INTRODUCTION
Health literacy has been an increasing topic of discussion in the orthopaedic literature (Cosic, Kimmel, and Edwards 2017; Lans, Bales, Borkhetaria, et al. 2023; Lans et al. 2023; Lans and Schwab 2023; Mertz, Eppler, Shah, et al. 2022; Narayanan et al. 2021; Tarabochia, Menendez, and Ring 2021). While definitions can have many iterations, our preferred description of health literacy refers to the degree to which a patient can obtain, process, and understand information regarding their overall health, healthcare conditions, and treatment options (Baker 2006). Individual patient health literacy can vary across different aspects of medicine, as baseline comprehension between topics fluctuates (U.S. Department of Health and Human Services 2000). Specifically, general health literacy may not accurately reflect orthopaedic-specific health literacy. Rosenbaum et al (Rosenbaum, Pauze, Pauze, et al. 2015). were the first to demonstrate this distinction using the validated Literacy in Musculoskeletal Problems (LiMP) questionnaire, which revealed significantly lower orthopaedic knowledge compared with general health literacy among their study participants.
Lower health literacy has been associated with worse clinical outcomes in a number of medical specialties, and orthopaedic surgery is no different (Wright, Edwards, Goggins, et al. 2018; Theiss, Wood, McLeod, et al. 2022; Dumitra, Ganescu, Hu, et al. 2021). Narayanan et al (Narayanan et al. 2021). assessed 450 patients undergoing total knee arthroplasty using the LiMP questionnaire and found that lower health literacy was associated with worse overall satisfaction after surgery. Similarly, Lans et al (Lans and Schwab 2023). evaluated 318 patients with back pain and found that poor health literacy was linked to lower baseline patient-reported outcome measures (PROMs) at the time of their initial visit to a spine clinic. Strahl et al (Strahl, Bücker, Bechler, et al. 2024). reported that higher health literacy was positively correlated with increased satisfaction 1 month after total hip arthroplasty. Recently, health literacy has been studied in the context of shoulder arthroplasty and was shown to be associated with differences in preoperative pain and function as well as perioperative hospital length of stay (Puzzitiello, Colliton, Swanson, et al. 2022).
The large number of new studies being published in orthopaedic surgery literature on the relationship between health literacy and outcomes has driven the need for system-specific validated scoring systems to accurately evaluate the broad spectrum of orthopaedic patients (Lans et al. 2023). This work aims to be the first to describe a validated, shoulder-specific health literacy assessment the “Campbell Assessment of Shoulder Education” (CASE) score. In addition, we aimed to evaluate patients undergoing shoulder arthroplasty and how varying health literacy affects outcomes postoperatively. Our hypothesis was that lower baseline health literacy would result in inferior patient-reported outcomes and worse postoperative range of motion after shoulder arthroplasty.
MATERIALS AND METHODS
Validation of the CASE Questionnaire with LiMP
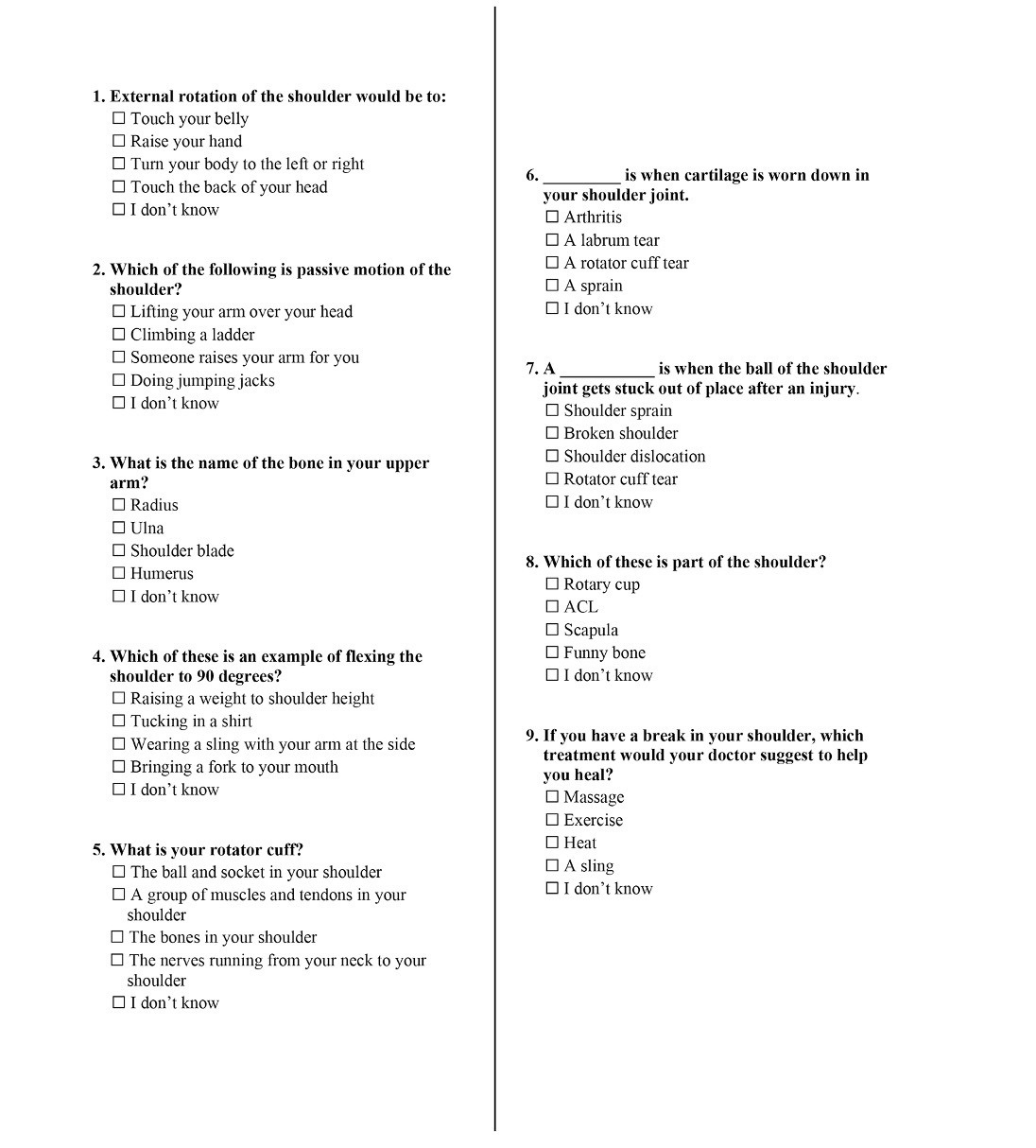
As also described in our sister study evaluating health literacy and outcomes of rotator cuff repair, we first sought to validate CASE against a previously accepted and validated assessment of musculoskeletal health literacy, the LiMP score. Our shoulder-specific health literacy assessment instrument was developed collaboratively by the board-certified sports medicine and shoulder/elbow trained orthopaedic surgeons authoring this study using the LiMP assessment tool as a guide in terms of presentation of questions and length of assessment. The created instrument, called CASE, is presented in Figure 1. The final version of the CASE questionnaire included nine multiple-choice, single-answer questions written at the 3.6 Grade Level per Flesch-Kincaid readability score. After approval from the Institutional Review Board of the University of Tennessee Health Science Center (IRB #20-07870-XP), patients presenting to an outpatient shoulder clinic were enrolled in the study and completed both the LiMP and CASE assessments, either by mail or in-person, after providing informed consent. The inclusion criteria for this portion of the study were adult patients (age > 18) presenting with shoulder pathology. Patients whose primary language was not English, as well as those presenting with acute shoulder trauma, were excluded. The scores from both instruments were compared to validate the CASE test as an effective tool for assessing shoulder health literacy, with LiMP and CASE scores analyzed using a contingency table, sensitivity and specificity analyses, and Spearman correlation coefficients.
.jpeg)
Shoulder Arthroplasty Outcomes and Health Literacy
Patients who were not included in the CASE validation cohort who were scheduled to undergo primary anatomic or reverse total shoulder arthroplasty were then voluntarily enrolled into the second stage of the study. A preliminary power analysis was conducted to determine sample size based on the minimally important clinical difference in forward elevation postoperatively. Patients were excluded from participating if undergoing revision arthroplasty or arthroplasty for proximal humeral fracture. Both the CASE and LiMP assessments were administered to patients by mail 3 months after shoulder arthroplasty. All patients participated in the institute’s standard physical therapy and rehabilitation protocols for TSA and RSA respectively. These results were then correlated with patient demographics, as well as patient-reported outcome measures including pre- and postoperative American Shoulder Elbow and Elbow Surgeons (ASES) , visual analogue scale (VAS), single assessment numeric evaluation (SANE) scores, and range of motion.
After each patient completed the CASE assessment, they were placed into either a ‘high literacy’ or ‘low literacy’ category based on their score being 5 or higher, or 4 and lower, respectively. Scores of 4 and 5 were chosen based on measures of central tendency for the data set and distribution of scores for CASE and LiMP. Fisher’s exact test was used to assess for significant differences in patient demographics (e.g., gender, race, education, healthcare experience, complications, operating surgeon) comparing the high and low literacy groups. Student’s t-test was used to assess for differences inpatient age, and continuous outcome measurements (ASES, SANE, VAS, and range-of-motion measurements [ROM], forward elevation, external rotation in adduction, and internal rotation behind the back) acquired preoperatively, at 3 months postoperatively, and the difference between 3 months and preoperative according to literacy group. The latter delta metric was also analyzed using a nonparametric median test. Continuous outcomes (ASES, SANE, VAS, ROM) were further analyzed adjusting for significant demographic and joint history using general linear model analyses. P-values < 5% (0.05) were considered statistically significant.
RESULTS
CASE Validation
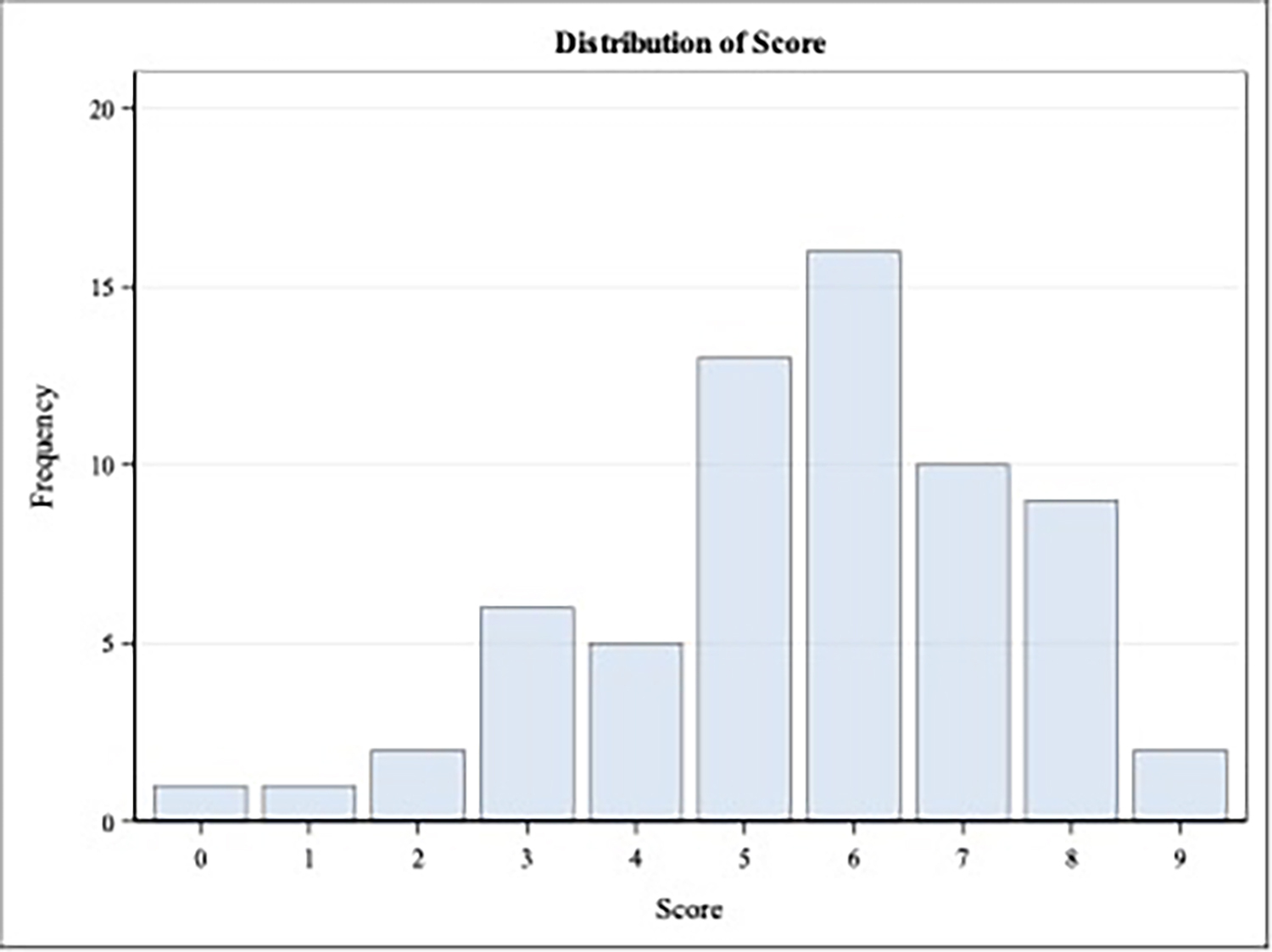
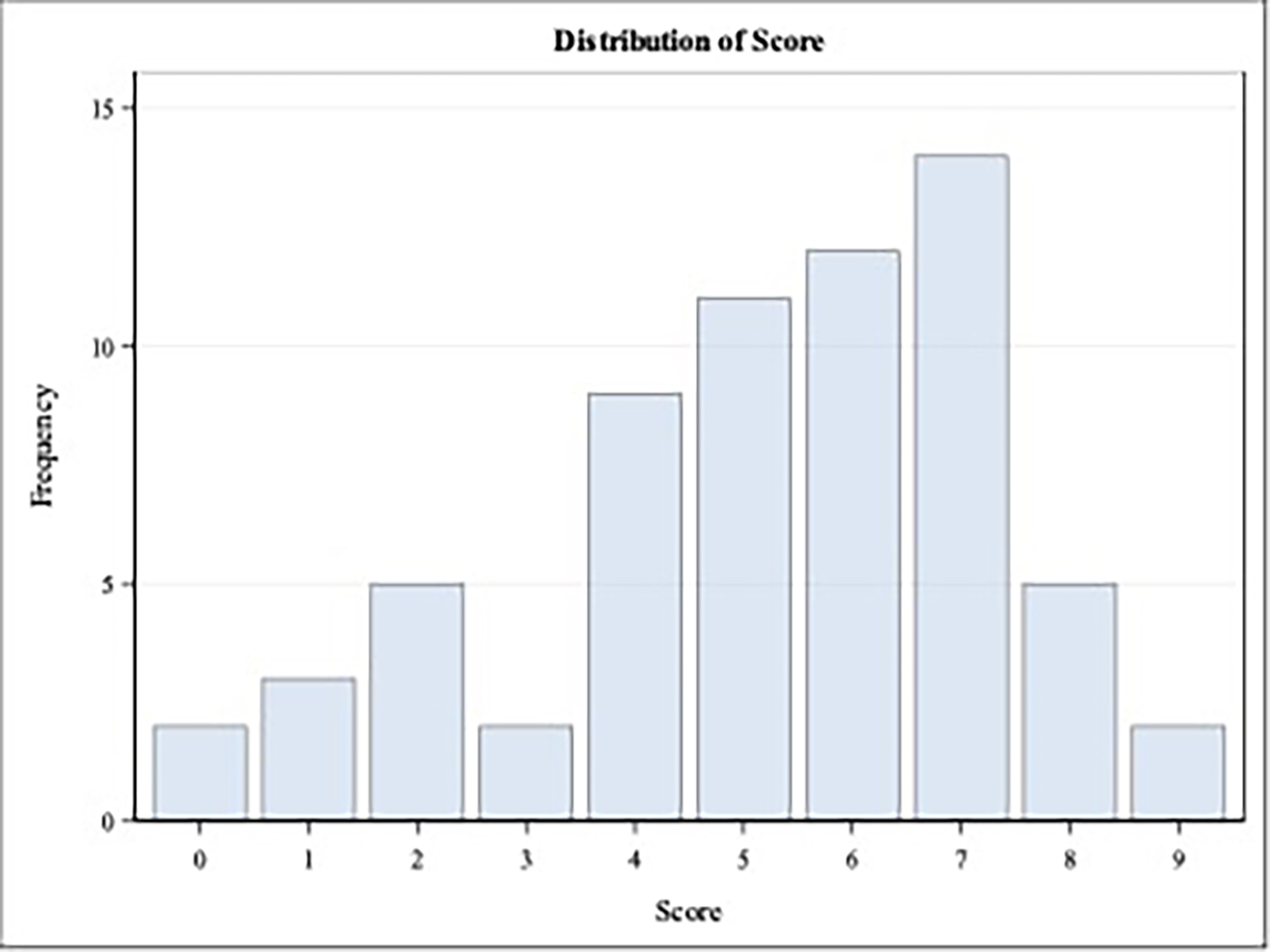
After preliminary power analysis, 65 patients completed both the LiMP and CASE assessment for validation. See tables below for baseline demographics (Tables I and II). The average age of participants was 61 years old. Most patients had a high school education or greater. The mean score for CASE and LiMP was 5.2 and 5.6, respectively. See Figures 2 and 3 for breakdowns of scoring on each assessment. Nonparametric Spearman rank-order correlation was used to compare results between CASE and LiMP surveys and found a moderate positive correlation with r = 0.572, and P < 0.001. These results suggest validation of CASE regarding its ability to accurately assess shoulder health literacy.
_survey_score_distribution.jpg)
_score_distribution.jpg)
Shoulder Arthroplasty and Health Literacy
A total of 202 patients undergoing both standard and reverse total shoulder arthroplasty responded to the mailing questionnaire CASE and LiMP surveys 3 months after surgery. A cutoff of less than or equal to a score of 4 on CASE was used to represent low health literacy. A total of 117 patients were found to have good literacy, and 85 (42%) were found to have poor literacy. Demographically, as has been shown in previous literature, White patients tended to have higher literacy than other races, and Black patients tended to have lower literacy (P < 0.05) (Rosenbaum, Pauze, Pauze, et al. 2015; Shea et al. 2004). Higher baseline education and previous healthcare experience was associated with higher scores on CASE assessment (P < 0.05). Patients with poor shoulder literacy demonstrated higher preoperative VAS score (6.4 vs. 5.4, P = .005); however, there was no difference in VAS 3 months postoperatively (2.2 vs 1.8, P = 0.121). Additionally, patients with lower health literacy tended to have lower baseline values in forward elevation (84 vs. 116), external rotation (81 vs. 114), and internal rotation (107 vs. 82), although this was not statistically significant (P > 0.05). Patients with poor shoulder literacy did not show inferior ASES (67.7 vs. 69.3, P = 0.548) or SANE (62.9 vs. 61.2, P = 0.612) scores 3 months postoperatively. There was no difference in external rotation (36.6 vs. 39.7, P = 0.143). internal rotation (40.7 vs. 40.0, P = 0.724), or forward elevation (128.1 vs. 136.0, P = 0.081) between groups at the 3-month timepoint. The change in forward elevation following surgery was greater for the patients with higher health literacy (48.8 vs. 35.9); however, this failed to reach statistical significance (P = 0.059).
DISCUSSION
This study should be interpreted as a pilot investigation designed to explore short-term associations between shoulder-specific health literacy and early postoperative outcomes. We believe several portions of this work will be important in future literature. First, the lack of a shoulder-specific health literacy assessment has been an obstacle in accurately evaluating the importance of health literacy on specific subspecialties of orthopaedics. With the wide variety of nonspecific tools used in orthopaedics currently, there is a need for standardization in the academic literature (Baker et al. 1999; Davis, Long, Jackson, et al. 1993; Gottfredson 1997; Nurss 2001; Parker et al. 1995; Weiss, Mays, Martz, et al. 2005). As shown previously, health literacy is fluid and changes between medical subspecialties based on a number of baseline patient factors. Without an accurate assessment of shoulder knowledge, it would be difficult to evaluate how interventions aimed at increasing health literacy in this area can be improved. We believe CASE provides a relatively simple, validated, and effective assessment in this area which is easy to understand across a broad range of patient backgrounds (3.6 Flesch-Kincaid).
This pilot study adds to the growing evidence that disparities in health literacy can be addressed through proper perioperative patient education and should not preclude the treatment of surgical pathologies. Consistent with prior research, lower health literacy in our population was associated with risk factors such as nonwhite race, lower baseline education, and no past healthcare experience. In our cohort alone, 42% of patients assessed were classified as having low health literacy in the early postoperative period. Previous work in the knee and spine literature would suggest lower health literacy correlates with worse patient-reported outcomes, higher pain scores, and increased complications (Puzzitiello, Colliton, Swanson, et al. 2022). Such disparities have the potential to impact surgical decision-making, potentially denying high-risk patients access to necessary care. Our study differs from previous work in that, although low health literacy was associated with higher preoperative VAS pain scores, there were no significant differences in patient-reported outcome measures, VAS pain scores, or range of motion between groups at any time point up to 3 months postoperatively. This suggests that similar outcomes can be achieved in patients undergoing shoulder arthroplasty regardless of health literacy at short term follow-up. It is important to note that considerable preoperative education was provided by the attending surgeon regarding the diagnosis and treatment modalities preoperatively, which likely had an impact on patient health literacy at the time of surgery.
While our patient follow-up was relatively short at 3 months, we believe this timeframe is justified in its representation of the immediate preoperative and postoperative shoulder arthroplasty patients, as most improvement will be seen in the first 3 months. The finding of an increased baseline in VAS score in patients with lower health literacy provides an interesting opportunity for expanding our current conservative therapy in patients with degenerative shoulder disease. Both patients with “high” and “low” health literacy VAS scores became equivalent postoperatively, perhaps indicating the effectiveness of perioperative counseling and education done by surgeons.
This study has several limitations. It was conducted at a single institution with a two-surgeon patient population, which may reduce generalizability and limit demographic diversity. Differences in preoperative and perioperative instruction may also have influenced outcomes and further restricted external applicability. Both surgeons in our cohort provide a high degree of preoperative education which may not reflect all practice environments and could limit the applicability of these findings to settings with different baseline health-literacy resources. Additionally, we included both anatomic and reverse shoulder arthroplasty patients, as well as a mix of inpatient and outpatient procedures, which introduces heterogeneity into our cohort. The follow-up period was relatively short at only 3 months postoperatively, which limits assessment of longer-term outcomes. These factors may have influenced our findings and should be considered when interpreting the results. Future work should include larger, multi-institutional cohorts with more demographic diversity, along with longer-term postoperative follow-up, to validate and expand upon these early findings.
CONCLUSIONS
CASE’s sensitivity, specificity, and Spearman correlation testing compared with the previously validated LiMP assessment indicate that it is a reliable tool in evaluating musculoskeletal-specific health literacy. While inferior shoulder health literacy was correlated with worse preoperative VAS score, it was not predictive of postoperative motion or patient-reported outcomes. Low shoulder-specific health literacy, as measured by CASE, was not predictive of worse short-term postoperative outcomes in this cohort. We hope to utilize CASE in future work to further explore how health literacy can be optimized preoperatively and also its implications in longer term follow-up.