
Good morning, everybody. So this morning, I’m going to talk a little bit about this emerging reality that John just mentioned in doing revision total hip arthroplasty in the ASC. Kind of an interesting concept.
These are my disclosure. It’s not irrelevant.
Logan Hyatt, he’s a resident here, fourth year, he did do some of the lit search on this, so we’ve got to give him credit. So ever since, you know, getting primaries in the ASC, it’s been a complete game changer. You know, ever since its removal from the inpatient only list, we’ve dramatically increased efficiency. We’ve led to, this has led to better PROMS and outcomes. We’ve taken control of our process. We’ve taken control of our lives, which has led to quality of life, more time with our family. We did this by breaking down the dogma, thinking that primary joints had to be an inpatient procedure and in the hospital for several days and going to rehab and all these things.
So how did we do it? Well, we changed the expectations. We educated our patients and really just changed the culture. Of course, we optimized them. We had better pain protocols, and we got these patients out of bed and we started moving them a lot quicker.
So we’re now confronted with the newest challenge, and that is getting the appropriate revision cases into the ASC. Why do we want to do that? Why do we care? Well, the same reasons that we move the primary joints over there, and really a lot of these revisions that we do are as safe or safer than many of the primaries we do in the ASC.
But importantly, you know, we all know that the revision burden is exploding and is expected by 2060 to double. All right.
And so, of course, this is going to get very, very expensive.
So take a note that ASCs are reimbursed just a fraction of what the hospitals are getting.
So there’s some cost savings opportunities here, which leads us to have to look at the term that we all love to hear, which is value-based care.
So let’s hear what Michael Porter, Harvard Economist, has to say. [video] “Have we thought about our health systems in a way that’s aligned with value? Do we have the right service in the right location?”
So do we have the right service in the right location? So take an example of what ASCs are doing for government health care spending. In 2008 through 11, they saved Medicare, $7 .5 billion, and then since then, well over $60 billion, so there’s, again, a lot of cost -savings opportunities here.
But is it safe to move revision cases to the ASC?
The answer is absolutely yes. In the appropriate patients, there’s multiple studies out of great institutions like Indiana, Duke, Rothman, And joint implant surgeons, of course, Lombardi and his team published on this. But in the appropriately selected patients, complications are the same or better, and patients are just as happy.
But what about our value? I brought up this example last year. I think this is also an important consideration, and I use the example that I can do six primary hips in the ASC in the same time it takes me to do a full hip revision in the hospital. But these, unfortunately, are not equal for our time and effort.
So at this most simplistic form, it’s a difference in the RVUs. So 120 versus 30 RVUs, that’s four times more valuable to do that time in the ASC for those cases. Now, when you take into account potential surgery center ownership, and the fact that these revision cases can provide us a headache for the rest of our lives, you could double that even further.
So this really doesn’t make any sense. So at the very least, bringing some of these revisions to the ASC will maximize efficiency and give us a little bit more time, you know, outside of the hospital. And if you have ownership in the ASC, of course, that helps as well.
So in order to understand where we’re at with this process, we need to understand where we’re at with CMS, because we’re still kind of trying to get through this conundrum with CMS before we’re going full -time on the outpatient revision spectrum.
And so let’s just talk a little about the history of where we were, and we call this the dark ages prior to the 2018 year. And the reason why is everything was on the inpatient only list, primaries and revisions, And at this point, CMS had relied on some existing evidence, basically saying that basically any arthroplasty was just needed an extended stay. It was more invasive. It had complications and a big recovery.
Fortunately, cooler mines prevailed, and in 2018, they did finally remove knees from the inpatient only list, and shortly thereafter added it to the ASC cover Procedures list so that we could start getting paid by CMS doing these in the ASC, and hips followed very shortly behind.
And in 2021, they actually went ahead and removed revisions from the inpatient only list. And there was no addition to the ASC covered procedures list, so we couldn’t readily start doing them with CMS patients. But the goal of this was to restore surgeons’ autonomy and allow us to decide what the appropriate location was going to be.
And they actually wrote this statement, which is shocking to see from a government health care agency. “But the physician should determine whether a particular beneficiary would be a good candidate to undergo a procedure in the ASC setting rather than the hospital setting based on the clinical assessment of the patient.” So they are actually delegating that to us to make the decision, which is quite wild.
Unfortunately, in 2022, after there was some pushback, including our own academy, they decided to reverse this inpatient only elimination. So we are currently still on the inpatient only list for revision joints.
So this is not fun.
All right, but you may have received this email from AAHKS recently. This is a summary of the major changes for the 2026 Medicare, OPPS, and ASC payment policy. The goal here is to drive more procedures to the outpatient setting, and I’ll highlight a couple of things here. You can see in the middle, the inpatient only list will be phased out over the next three years, and that includes all 27000 codes, which includes revision arthroplasty, and also proposing a reimbursement level for revisions as well as hip conversions.
And to go ahead and add these then to the ASC cover procedures list so that we can begin getting paid for them.
Okay, so we’re heading in that direction, but doesn’t make any financial sense to bring revisions to the ASC.
The way the ASCs get paid is A couple of factors, but they use a hospital wage index. They add in an ambulatory payment classification system, and they do an ASC conversion. So it’s kind of a couple of set numbers to get you that ASC payment.
The problem is that the implant is included with Medicare patients in that facility fee. So as the implant cost rises, of course, your bottom line is going to shrink. And, of course, revision procedures can be quite resource intensive, and these implants can vary quite a bit depending on the complexity of the case. So we need better solutions if we’re, in reality, going to be bringing a wide amount of these revisions to the ASC setting.
So there’s some potential solutions. You know, none of these are in stone yet, but you could do what’s called a tiered implant plus model where this is essentially stratified. It just varies the implant inclusive bundle depending on the case complexity. So if it’s a poly exchange versus a single component versus a two component, you can have different tiered models for the payer. And this gives them predictability, but recognizes that not all revision cases are equal. There’s also an implant cost carve -out threshold. And then, of course, the revision exclusion, so cost plus models. This is typically what they have in the hospital setting. So this would be preferred.
And the way that would work, of course, is you just add that implant cost in addition to what we discussed before, and this would be covered by the insurance. And, of course, you just try to get some maybe more favorable implant provider contracts.
Unfortunately, there’s just not a lot of precedent with this care of patients, but with this 2026 proposal, this may be changing with this new precedent. They’re suggesting unpacking things like skin substitute products and proposing APCs based on specific product factors. So this may be a way in for revision implants.
Another loophole, I guess, here is this device intensive option. So this exists now, but just not really seen with joints. And this basically says that “if the implant cost is greater than half of the bill, that they can separate the cost and just do an ambulatory payment classification conversion factor on the remainder of the visit.” And so this helps get you some of that implant cost back.
Okay, so we’re heading in that direction. We’re eventually going to hopefully have some solutions there on how to get Medicare patients paid in the ASC for these cases. So how do we do it safely? How do we recreate the magic that we’ve seen with our primary joints? So we’re going to use a lot of the same ingredients that we use with primary joints. We’re going to add a couple of new flavors.
But what are the appropriate indications for doing revisions in the ASC? So we like to think, of course, about the patient, okay? And not just their medical comorbidities, but also their functionality, social factors (do they have good home support, do they have a good living situation), of course we talked about payor contracts, surgeon comfort (of course you wany to be proficient in doing revision surgery, I’m certain everybody in here fits that bill), and surgical factors (we want to consider the acuity of the these cases, these surgeries), and of course the complexity.
So in terms of our optimization protocol, we haven’t really changed much other than we put a hard cut off at 80 years old and we raised the hemoglobin criteria a little bit. BMI is now 35. We feel maybe if you’re using anything more than a single prong cane, you probably want to go to the hospital and then dental clearance for all these patients.
Contraindications, the hard contraindications have remained the same as seen for our primaries.
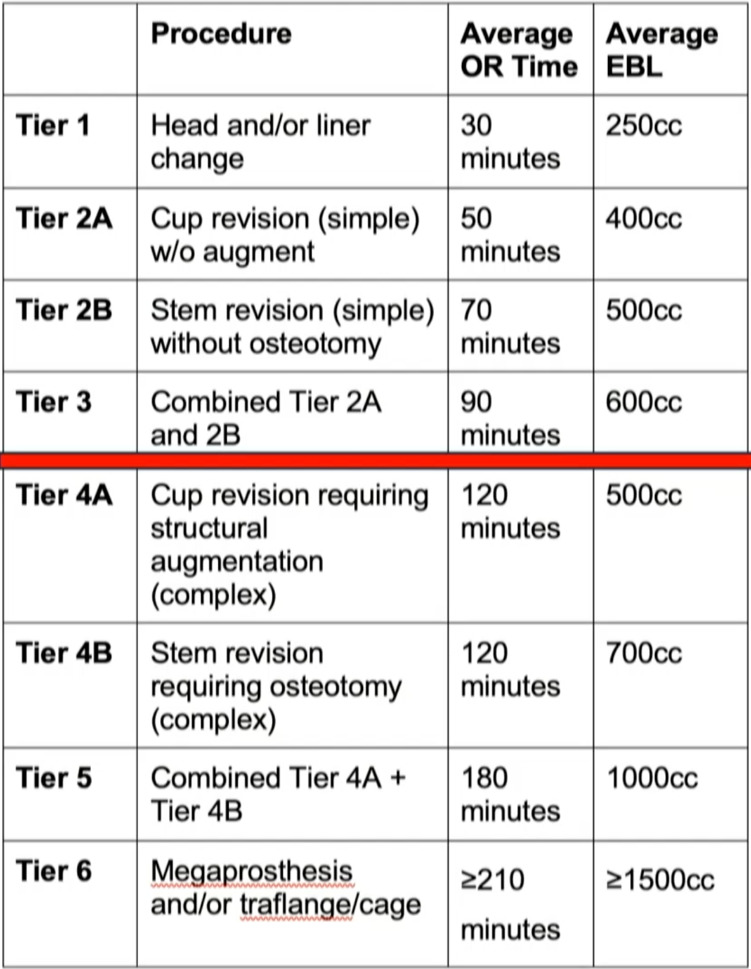
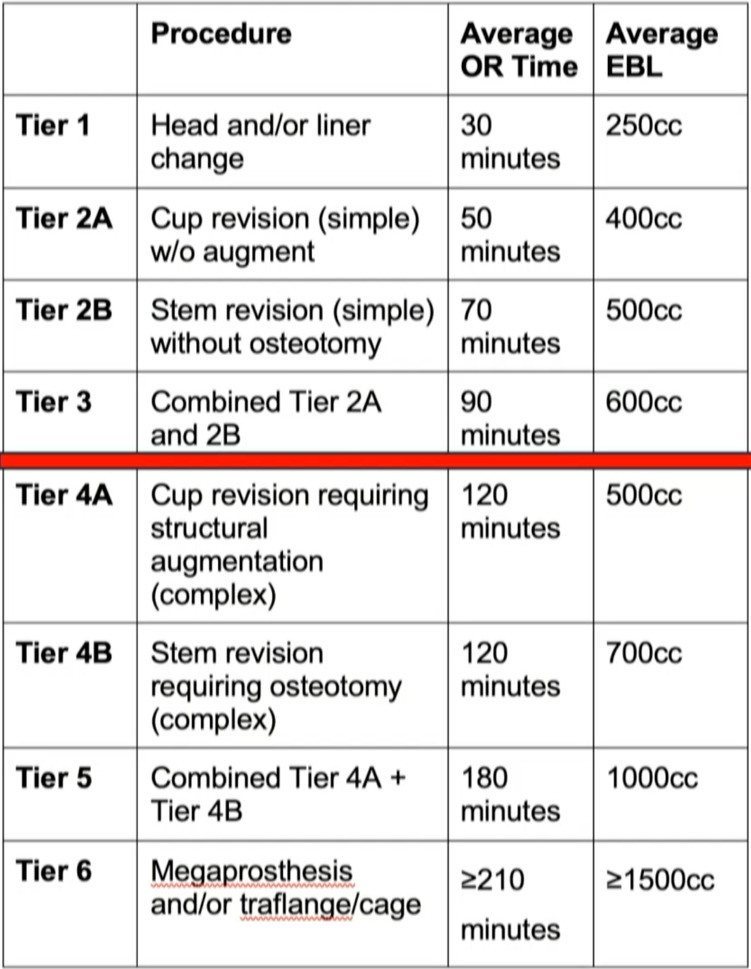
And so what are the right surgeries that we can take to the ASC? So revision arthroplasty is kind of a nebulous term. It’s really a spectrum of different procedures all the way from modular component exchanges up to these megaprostheses. So we’d like to think that we can draw a line in the sand and say, okay, these cases, aren’t going to be ideal for the ASC setting, but maybe we have a lot of opportunities over in this area.
So we put together this rudimentary, tiered classification system with some arbitrary numbers with OR time, EBL, Kind of drew a line here, basically saying “we can do a simple two -component revision in the ASC, but anything beyond that requiring, you know, augmentation or osteotomy is probably best served for the hospital,” at least currently. (Figure 1)
All right, so we’ve decided that we’re going to move forward with the case in the ASC. How do we do it? We need to go ahead, of course, and prepare. And scheduling can be the hard part because, you know, we’re having to coordinate a lot of these instruments and implants that we may not already have in the AAC. Of course, we need to optimize our patients. Education and planning is important because, you know, again, the post -op recovery may be different from that of our primaries, so we need to be able to communicate that.
So then comes the big day. They come in for their surgery. I think the big point I want to make here is that just because we’re going to be doing revisions in the ASE doesn’t mean we want to lose sight of our efficiency. So while we’re not going to do 12 -by -12, you know, hip revisions in the ASC, we still should be looking at, you know, our radical time transparency and continuing that operational excellence. We do have tier-dependent spinal blocks. So, of course, if it’s going to be a more complex procedure, longer spinal, maybe using cell saver intra -op for blood management, and, communicating and PACU the nurses and to the providers that, you know, what’s going to be different in this case versus our routine primary cases.
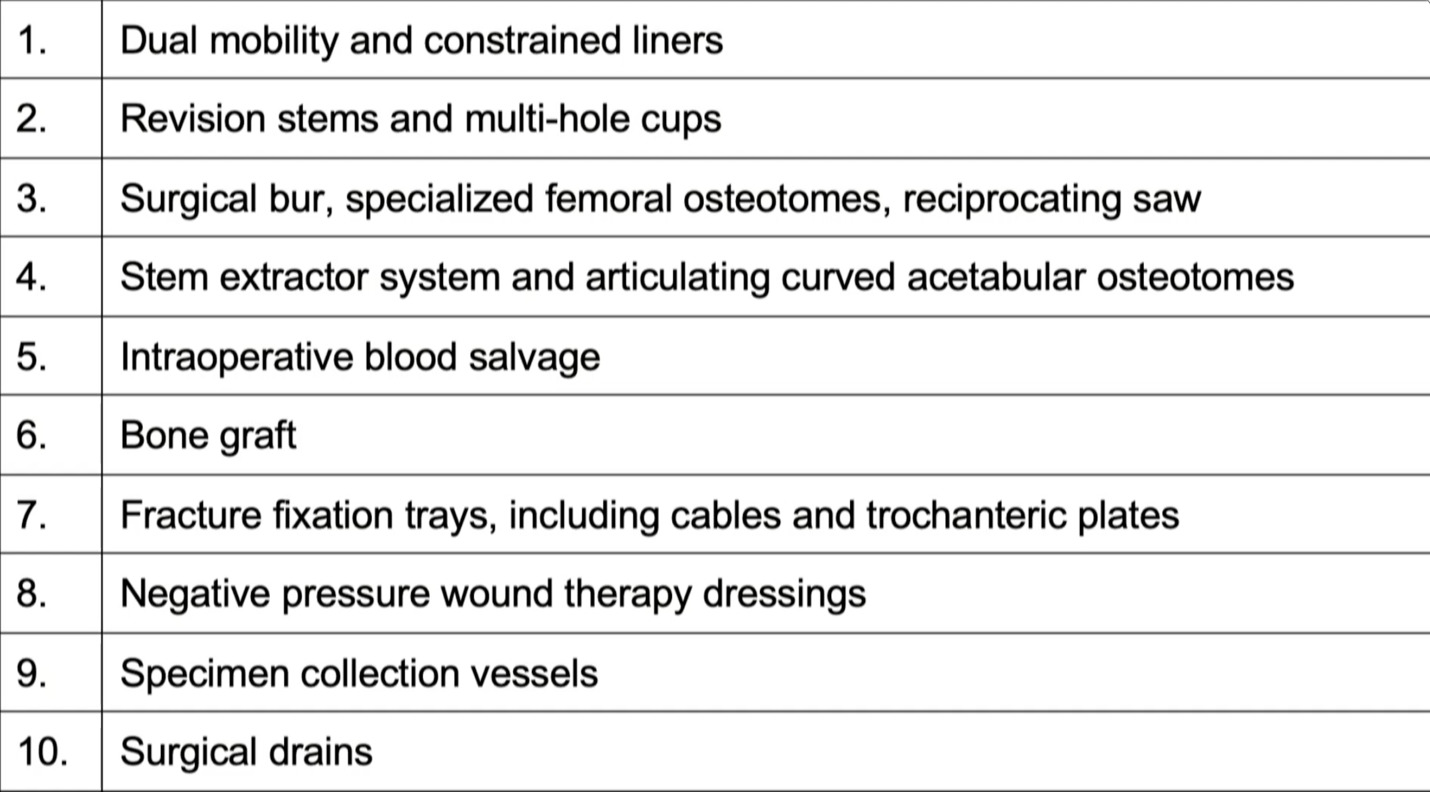
This is just a short list of things, of course, you want to probably have in the OR or in your ASC. (Figure 2)
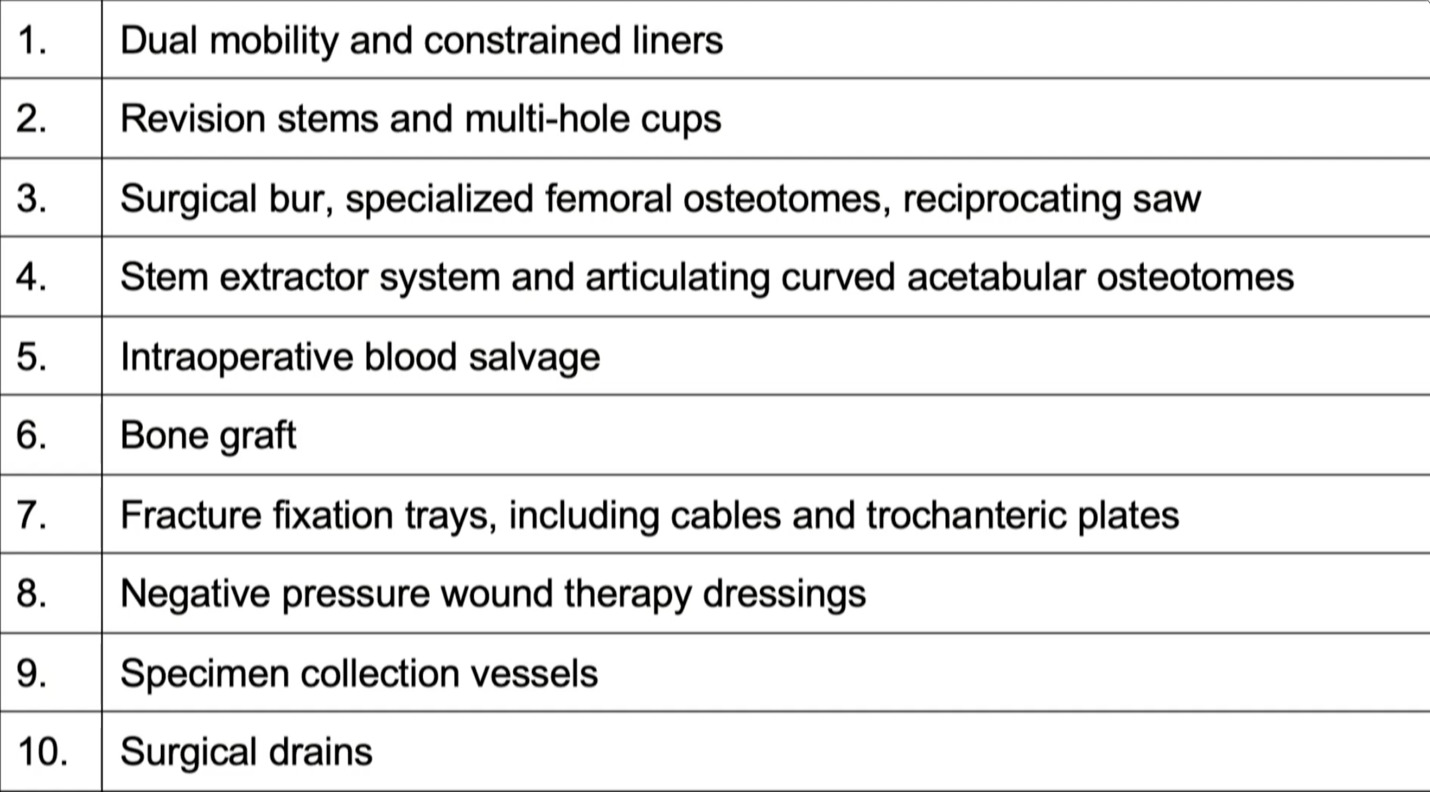
Of course, we have limited space in the ASC settings, so consignment or simply just bringing stuff in the day of surgery is often helpful, making sure that you have backups, but things like, of course, the revision components, extraction devices, bone graft, special wound dressings, you name it, just, you know, you can’t bring the kitchen sink every time, but you need to bring the essentials.
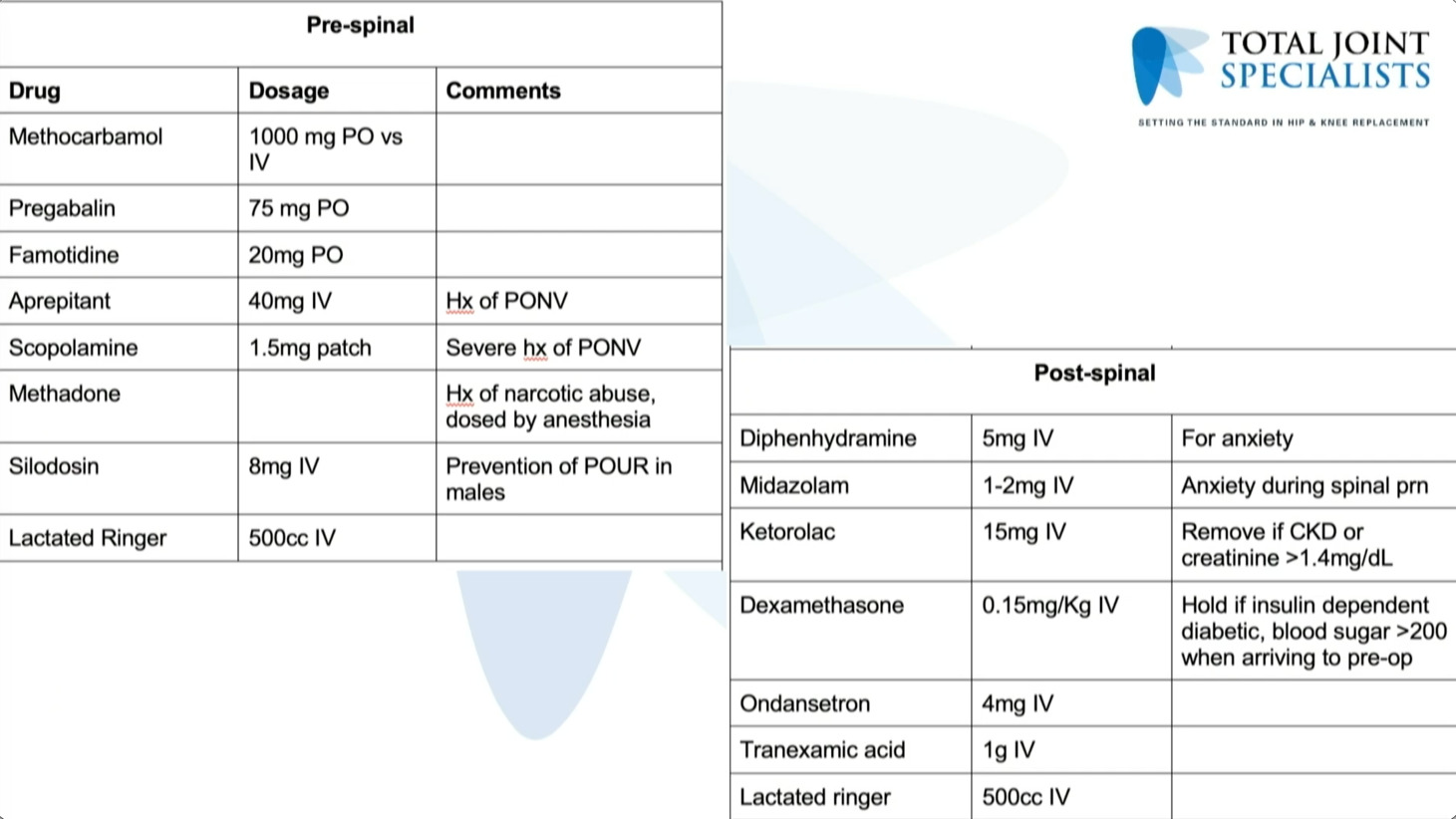
So pre -spinal, post -spinal, this is just our current protocol. This is really no different from our primaries. (Figure 3)
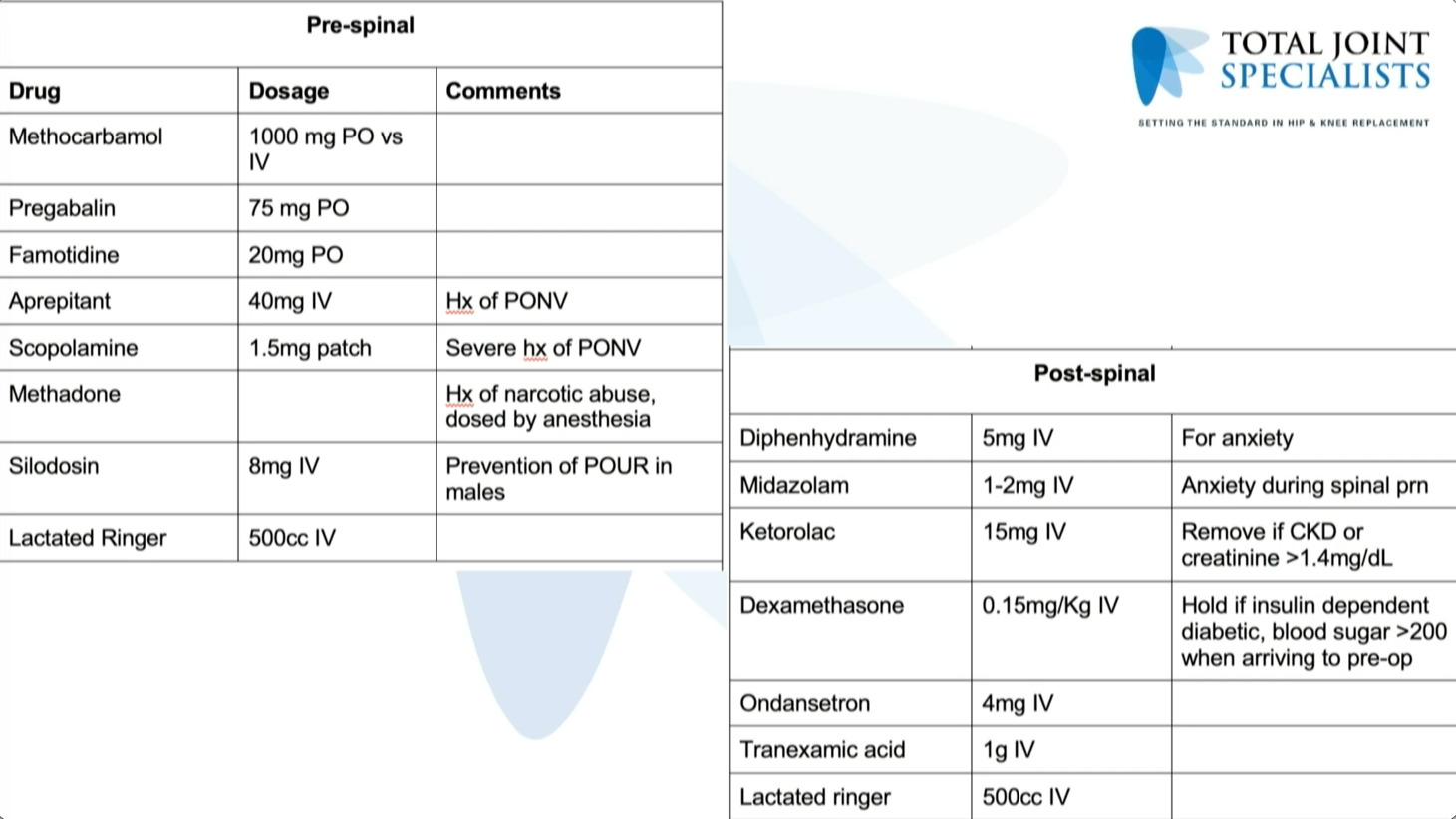
And Same thing with the discharge medications, however we did recently, start doing extended antibiotics for a week and also steroids.
So common pitfalls, these, again, are the same as you’d see with the primaries in terms of these discharge delays, urinary retention, nausea, vomiting, hypotension, pain, over sedation.
So the big thing here, again, is just had that planned place, continue to evolve your protocol over time so that we can continue to minimize these issues in terms of discharge delays, but really we haven’t seen too much different, too much of a difference with revisions versus primaries on this.
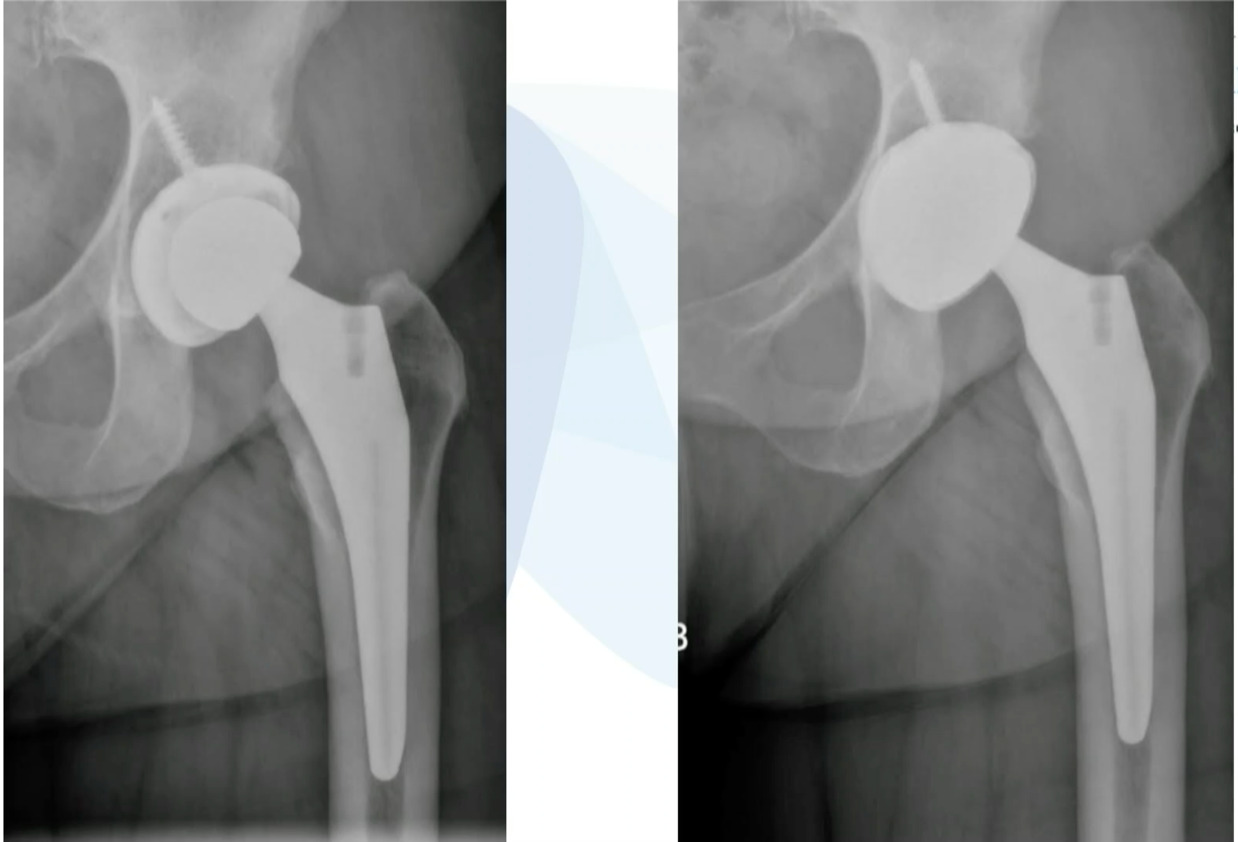
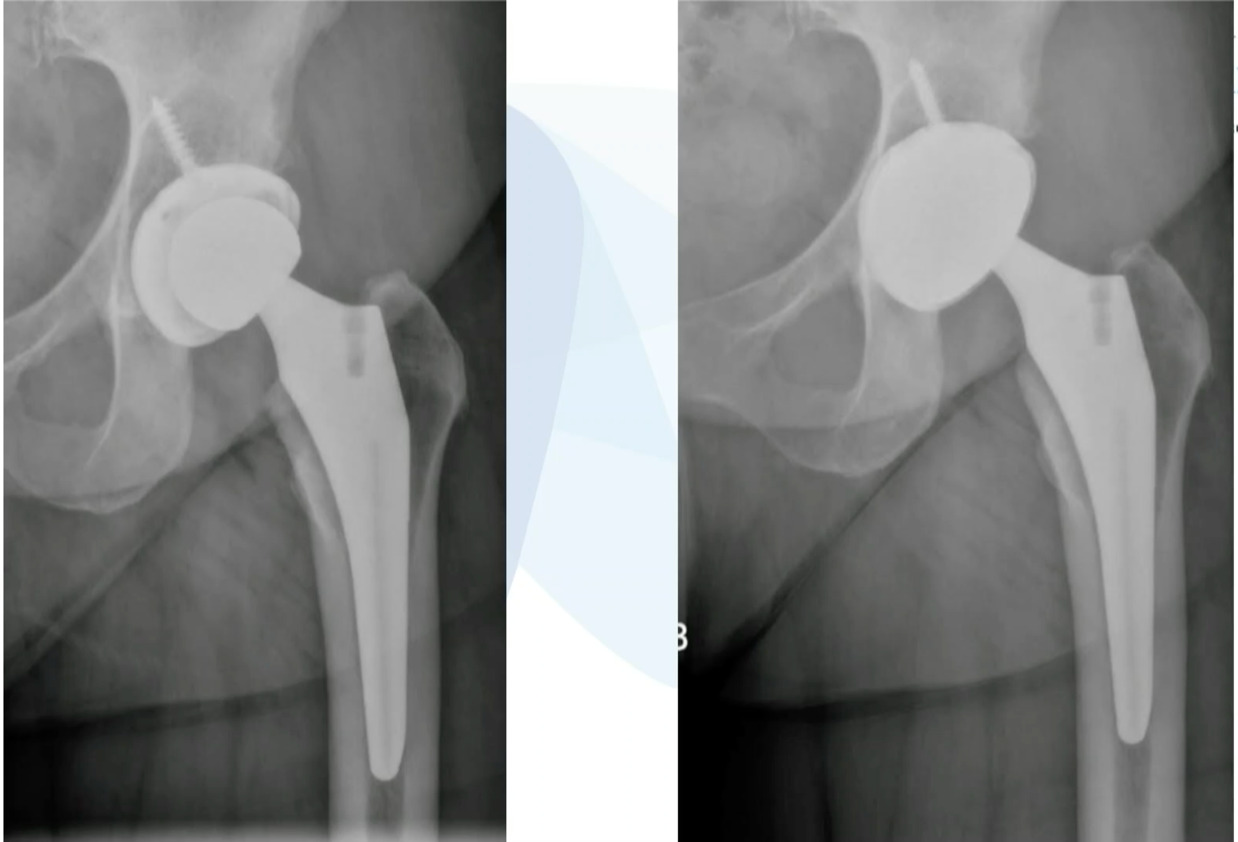
It’s just a couple quick cases that I feel are pretty ideal for the ASC. This is just a loose femoral stem here went in and actually revise this with a modern triple tapered stem. (Figure 4)

We’ve done this on quite a few cases and this is working really well, but you don’t have to use a primary stem, you can use a revision stem. But these loose components are ideal for the ASC setting. This was an ileus-psoas impingement. (Figure 5)
Cup was revised. This is an excellent case to do in the ASC setting.
[Video] “If today you’ve improved outcomes without escalating any cost, you’ve succeeded today. If you’ve delivered equally good outcomes, more efficiently, you’ve succeeded today. If you didn’t do one of those two things, you failed today.”
So let’s not fail today.
So in conclusion, develop your perioperative strategy, you know, pre -operative planning, as with primaries, it’s paramount. Practice these outpatient divisions in the hospital first and begin with easier cases and hopefully soon we’ll have some of these ASC contracts.