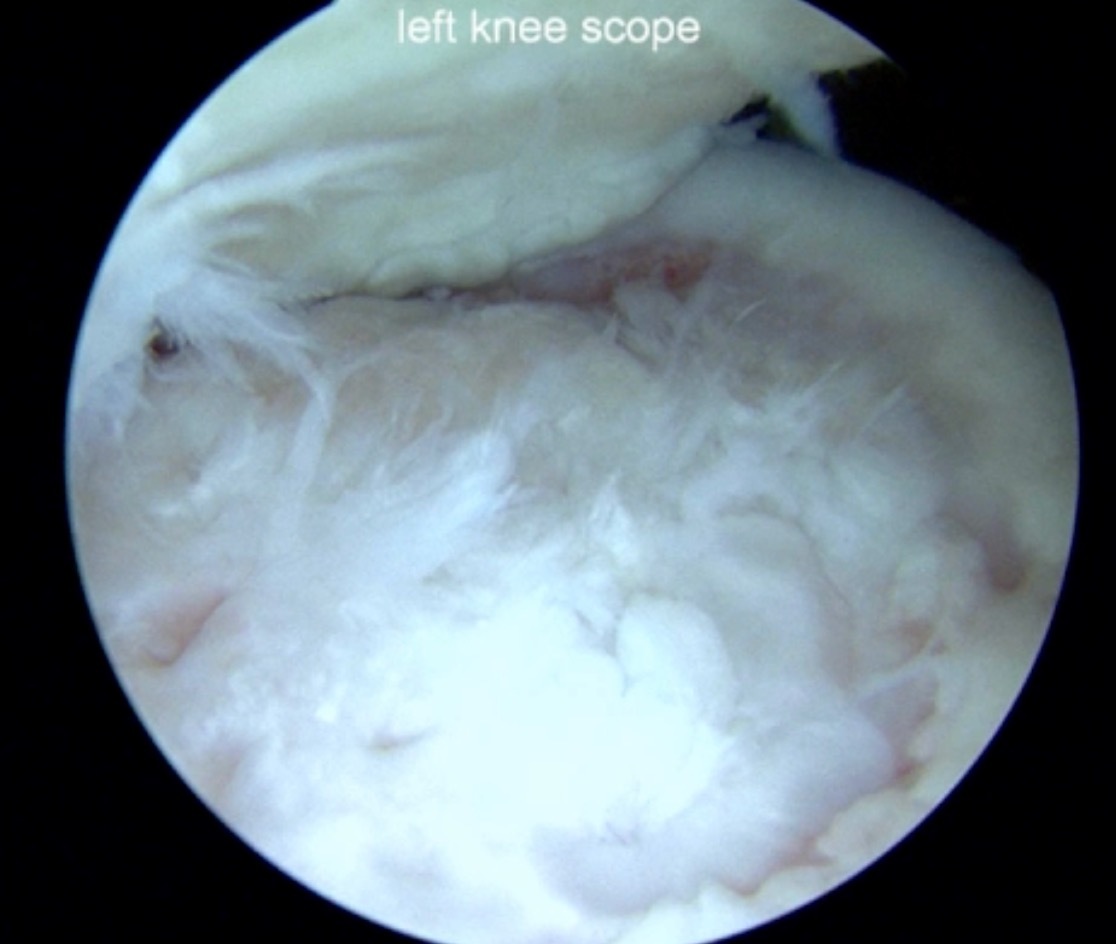
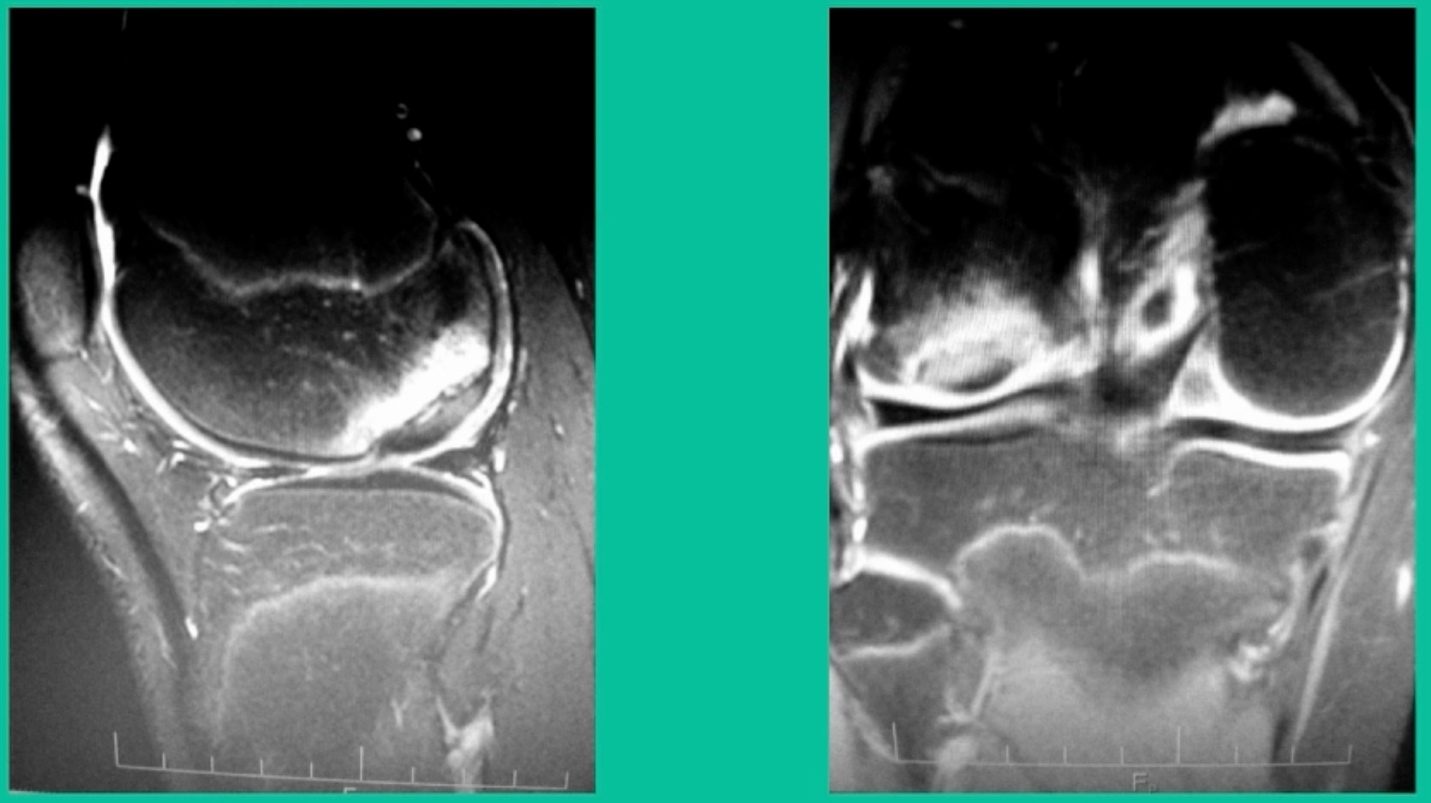
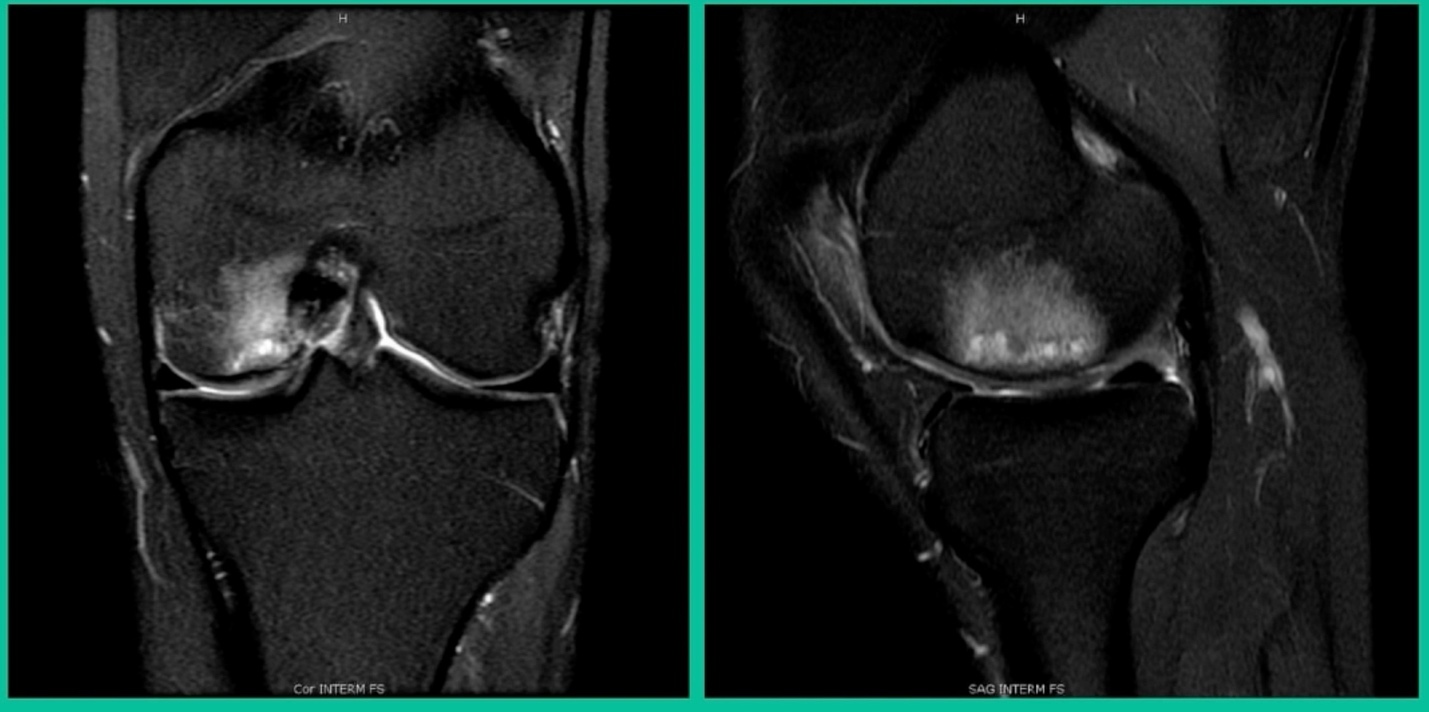
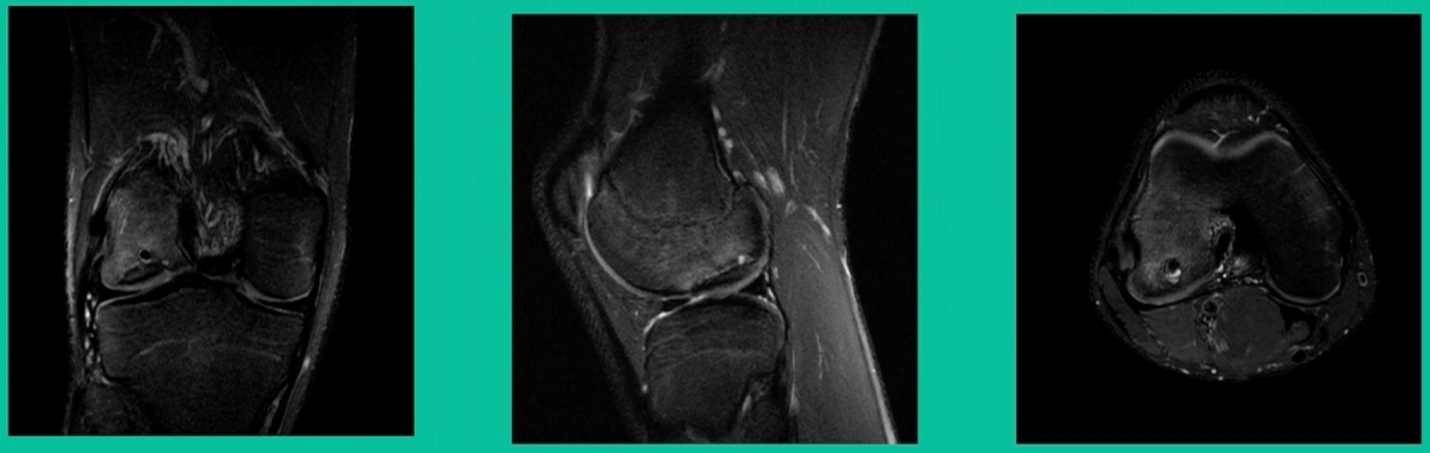
This is an 11-year-old. Left knee lateral knee pain. Effusions, the same type of classic findings (Figure 3)
You look at this one, you say, “what are you going to see when you get in there?” This is one when you get in there, you say, I’m not even sure I’m in the right knee because you almost don’t see it. That happens in patients who were painful, but they don’t look macroscopically unstable. Pediatric orthopedic surgeons tend to drill these. These are the ones that I see as failures. I think when you’re talking about something that’s mechanically unstable, it’s hard to understand why drilling would actually make it work without fixation. Even if it’s microscopically unstable.
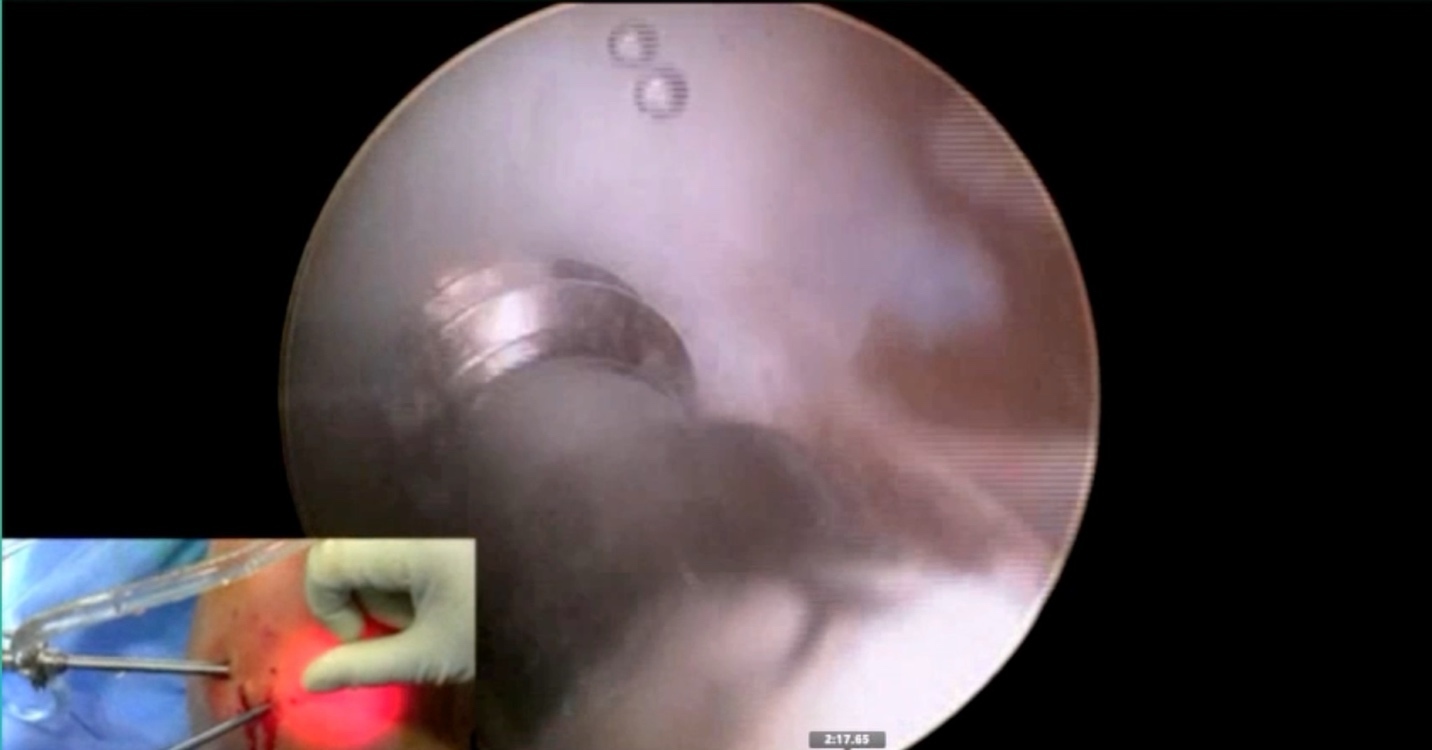
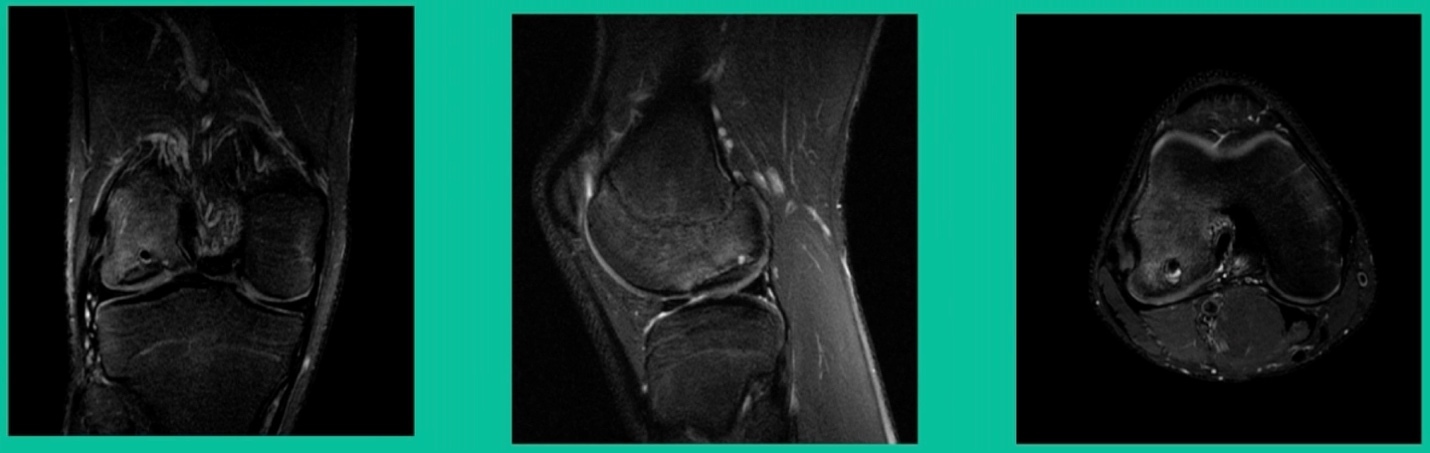
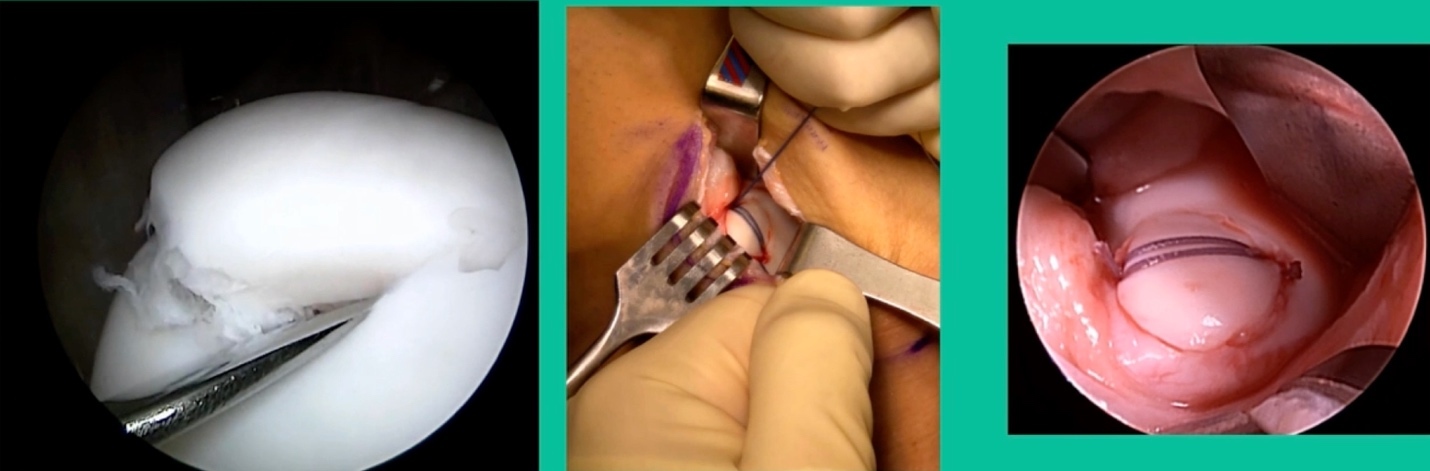
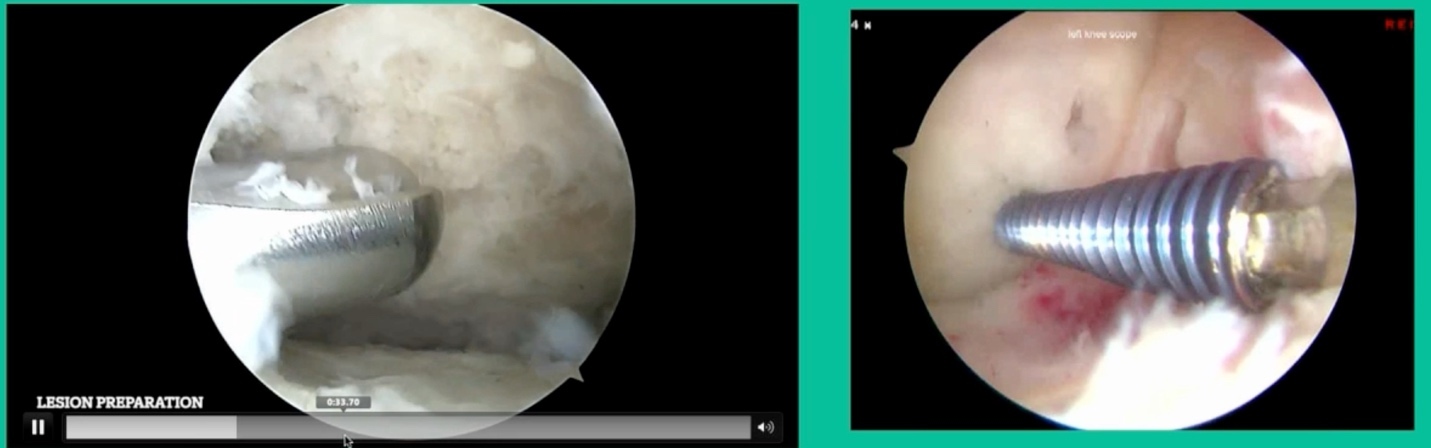
The challenge is this. This series of patients were populated by early decisions to treat when patients don’t have symptoms. That’s a problem in my mind. Post-Op, they protect their weight-bearing. That’s actually treatment. These are often smaller lesions of the medial femoral condyle. They do really well. That being said, it’s an option. It’s not my option. My option for someone who’s macroscopically unstable is we use biocomposite screws (Figure 4).
These biocomposite screws will hang around for upwards of a year. So, they’re not innocuous, and you’ve got to bury their heads. But we drill it, we tap it, and we stabilize it, and then we drill from the side in an effort to promote further biology. This is analogous to just arthroscopic fixation, but I don’t go back, and I don’t remove the screws. Then I’ll typically take a K-wire from the side after I place these screws. I keep them non-weight-bearing for eight weeks. I don’t remove it. I wait four months before they go back to high-impact activities like this patient did here.
What are the outcomes? Very, very favorable. We had 87% survivorship using a biocomposite screw. Would I use it for a macroscopically unstable one? I wouldn’t. I would tell you that the biomechanics are not nearly as good, and it is not innocuous. If you leave the head proud, this will scratch the tibia and cause a railroad track there. You must bury them, but don’t take them out.
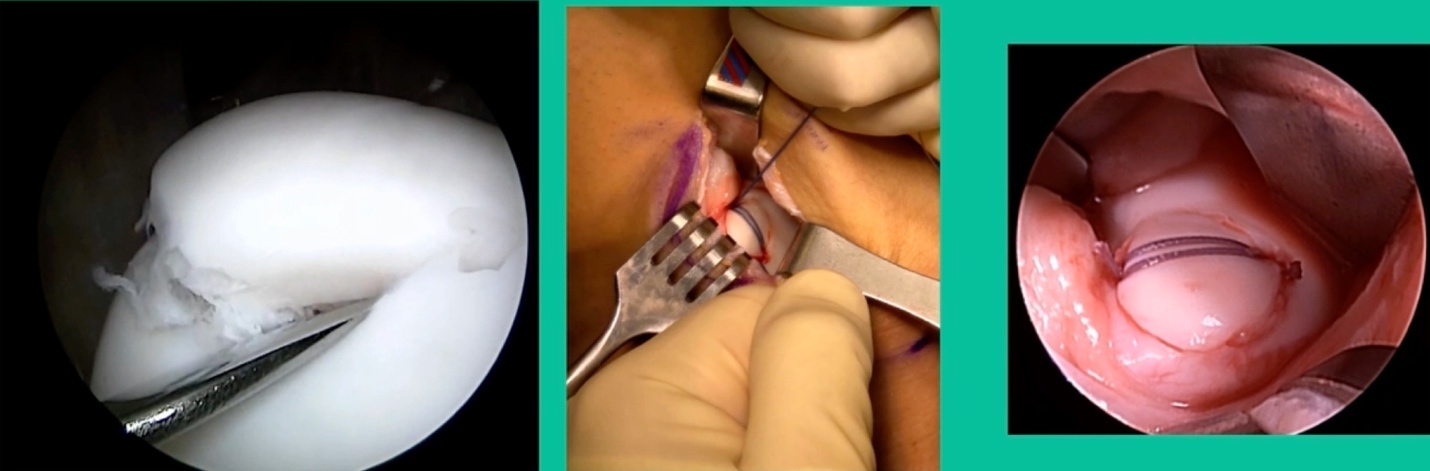
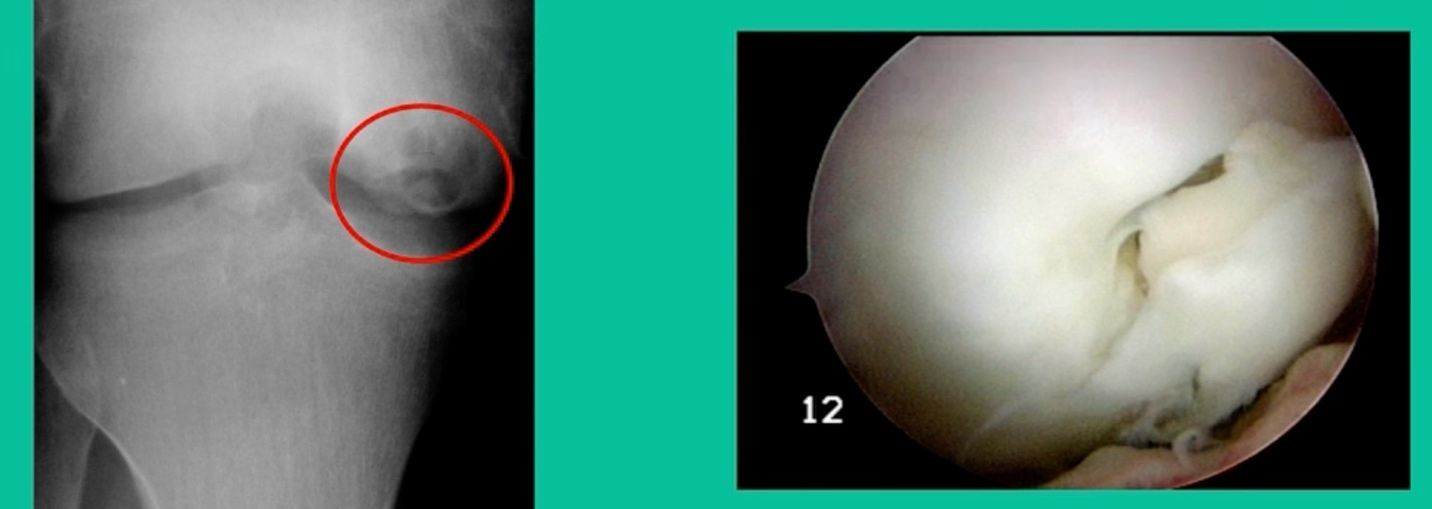
This is another one. 17-year-old basketball player (Figure 5).
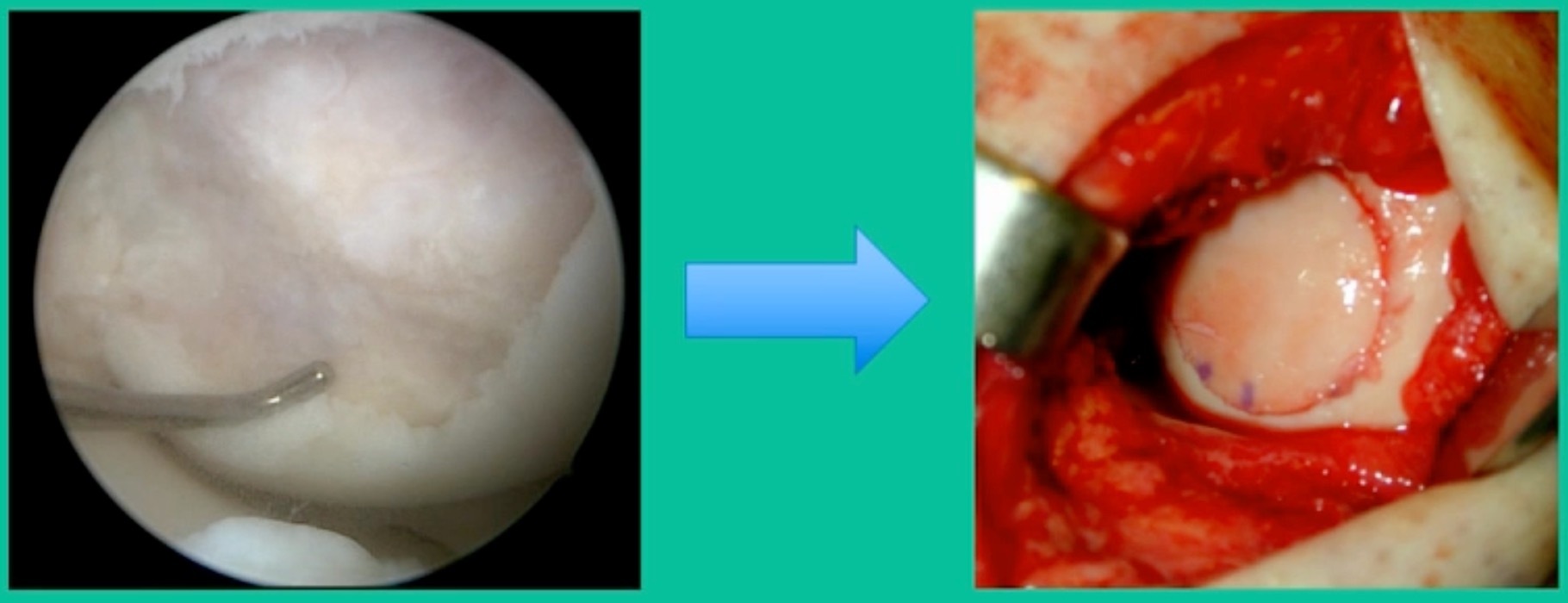
Oddly, this patient had posterior knee pain. I gave him a lidocaine injection because I couldn’t figure out what was going on. He got relief and I said, “Look, something’s going on in the joint. The only thing you got is this trochlear thing.” It was a piece of cartilage. This is all it was.
You can actually, in a young person, get cartilage to heal with no bone on it, and we use compression suture fixation (Figure 6). In his follow-up, five months after undergoing suture fixation of lateral trochlear OCD, he had a little squeaking in the knee because of the sutures there. That actually went away in time. Maybe the sutures ruptured. But he had a squeaking knee for about three months, and then that went away. So, you can fix an all-cartilage problem using a suture compression technique.
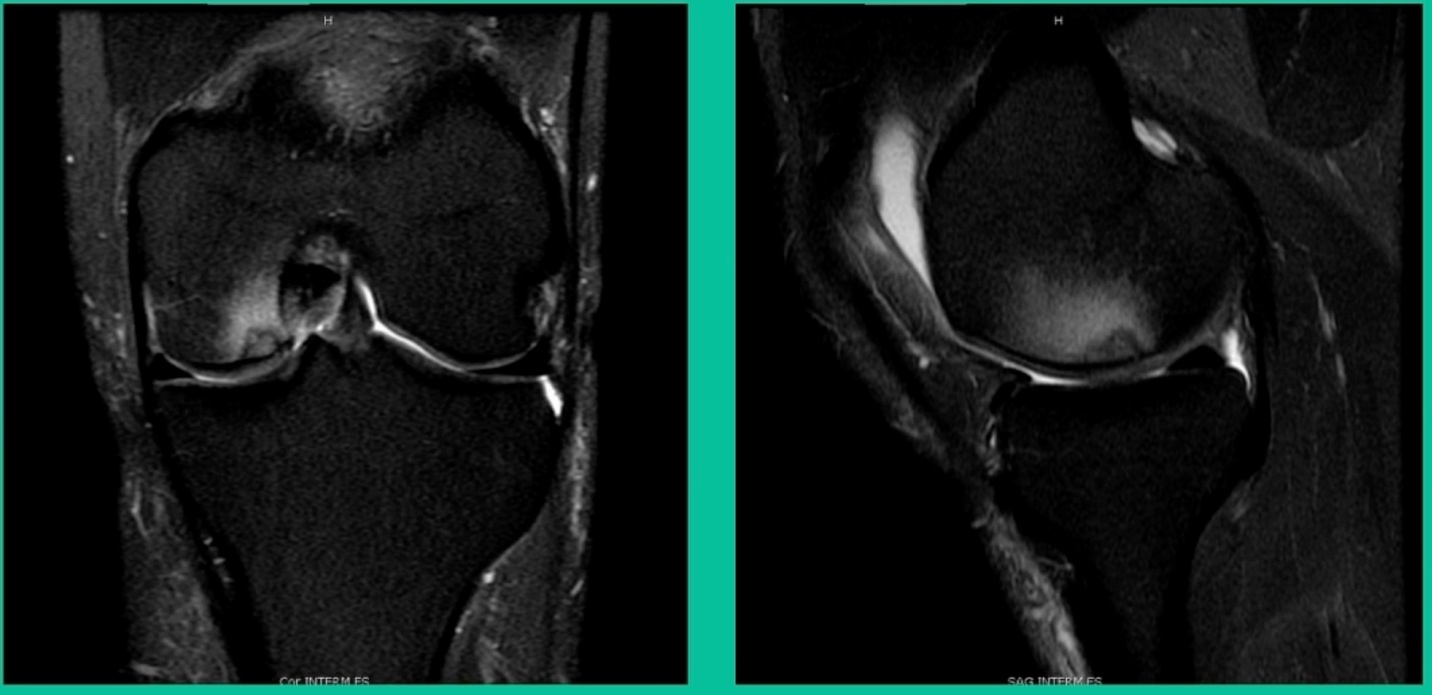
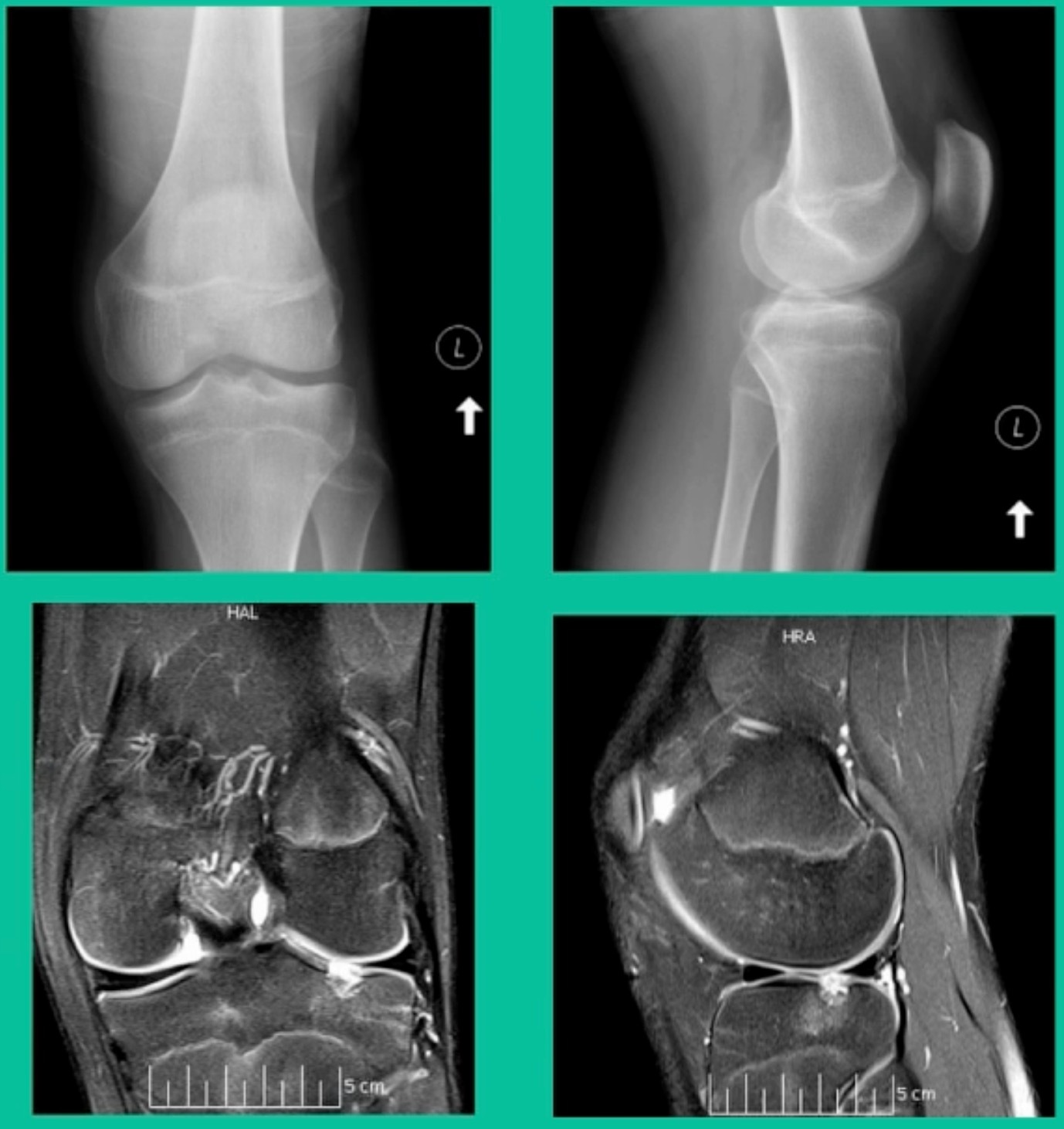
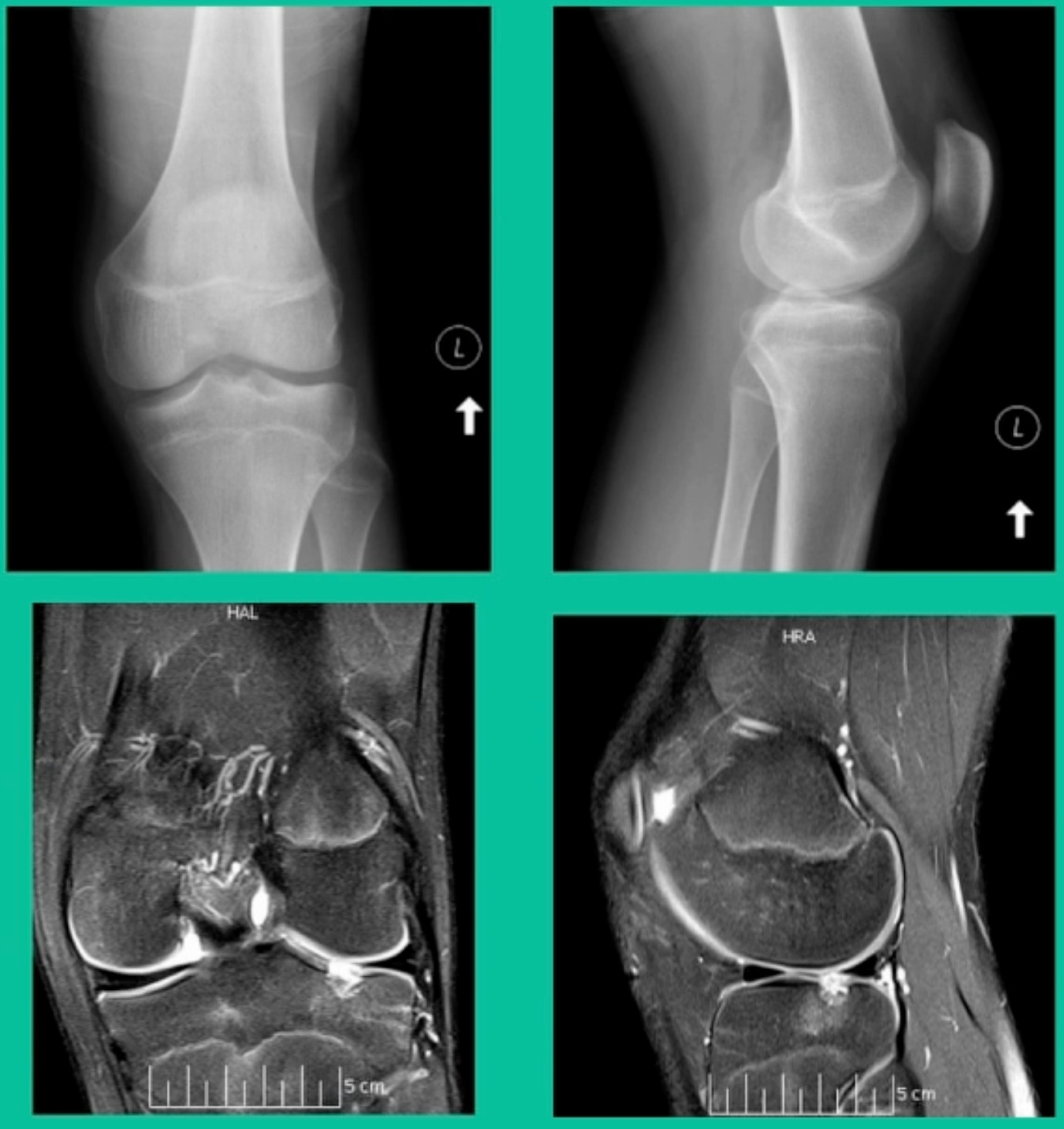
Another case example. 14-year-old male tennis player, 10 months of knee pain (Figure 7A).
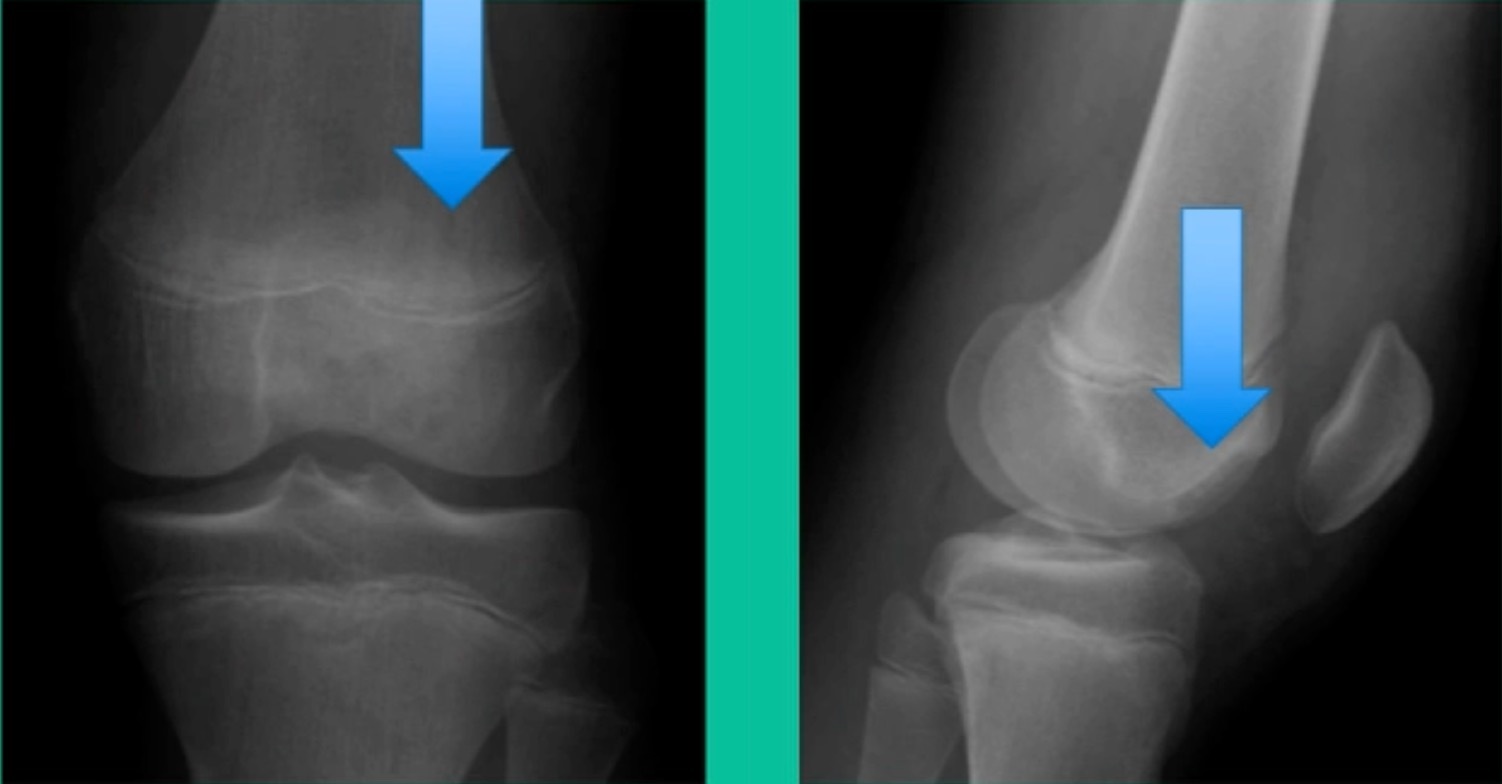
This is a Trochlear defect (Figure 7B).
This goes back to metallic screw fixation, because this one is macroscopically unstable. That is a fracture non-union. That’s an atrophic non-union. Debride it, curette it, drill it, and thenwe use metal screws because it’s macroscopically unstable.

However, in this instance, we did take the screws out.

He was back to everything at 16 weeks and, at two years, he had no further symptoms. How do these do? There’s plenty of literature that shows that metallic screw fixation for unstable OCD, not just in juveniles, but in adults, will lead to reliable fixation. It’s a four-month process. They get back to everything, and they rarely have problems downstream.
Now, we’ll shift to the adult. This is a 27-year-old. Right knee swelling, activity-related, and classic failed nonsurgical treatment on the lateral side of the knee.

This will probably be fixed. It’s a big piece and we’ll try to preserve it. The literature shows that preservation does pretty well. In this instance, there’s very little bone. It’s somewhat dystrophic, not very encouraging in my mind.
We removed it, and you say, “Well, this is terrible.” Lateral side, how is he going to do? Interestingly, the natural history does not suggest that that person will do badly. Probably the worst ones are going to be the ones who fall off to the side into the trochlea and lateral meniscus.
43-Year-Old, symptomatic medial femoral condyle.

D1 football player formally, affecting ADLs. For this one, I initially just wanted to watch it. This looks pretty small when he came in. Let’s see what happens. Six months later, this is where he progressed to.
We get in there, it’s delaminated, not much bone, nothing to fix in my mind, and so we drilled it.
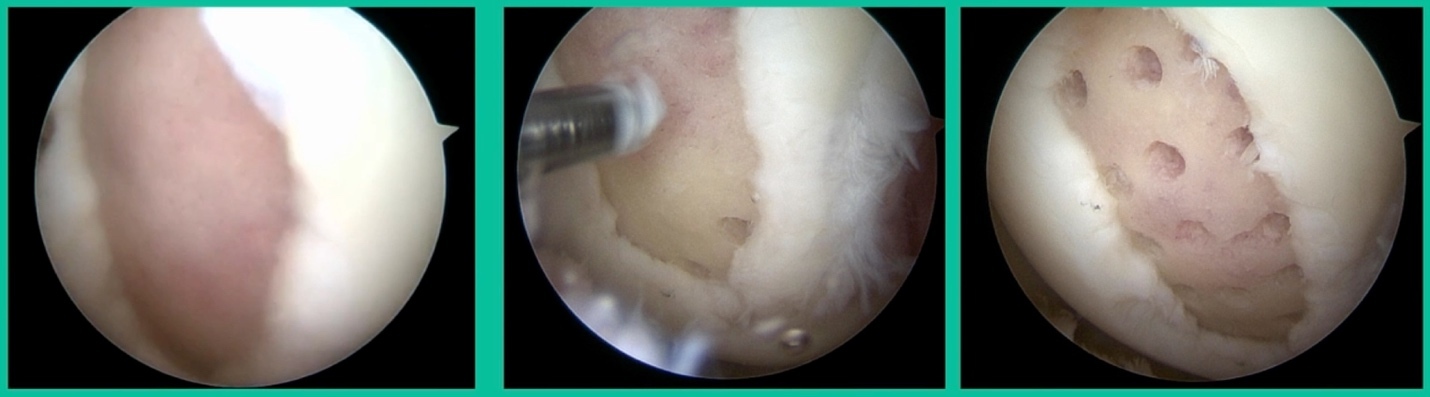
How do these do? There’s actually reasonable data for marrow stimulation for OCD. But if you have the option for small defects, I would prefer an osteochondral allograft over microfracture based on the literature. That’s the take-home. Marrow stimulation, if you do it, you’re probably better off drilling it. We showed that we could reduce revision rates with marrow stimulation by two-thirds if you drill it versus use a microfracture awl.
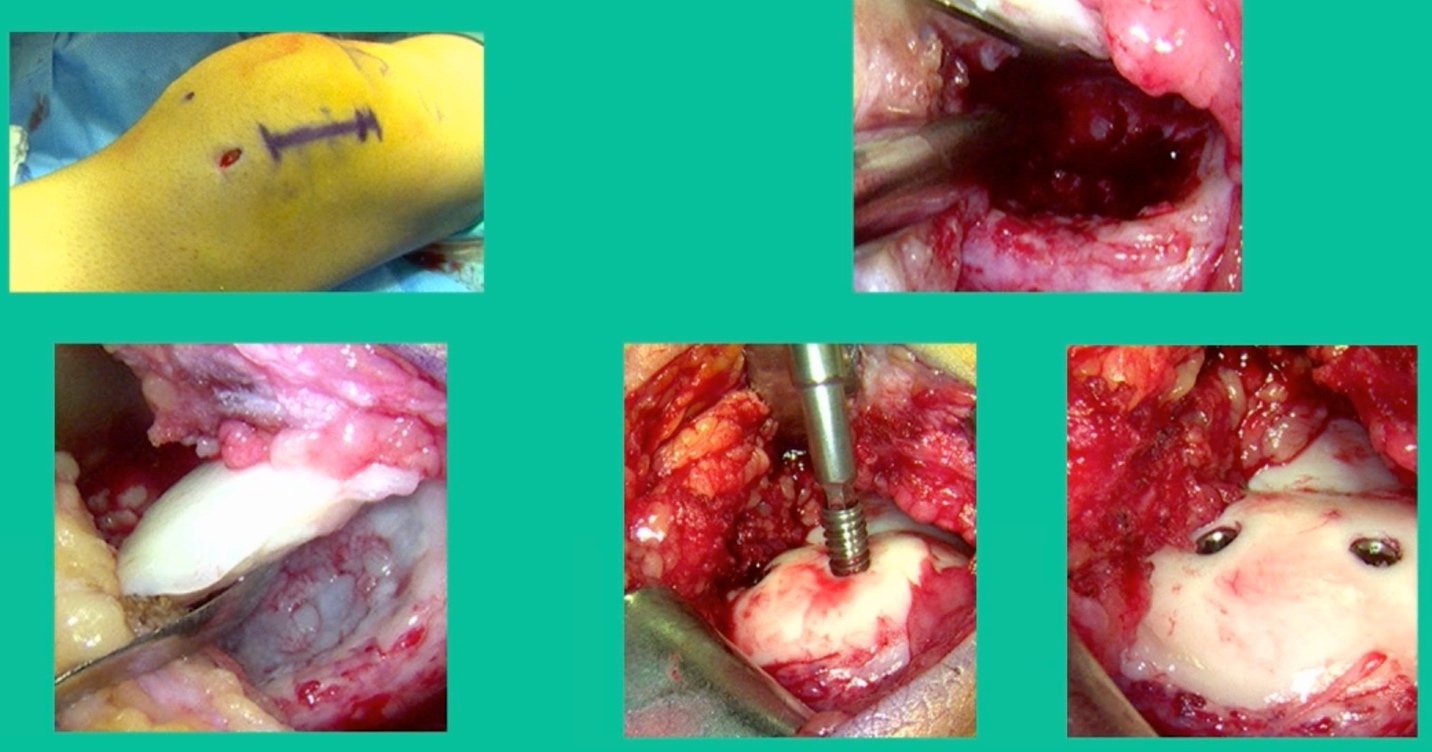
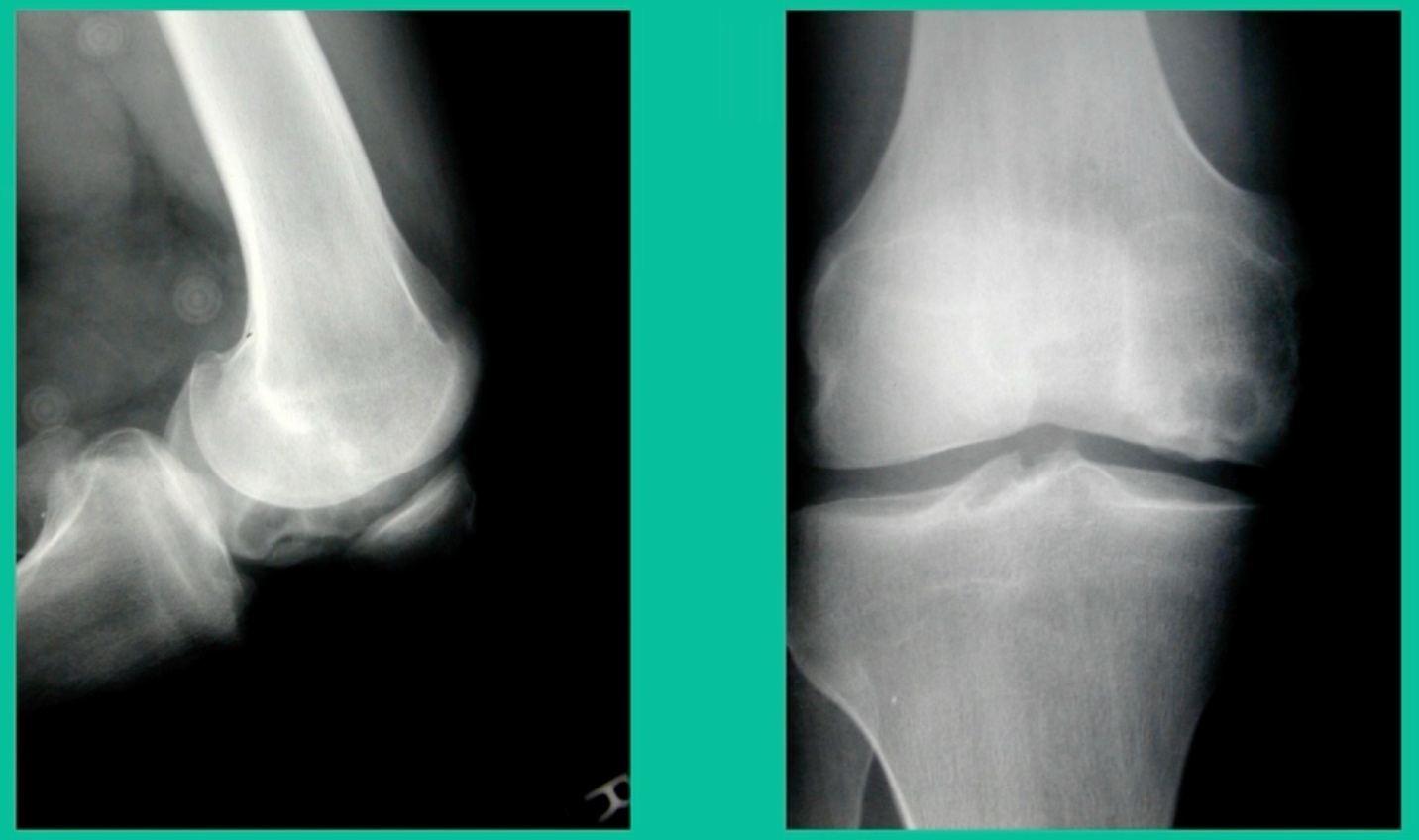
This is an 18-year-old with a lateral femoral condyle OCD:
Worsening over the last two years, has effusions but no locking, and has a large area of involvement that appears unstable. This is the classic fixation. If you can do this, this is the holy grail. Remember, fracture non-union: you elevate it, debride the base, get rid of any unstable fragments, just take them out, and preserve the major fragment. I’ll use a microfracture awl, but most commonly now I’ll use a pick or a pin, and I’ll drill it. I use two to three metal screws. I bury their heads, and then I come back at eight weeks after being non-weight-bearing, and pull the screws out.
Afterwards, I’ll allow them to fully weight-bear, wait eight more weeks, and then they go back to full sports. How do these do? Amazing. If you can get this to heal in an adult, this should last hopefully forever. The results over here show 80 to 90 percent healing rates in most series.
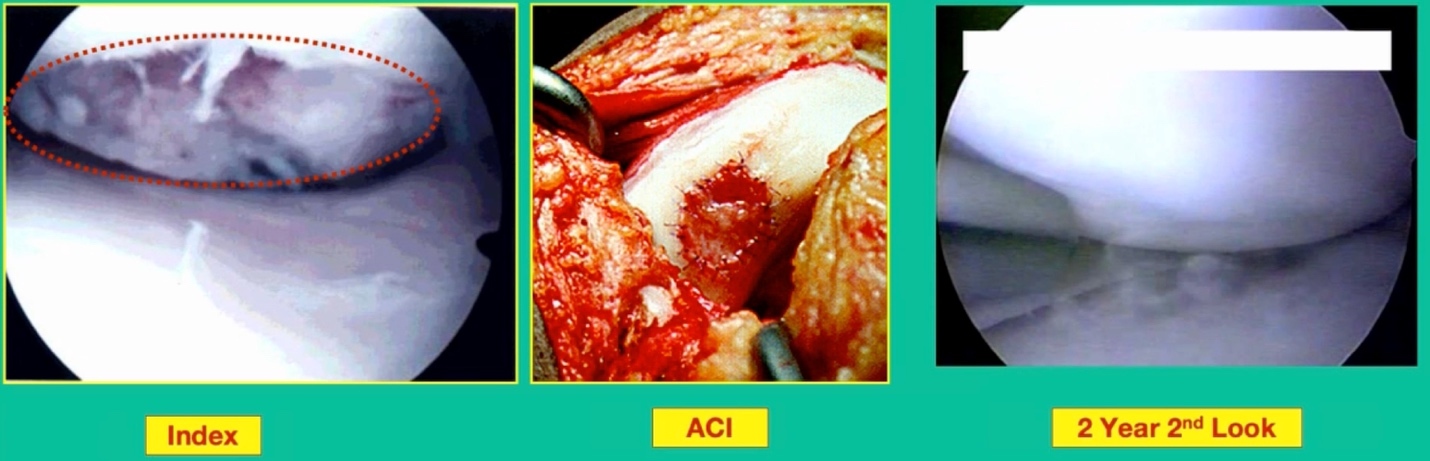
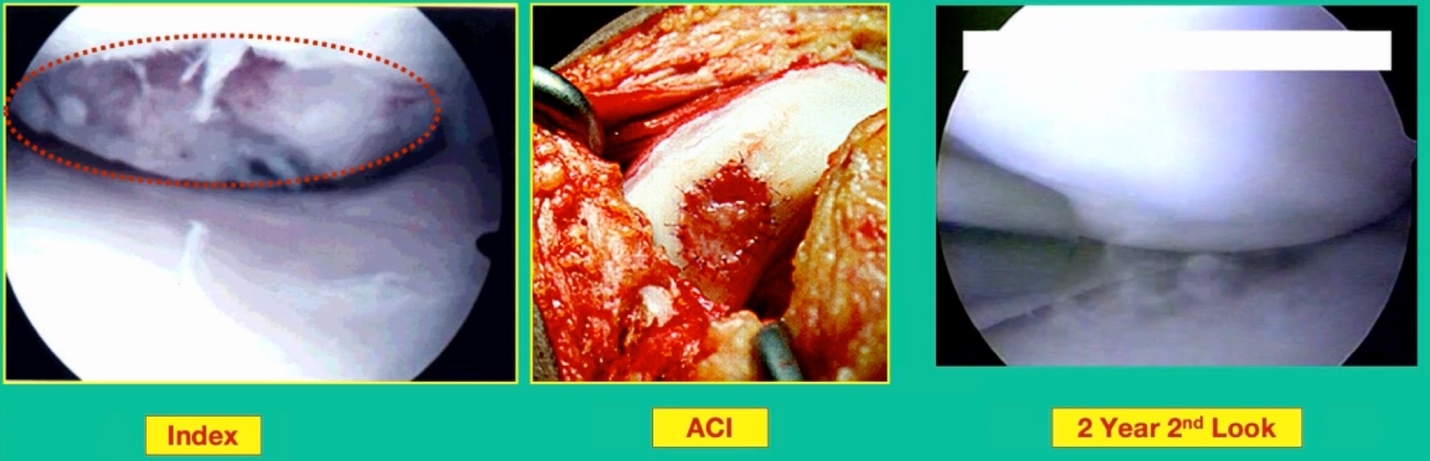
What happens when they fail? What do you do when the piece isn’t fixable, they stay symptomatic, or the piece is fixable, but later on it becomes unsalvageable? How do you manage these patients? Two options. This is one option. This is one who had a primary repair of a cystic lesion. I removed the piece and they remained symptomatic early on, so then I performed an Autologous Chondrocyte Implantation (ACI).
This one actually did very well following the ACI, despite having the radiographic appearance that you see here at four years.

ACI will never look as good as this autologous cell transplantation. This is still, to date, the best one I’ve ever seen. That was a guy who had OCD and failed standard ACI. That was when we used to use periosteum. What about if they have a lot of bone loss? Tom Minas and others have popularized the sandwich technique. To me, this is a long haul for a short slide. I’m not sure doing bone grafting and ACI makes sense in this instance, but the results can be favorable.
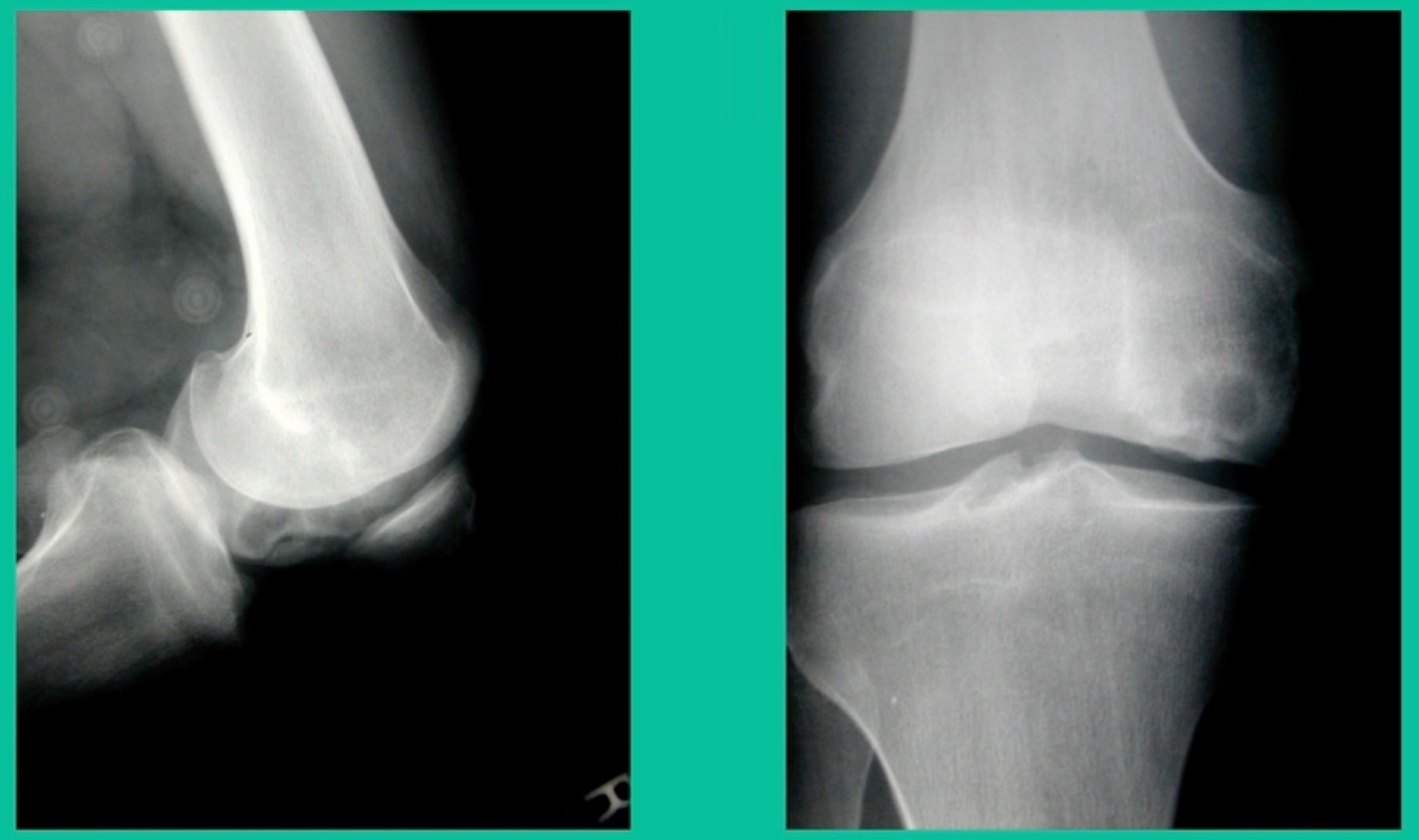
Another one. 24-year-old right knee pain, ADL discomfort, normal alignment, lots of symptoms, thought I might be able to fix it.
I get in there, the pieces are just fragmented, I’m not going to fix it. This is the lateral aspect medial femoral condyle. Statistically, this one can do well. You take the piece out, they say, “I feel better.” It’s on the upslope of the lateral aspect medial femoral condyle. They feel fine, right? That’s not the case here. This one still continued to have symptoms.
So, what do we do for this one? This one got an osteochondral allograft.
I gave you a whole talk earlier on today about OA grafts. This is my mainstay for a salvage. I do not pull this out of the bag when the patient walks in the office for their first-line treatment. First, they get a scope. If it can’t be fixed, it comes out. If it can be fixed, we fix it with metal screws if it’s grossly unstable. If it’s not grossly unstable, we use biocomposite screws. If they get fixed, they go back to sports in four months. If they fail, they generally get this (Figure 28).
The results of osteochondral allograft in juveniles and adults, that’s the left and the right here, have been uniformly good. In juveniles, we get up to 90% success rates. Same thing for our adult onsets, a little bit less favorable. Even athletes can return to sport after an osteochondral allograft. Now we have 36 professional athletes that have had an osteochondral allograft who have gone back to sports. Some of them have had a meniscal allograft. So, salvage situation, you never make a promise, but it can’t happen.
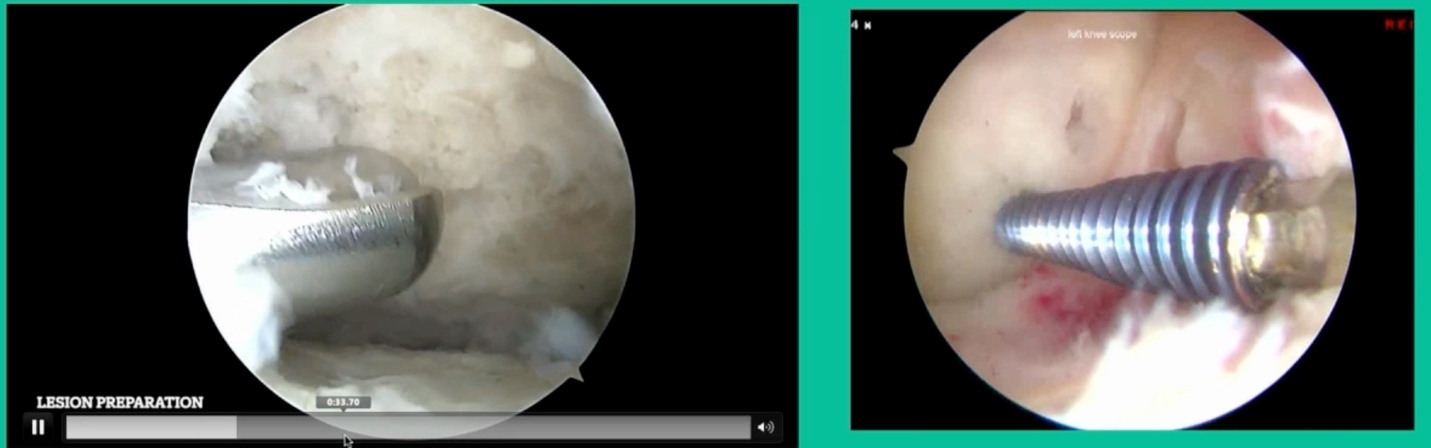
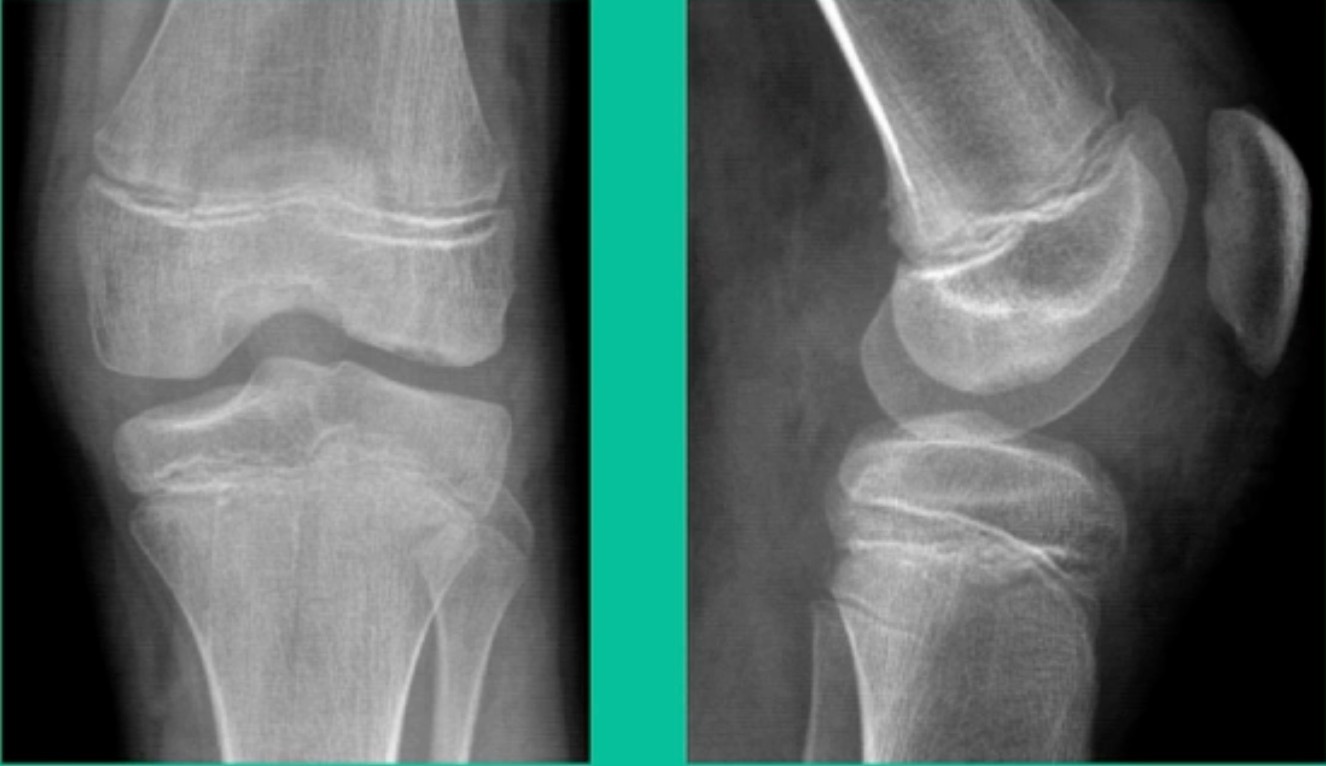
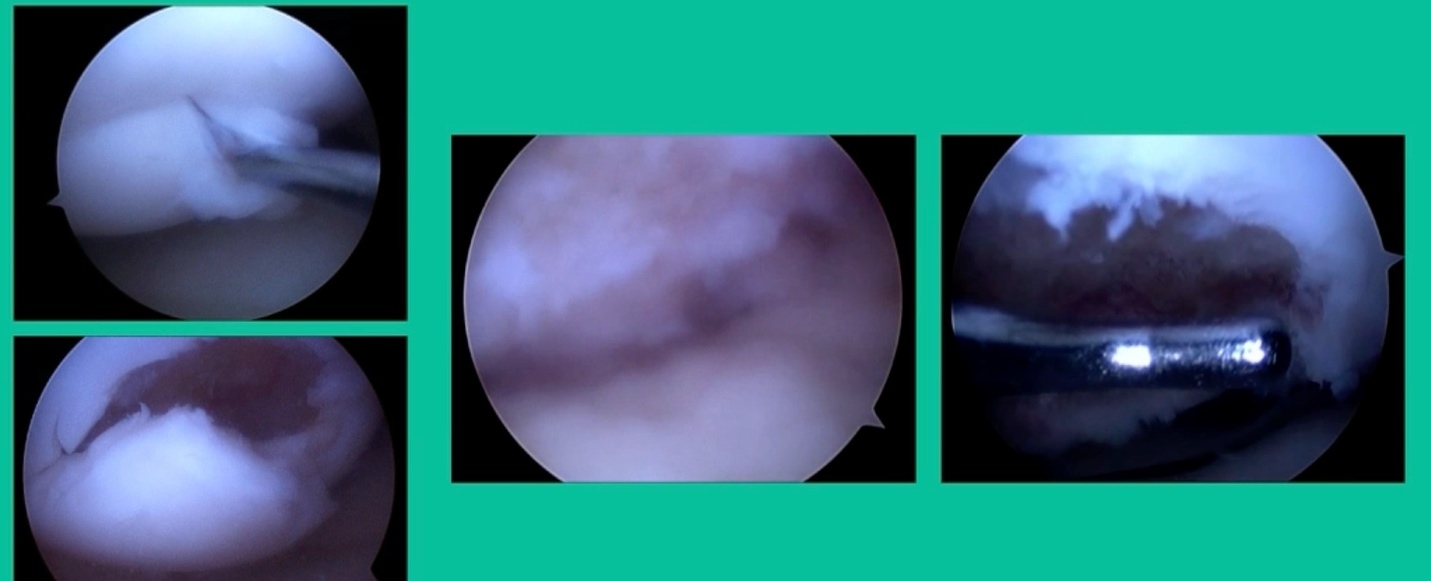
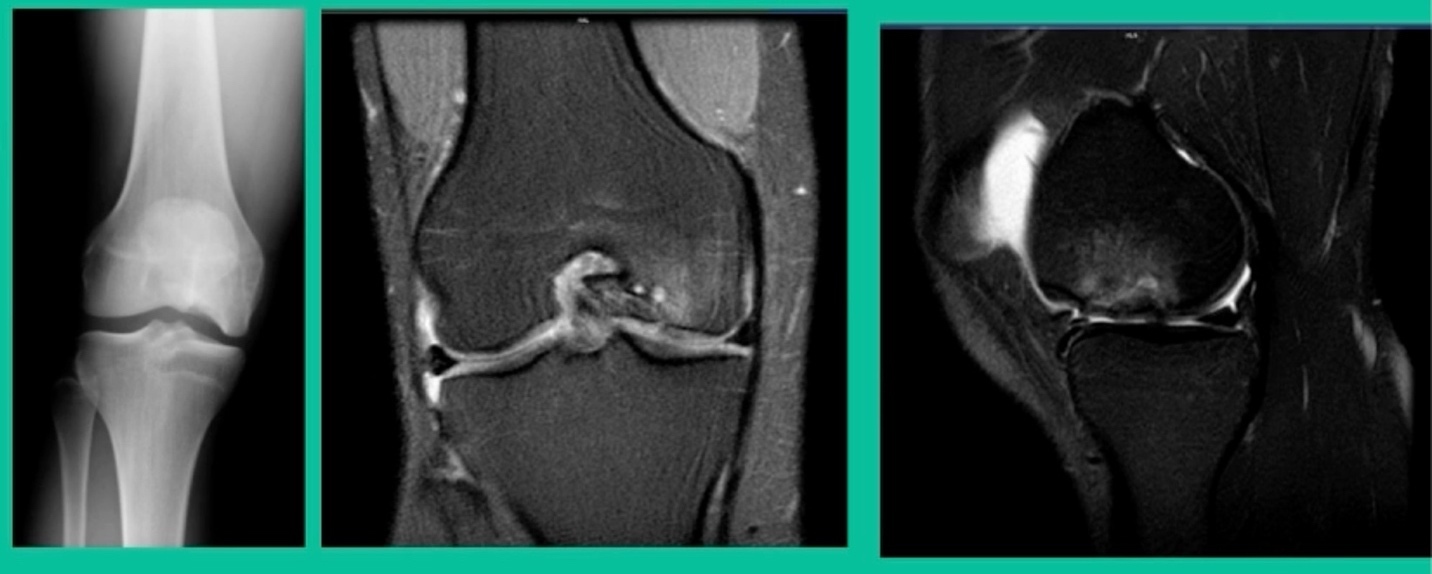
The last problem is we do occasionally see these in the tibia, and fortunately, we have solutions for the tibia. What did I do early on? This is a 15-year-old male runner.
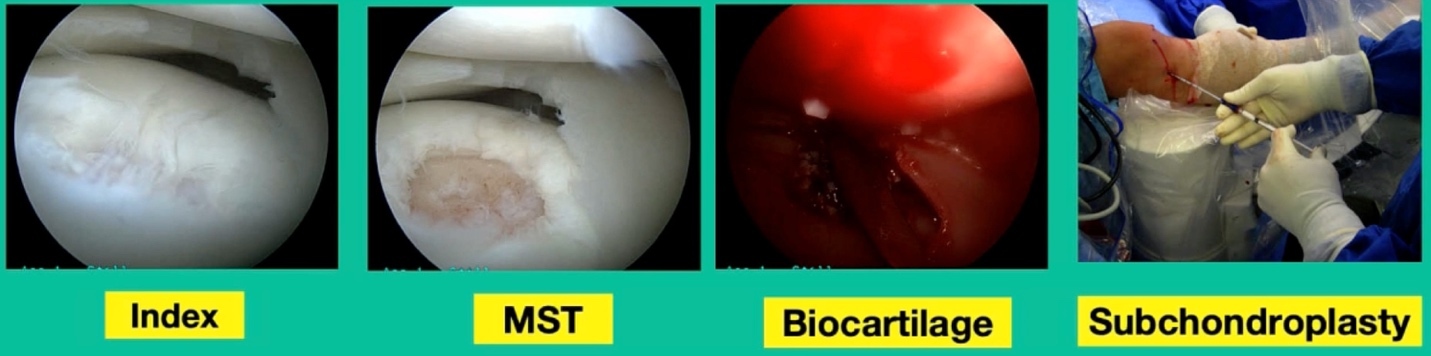
Lateral knee pain and swelling, failed microfracture the tibia and so we did biocartilage.
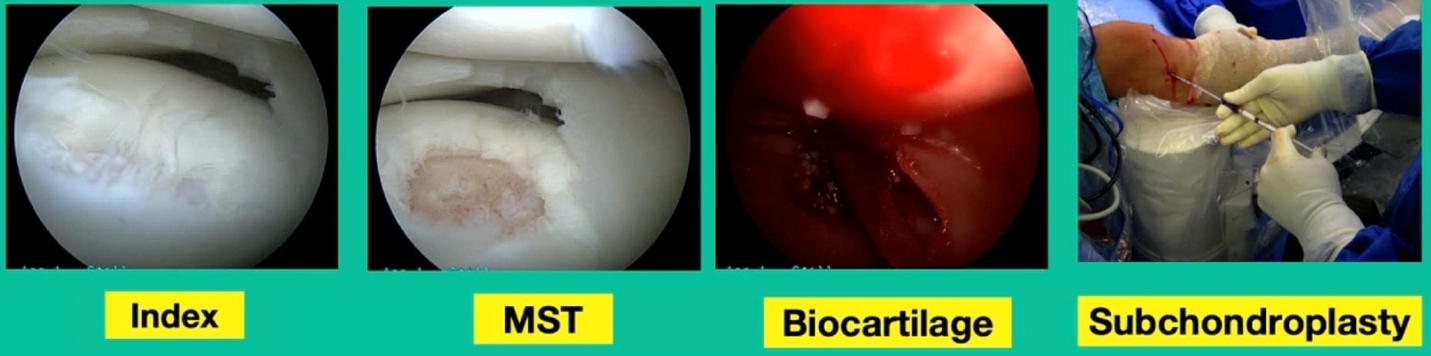
This is basically lyophilized collagen taken from allogeneic cartilage, and we put it in arthroscopically with some fibrin glue. Then we did a subchondroplasty. That was my early treatment. Now, we’ve evolved. What do we do?
This is another one. 38-year-old, lateral side knee pain, lots of edema.

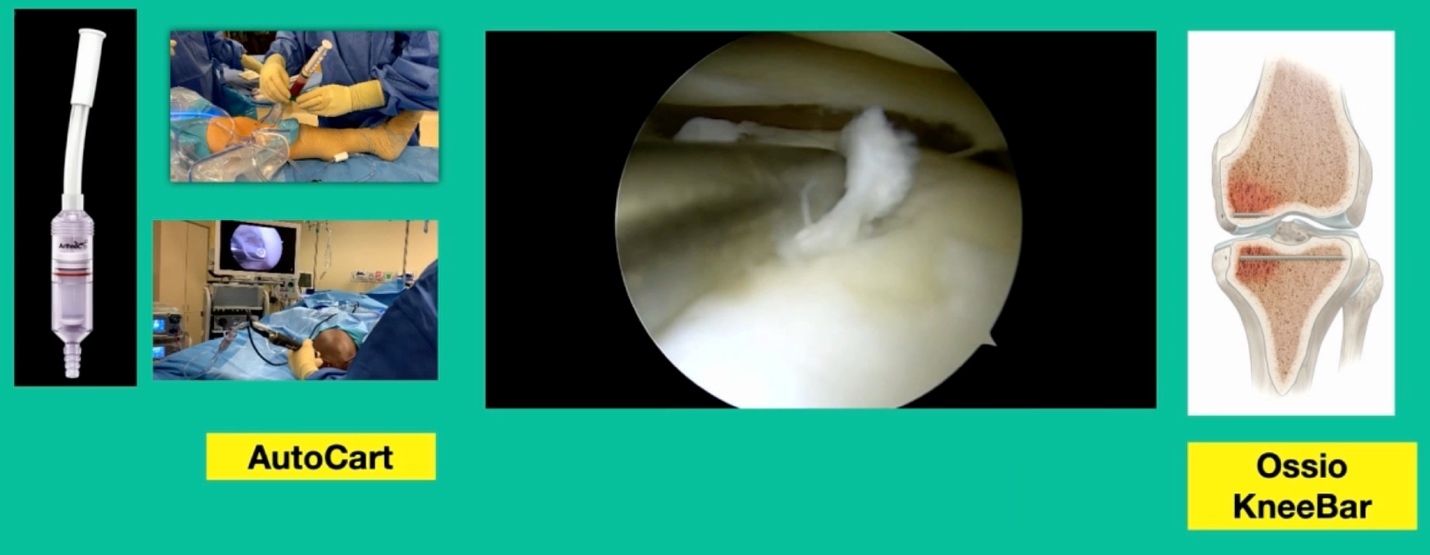
What’s amazing with this one is he’s got that little focal defect, but tremendous edema there and lots of bone pain. This one, we did something called AutoCart™ (Arthrex, Inc.).
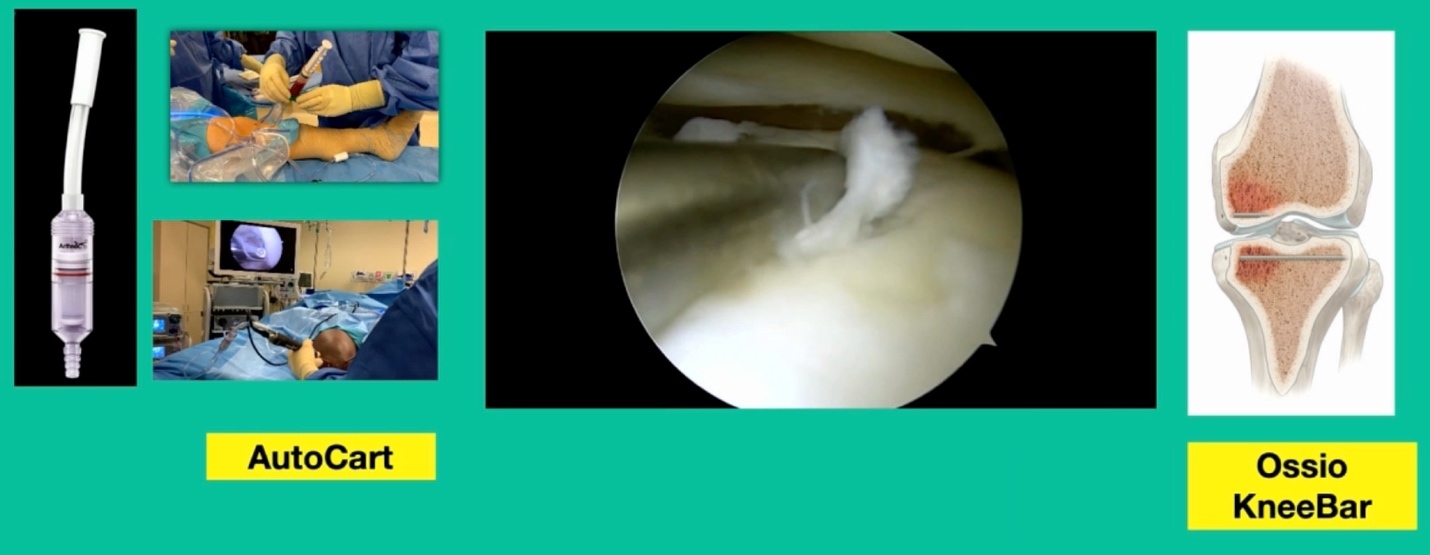
Now, it’s an interesting procedure, and it’s sort of a poor person’s cartilage transplant. We take advantage of the body’s innate ability to heal. That’s the lateral tibial plateau and we’re curating the base of it. Using a shaver we grab cartilage from the intercondylar notch and we collect it in a little receptacle (that’s collecting the cartilage).
We then make this sort of “witches’ brew” of articular cartilage, which is living articular cartilage, some collagen, what we call bio cartilage as a scaffold, and bone marrow concentrate, and then we create a paste. Then, arthroscopically, we introduce it, and we put fibrin glue over it. Then, to treat the edema, we do something called OssioFix or KneeBar (Ossio Inc.) where we take a biocomposite pin. It’s like a rafter screw, and we put it across the tibia to shore up the tibia. We have now about 20 patients who have been treated this way and it can be very good because we’re treating the bone and the cartilage.
In conclusion, OCD is a fracture non-union. They hurt when they become unstable. Some will heal without surgery. If you do surgery, the order is successful repair, followed by excision, followed by restoration, followed by fragment retention, which is really something you don’t want to do, because this is not going to get them better. What’s interesting is the natural history of “nobody home,” meaning you take the piece out, is actually pretty benign. It may take several steps to get it right, and in the end, the osteochondral allograft will likely solve the problem.
To those of you who do total knee replacements: can you recall how often you see a patient come in who has had OCD as a kid? Hardly ever, right? I asked my partners at Rush. They’re like, I don’t know if I ever see it. I will see people with arthritis downstream because of my practice from it, but it is extraordinarily rare. So, probably too much is being done for this condition. That being said, when they become symptomatic, I think this is a good way to manage it.