Whenever you have ortho tumor folks speaking to you, what you really have are two big opportunities and this is the preachy part of the lecture. The first opportunity is hopefully to help prevent someone dying. This is a hard stop and not hyperbolic. All of us on this panel could probably fill up an entire lecture with “OOPS” surgeries that have resulted in death. The second thing is mitigating the risk of needing to amputate another surgeon’s “OOPS” surgery. This is another hard stop. If we can get in front of people, residents attendings, whomever, and impress upon them those two things then I think that I would be happy.
So, how do we do this? I was tasked with discussing tumors that mimic.: An agreeable definition may be that a mimic or a mimicker is something that gives an impression that is not real; it’s assuming that what you are seeing is benign but it is not. That’s what a real mimicker would be in the world of tumors. I don’t think that this dilemma that we have with mimicking is wrongly assuming something is benign. Mimicking is what we’re supposed to be talking about, but common things are common and rare things are rare. I think that what we have is a problem with just not seeing a tumor!
The reverse total shoulder arthroplasty previously presented wasn’t a case of mimicking. That was a dedifferentiated chondrosarcoma. There wasn’t anything mimicking about it. There was nothing that was abnormal as far as the chondrosarcoma world goes. However, there is something wrong with seeing the x-ray amongst a half day clinic of 40 people. But that’s not the tumor’s fault and that’s not a mimic. That’s just a missed x-ray. Another dilemma may also be sending a patient thought to be benign to a tumor surgeon for whatever reason. Which is also, again, not a mimic.
I think that a real mimicker is amazingly rare. I think that what’s more common is not remembering that tumors exist, which gets us into trouble. What is even more common amongst all of our practices with all of the externalities that are beating down on us, is lamenting the extra time it takes to prove or disprove an innately skeptical hypothesis i.e., a gut feeling that something isn’t right. I can’t tell you the number of times that someone has called (and we do appreciate “OOPS” surgery referrals to be preceded by a call) saying “I knew something wasn’t right, but…” So in my mind what we should be trying to do is to strive for bigger and better “guts.”
I don’t mean that in the negative. It’s the development of listening to your gut. The real mimic dilemma is the occasional misread of a bony lesion by an orthopedic surgeon. Most of us have to read our own x-rays now for a lot of different reasons. It is possible that you misread an x-ray. I think it is amazingly rare that orthopedic surgeons misread x-rays, radiologists call something benign when in fact that it’s not, or radiologists suggest something to be malignant and the surgeon may or may not for whatever reason discredit that read or not read it. Those I think, are opportunities to discuss mimicking but they are again, rare. These are some pearls to stay out of trouble. I think that pearls do last a little bit longer on our minds than a random, crazy looking x-ray. The first thing that I tell every single resident that comes onto service, “resist the urge to name something.” What seven syllables you attach to an x-ray finding means nothing to that finding. Whatever it is, it is. The good Lord knows what it is. The rest of us are just guessing. The moment that we utter something, and heaven forbid, dictate in a chart that that’s what it is, everyone else starts from that point, not from zero. I can’t tell you the number of people that I’ve seen that have been told to have (and the radiologists love this), a fibroxanthoma of bone, which I think in my 21 years of practice, I may have actually seen once. But I swear to you I get six of these a month called by the radiologist. Resist the urge to name something and to prove that point we’ll play a little game with all of the distinguished people in this room. What is the treatment for a Unicameral bone cyst? It’s one of two, observation or curettage. Treatment for a giant cell tumor unless it’s very aggressive stage 3; curettage, bone graft, or watching? Treatment for an ABC; curettage, bone graft, or watching? Treatment for a CMF; curettage, bone graft, or watching? Why in the hell do we have to have this desire to name something when it is the treatment that is the most important?
What’s the treatment for Ewing sarcoma? Referral to a cancer specialist? What’s the treatment for osteosarcoma? Referral to a cancer specialist. What’s the treatment for Dermatofibrosarcoma Protuberans? Referral. Again, given the similarities in treatment why do we care about the name when what we need to be figuring out is “aggressive or not aggressive.” Resist the urge to name something and instead of naming, tell me whether or not you’re worried about it. Because that goes a lot farther than naming something. Trust your gut. Once you pass your boards, who cares about the name? The patient doesn’t. Does what you are looking at make you and your gut feel good, bad, or are you in between? Do you just not know? There is that old adage that says to always trust your gut. Your brain can be fooled. Your heart is an idiot, but your gut doesn’t know how to lie. We should trust it. If you are on the fence, how do you get off the fence, if you see something that you aren’t sure about how do you get off of that?
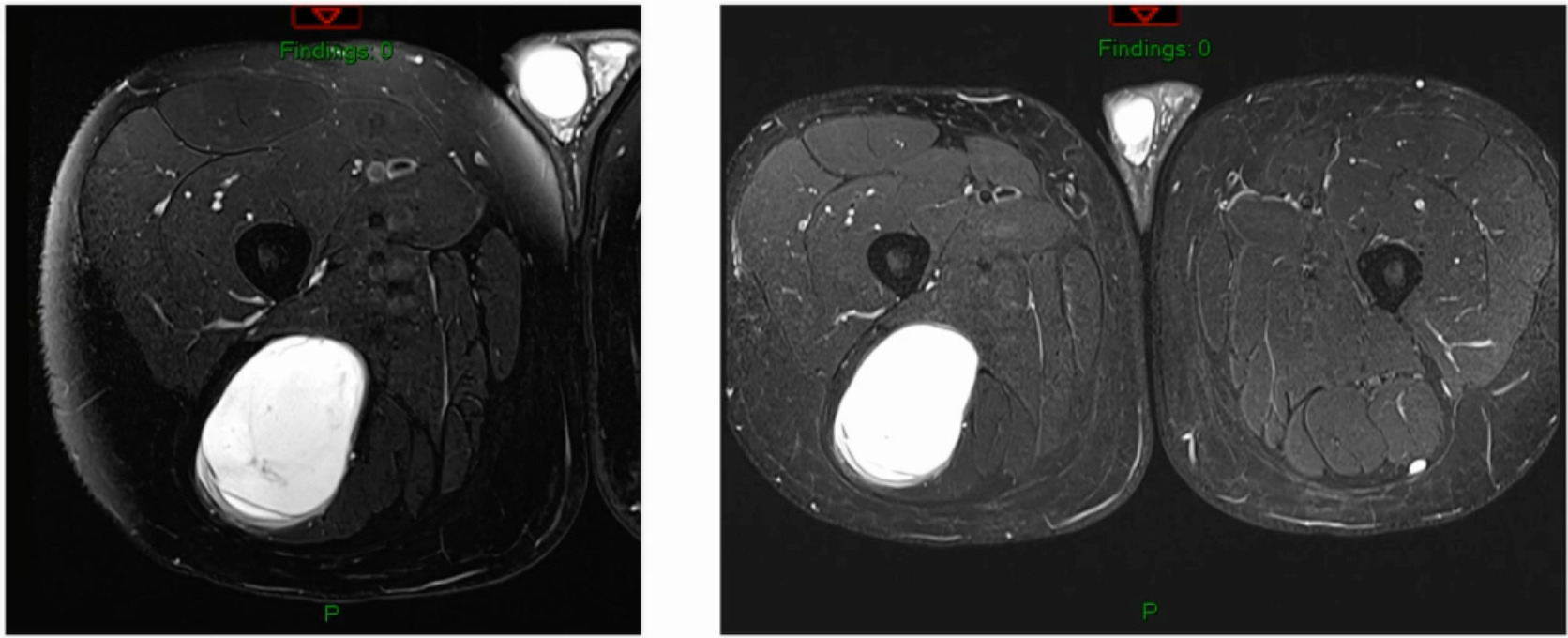
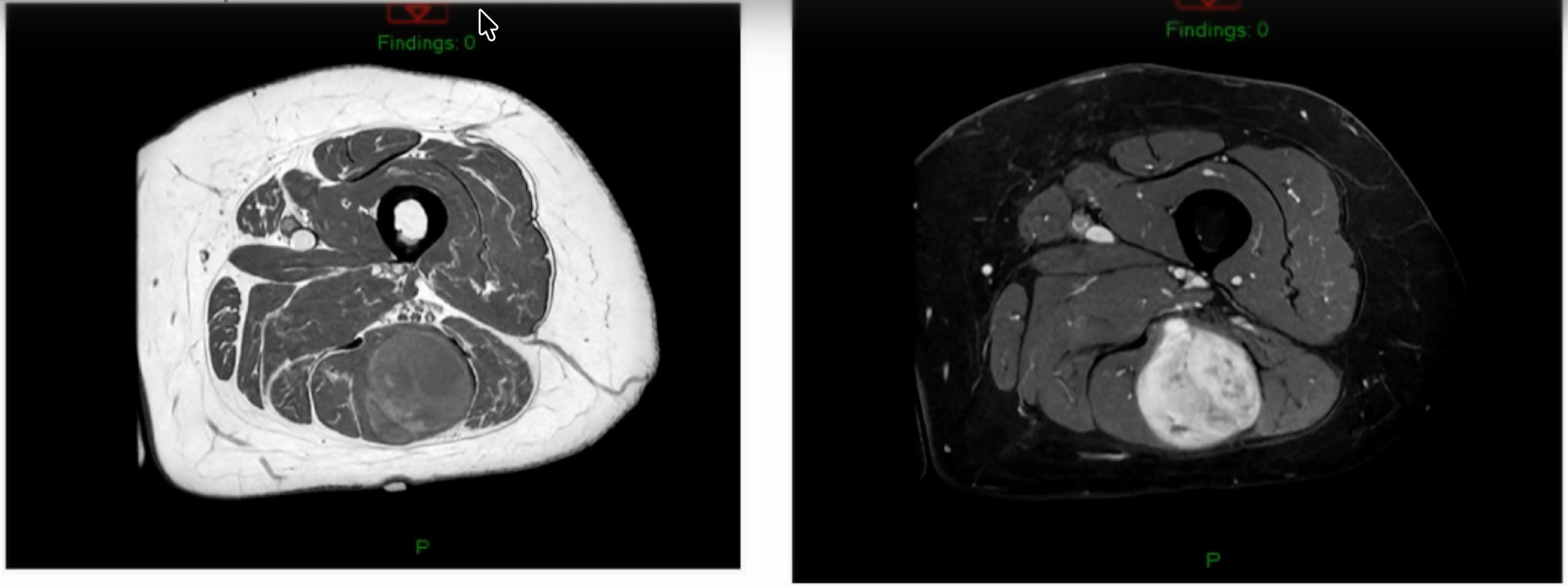
In 2025, the answer to that is an MRI with contrast. Generalists are not going to be ordering a PET scan. Bone scans are, I think, instruments of the devil. CT scans are necessary if somebody has a contraindication to an MRI. But MRI is the absolute “gold standard.” Radiologists will suggest something to be malignant, and we either agree or disagree with it. Now onto some cases. This is the one I think that gets many people into trouble. (Figure 1)
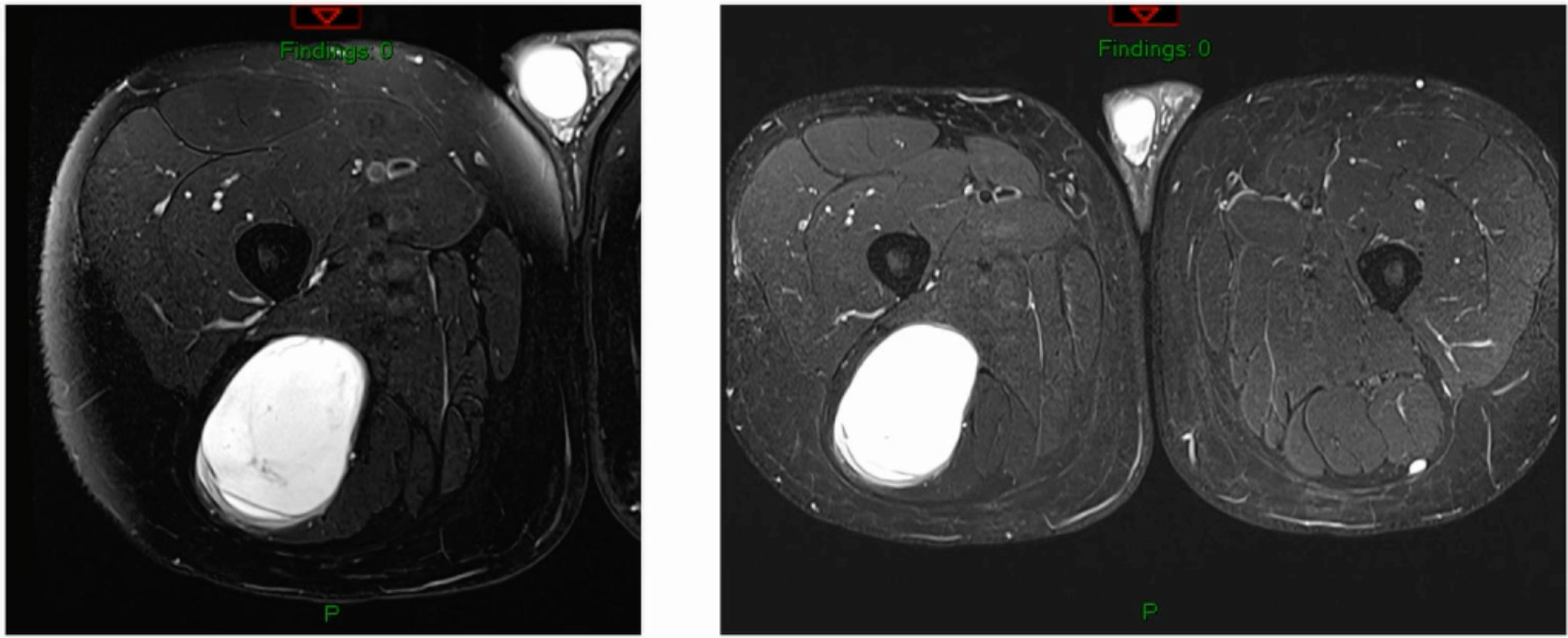
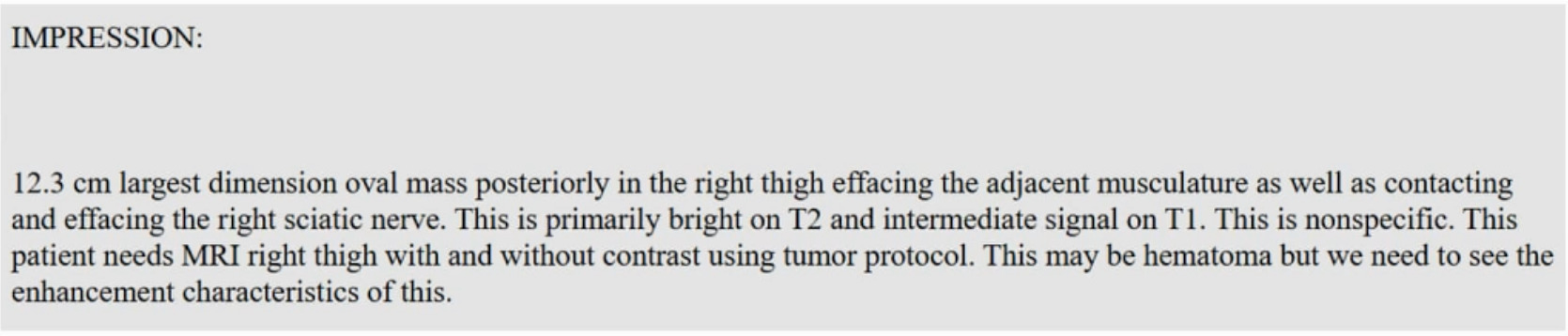
The radiologist report is below. (Figure 2)
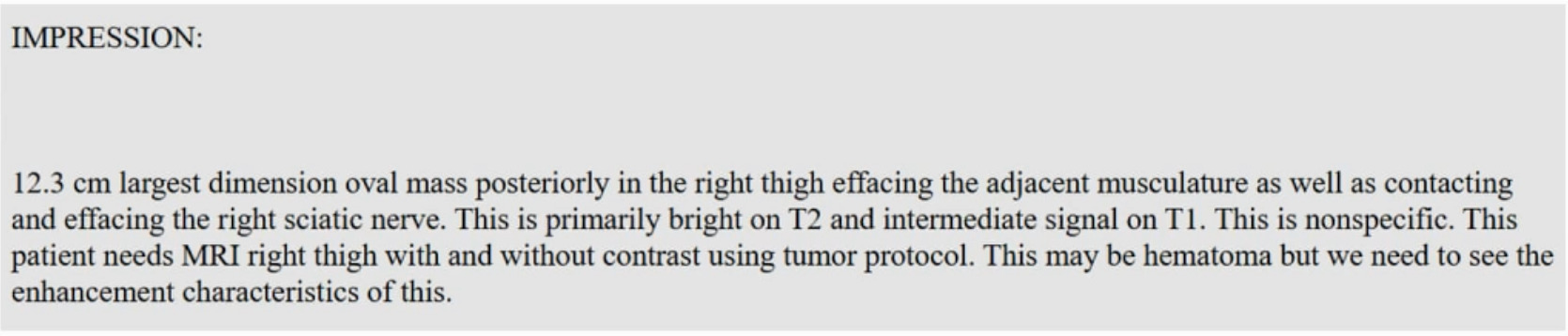
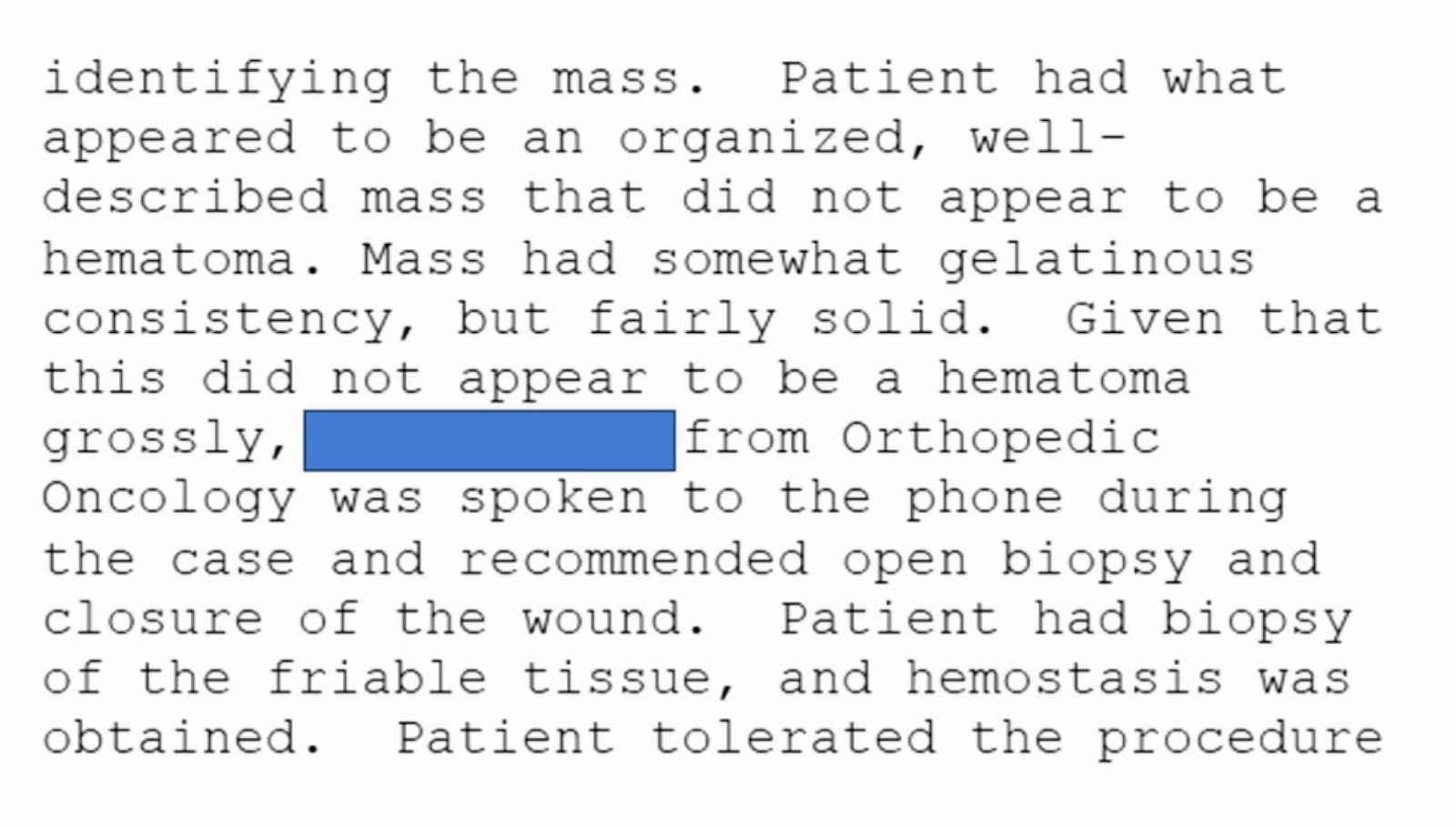
This was done without contrast. The radiologist says you should “do it with contrast.” But the surgeon said, “I’m going to take it to the OR.” Below is the OR note obviously redacted. (Figure 3)
Following studies, it was a malignant peripheral nerve sheath tumor. Was that an “OOPS?” Was that a mimic? A contrast MRI would’ve shown exactly what that was as far as aggressive or not aggressive. It doesn’t tell you it’s a malignant peripheral nerve sheath tumor, but it does suggest aggressive or not aggressive. This is not a mimicker like when aradiologist calls something benign when it’s not. These are the ones that I think get us into a lot of trouble as well. Because many of us are so busy, we don’t read our own imaging. We just order the imaging and then read the report or our physician extender might read the report.
These are a couple of sub pearls: “nothing in an adult should grow!”
Patient: “Doc, I’ve had this lump on my arm.”
Surgeon: “How long has it been there?”
Patient: “It’s probably been there about five months.”Surgeon: “Is it growing?”
Patient: “I think it is.”
If you have the urge to operate on that, lay down until that urge passes. That’s going to get you into trouble.
Patient: “Doc, I’ve had this bump on my arm.”
Surgeon: “How long has it been there?”
Patient: “It’s probably been there four or five years.”
Surgeon: “Is it growing?”
Patient: “I don’t think so. It’s been there four or five years. It doesn’t bother me.”
Do whatever you want to do to that one. But nothing in an adult should grow. If it’s growing it doesn’t need to be in your office. Nothing in adult should grow. Masses deserve an MRI with contrast, obviously there are some times that you can’t get that andthe contrast is the key.
Lipomas are homogeneously bright on T1 imaging. Beyond reasonable doubt you can truly diagnose lipomas based on an MRI. Everything else is always could be X, Y, or Z. Lipomas look like subcutaneous fat on all images including other sequences, but T1 is the one that nails it.
Synovial sarcomas are rarely ever next to a knee. It is a misnomer. Synovial sarcomas are not made of synovium.
Hematomas are rare in young patients, rare in patients that are not on anticoagulation and rare in patients without trauma. It happens, but it’s rare.
Spontaneous abscesses, same thing in the non-diabetic, spontaneous abscesses are rare. When you read these in a report it doesn’t mean that it’s not accurate. It just means that there might need to be a little bit of a pause, and perhaps even a phone call. Because a 30-year-old shouldn’t be getting a spontaneous abscess who is a 30 mile a week runner with peripherally enhancing cysts on MRIs. Now you can have some rare things, and that’s where the mimicking thing may happen. Cysts can be present in a melanoma as an example.. But the point though is all of those are exceedingly rare and exponentially rarer than simply missing a finding.
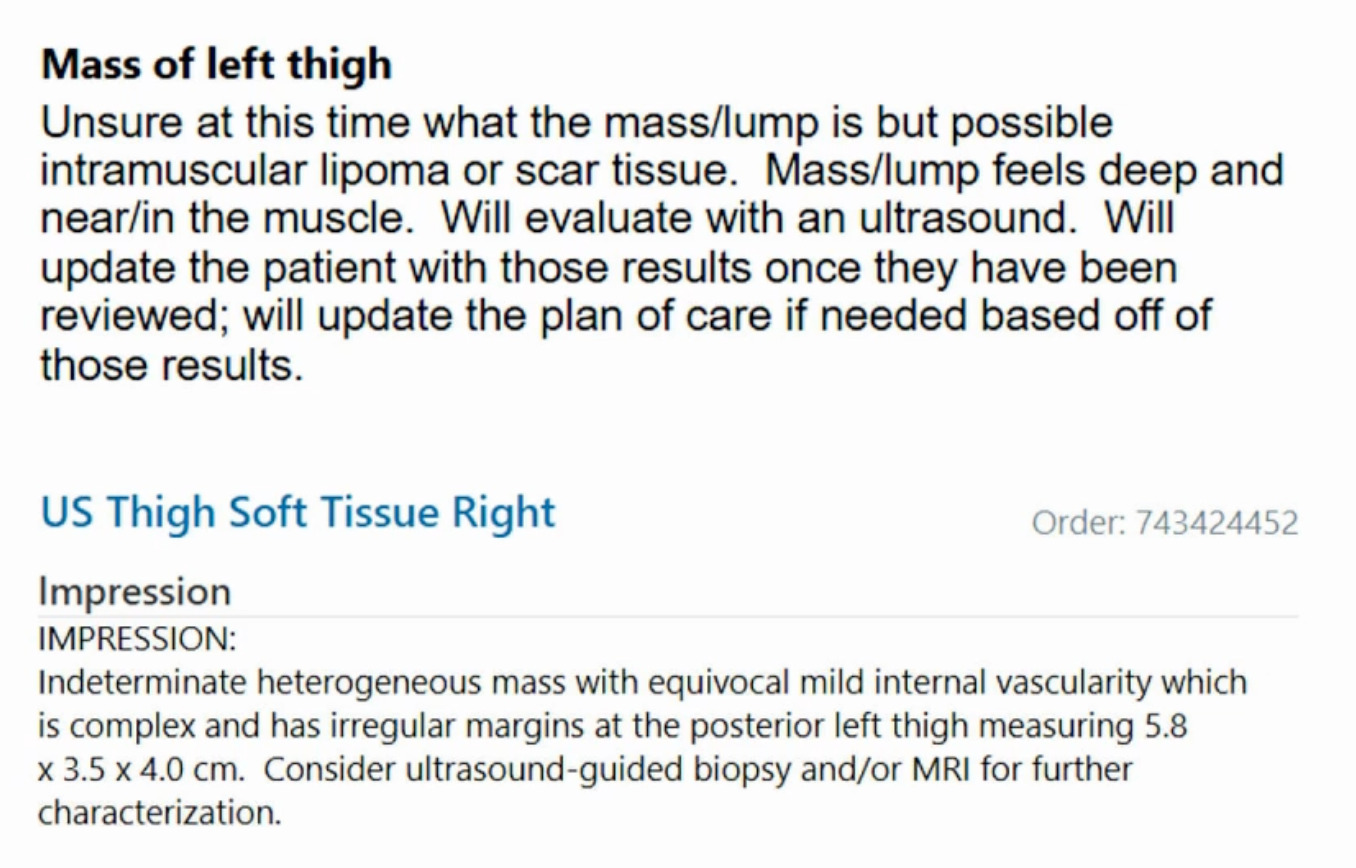
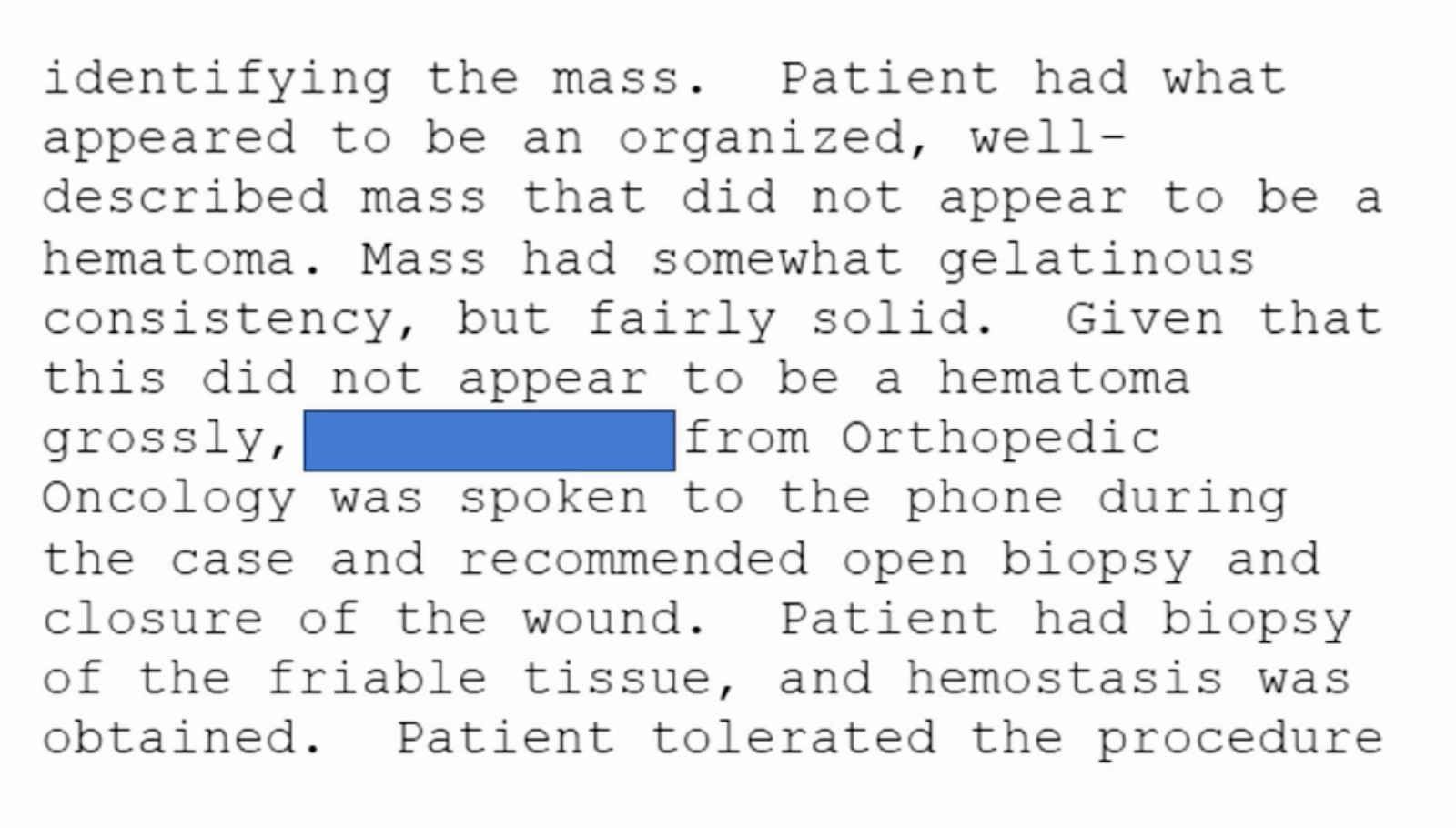
This is a 76-year-old that I just saw this week that had a bump on her thigh annd this is the report (Figure 4).
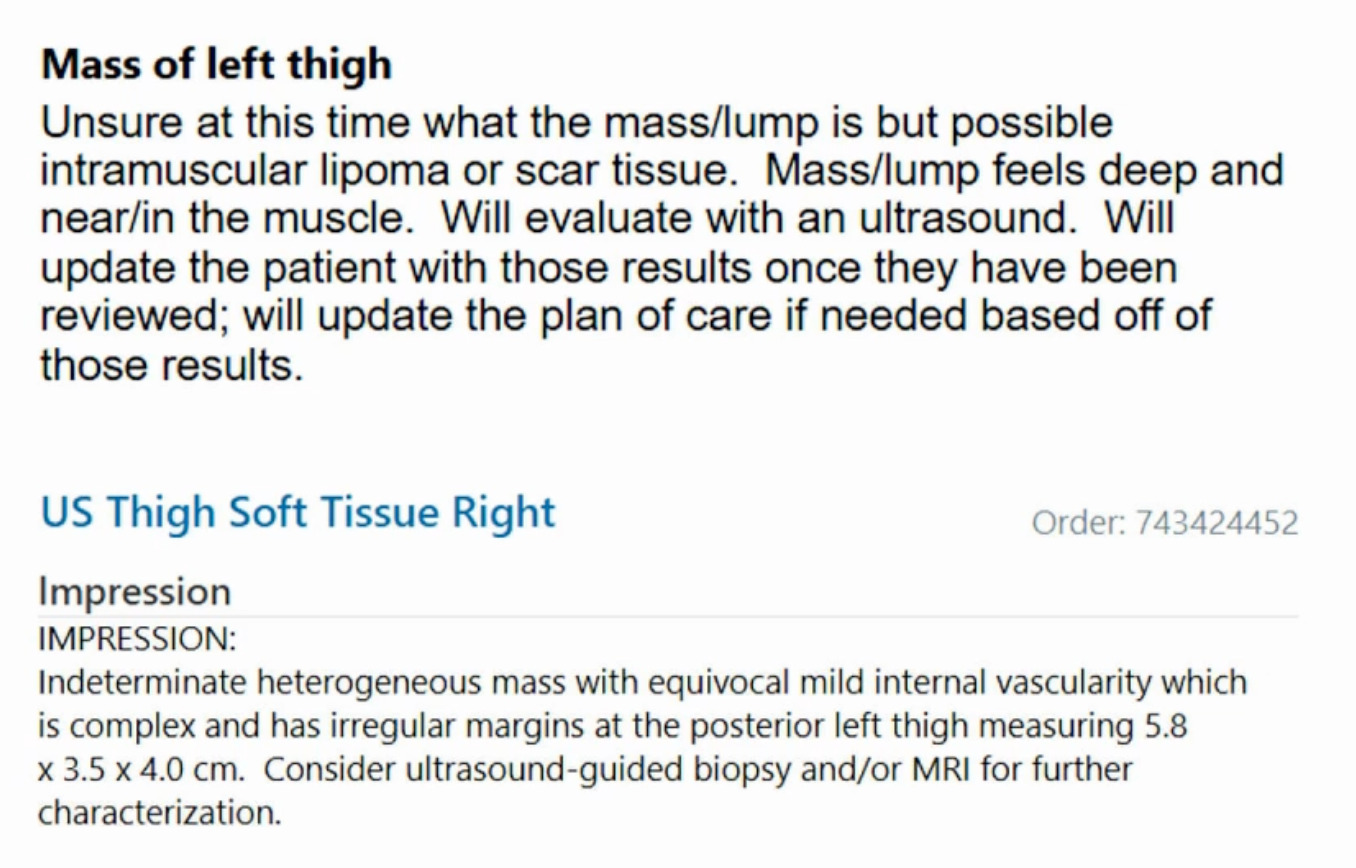
Unsure what it is? Intramuscular lipoma? Intramuscular lipomas aren’t firm and they aren’t hot. Ultrasound for that? The “gold standard” would be an MRI, not an ultrasound, but they did ultrasound it. The ultrasound came back with, “should get an MRI.” But they biopsied it instead. An MRI was then obtained after the biopsy. (Figure 5)
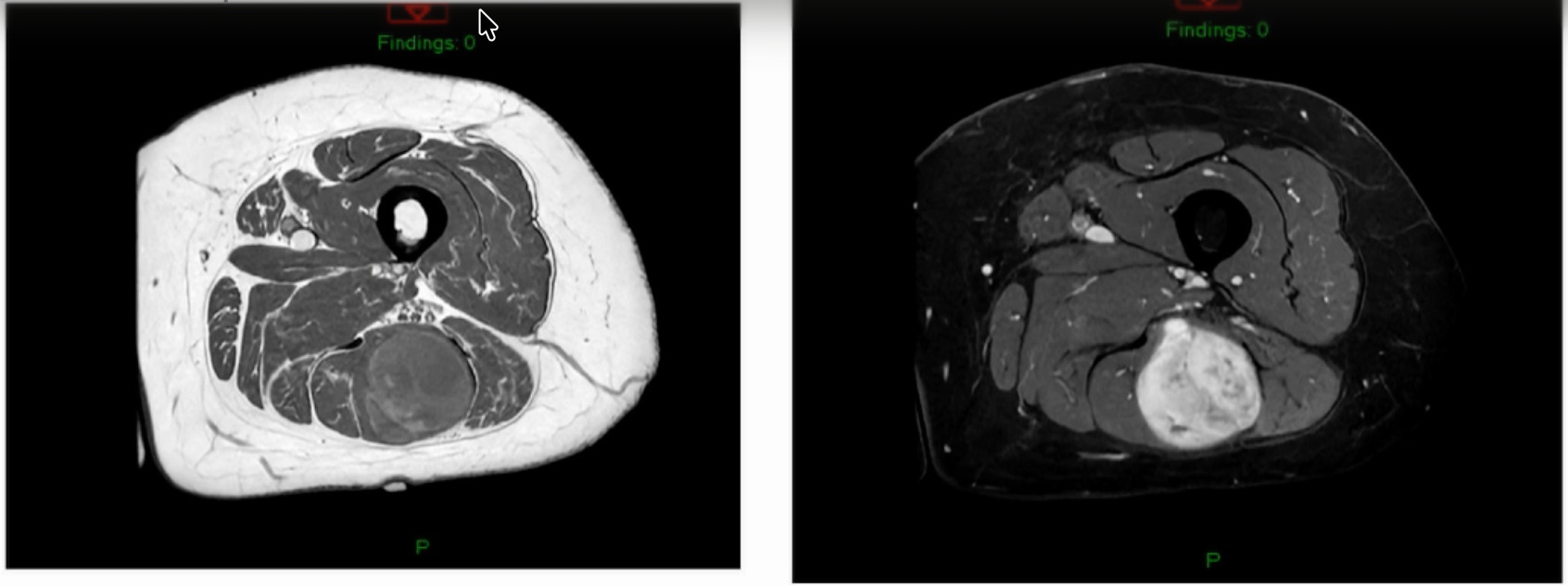
The biopsy came back as a myxoid fibrosarcoma they biopsied it with a needle, so it’s very hard to tell grade. Additionally, if I’ve got a tumor that’s this big and I’ve got a needle the size of a pin then my sampling error is massive. I don’t ever believe grade off of a biopsy. I just get biopsies so that now I can at least give radiation or do whatever pre-operatively. She is starting her radiation next week for a number of reasons. But she’s got a myxoid fibrosarcoma.
In summary I think mimickers are rare. I think that it’s much more interesting and it would be a fun conversation and a fun lecture to talk about MRIs, maybe the entire time because they’re fascinating. Always remember, we’re here to help! Call. Text. Everyone in the upstate of South Carolina and in the Midlands has my mobile number. As for the other panelists, I bet the same thing for Northern Florida and I bet the same thing for Jersey. They have our numbers so text, call, anything including smoke signals, carrier pigeon, whatever it is, I’ll answer it.
Paul Catalana, MD, one of our former deans, had said this 10-years ago and it’s something that has just kept with me ever since,
“What we do in just five minutes can affect what happens to someone for the rest of their lives.”
So, no amputations and let’s not try to kill people.