INTRODUCTION
Anterior cruciate ligament (ACL) tears are among the most common ligamentous injuries of the knee (Davarinos, O′Neill, and Curtin 2014). For athletes, ACL injuries are particularly significant, as they result not only in immediate functional impairment but also frequently necessitate prolonged rehabilitation, delay return to sport and may even be career-ending. ACL injuries account for over 200,000 cases annually in the U.S. alone (Mall et al. 2014).
Pivoting sports such as football, basketball, and handball carry a particularly high risk of both primary ACL injuries and graft retears (Mall et al. 2014). The gold standard treatment for active individuals, especially elite athletes, is anterior cruciate ligament reconstruction (ACLR) (Buerba et al. 2021). However, the optimal autograft choice remains a topic of debate. Despite the widespread adoption of ACLR, uncertainty persists over which graft offers the best combination of durability, safety, and performance, particularly in athletic populations.
Traditionally, hamstring tendon (HT) and bone–patellar tendon–bone (BPTB) autografts have been the most used grafts. While the use of HT grafts are widely employed in the general population, their limitations, such as reduced knee stability and longer incorporation times, make them less suitable for professional athletes with high biomechanical demands (Fineberg, Zarins, and Sherman 2000; Middleton et al. 2014). In contrast, BPTB autografts have been preferred in athletes for their lower retear rates and greater postoperative stability (Slone et al. 2015). However, BPTB use is also associated with increased risks of anterior knee pain, patellar fractures, and donor site morbidity (Kraeutler, Bravman, and McCarty 2013). These complications have prompted interest in alternative graft options that provide comparable biomechanical strength while minimizing adverse outcomes.
Recently, the quadriceps tendon (QT) has emerged as a promising alternative graft for anterior cruciate ligament reconstruction (ACLR). This graft combines several advantages of the BPTB graft, including high strength and stability, while offering additional benefits like a larger cross-sectional area (2.5 to 3 cm at its thickest point) and reduced donor site morbidity (Slone et al. 2015). These advantages have been supported by multiple systematic reviews and meta-analyses comparing QT and BPTB grafts in the general population (Dai et al. 2022; Kurkowski et al. 2025; Mouarbes et al. 2019). However, to date, no previous meta-analysis has focused specifically on athletes, who have different physical demands, performance goals, and injury risks than the general population.
In addition, existing reviews have largely been narrative or lacked quantitative synthesis, revealing a methodological gap in the literature. To our knowledge, no meta-analysis to date has specifically addressed this question in an athletic population.
Therefore, this systematic review and meta-analysis aimed to compare clinical outcomes between bone–patellar tendon–bone (BPTB) and quadriceps tendon (QT) autografts in athletes undergoing ACL reconstruction. The analysis focuses on graft failure rates, return to sport, patient-reported outcomes (including Lysholm and IKDC scores), and the certainty of evidence supporting these findings.
METHODS
Protocol and Registration
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page, McKenzie, Bossuyt, et al. 2021) and the PERSiST guidance for implementing PRISMA in sport and exercise medicine, musculoskeletal rehabilitation, and sports science (Ardern et al. 2022). The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420251067999.
Eligibility Criteria
Studies were eligible for inclusion if they involved athletes, defined as individuals participating in competitive or high-demand sports, who underwent primary anterior cruciate ligament reconstruction (ACLR) using either quadriceps tendon (QT) autografts or bone-patellar tendon-bone (BPTB) autografts. Only studies directly comparing QT and BPTB autografts were included. Eligible study designs comprised randomized controlled trials and observational studies (prospective or retrospective cohorts) that reported at least one clinical and functional outcome such as graft failure, return to sport, Lysholm score, or International Knee Documentation Committee (IKDC) score. Studies involving pediatric populations, multi-ligament injuries, or including graft types other than QT or BPTB were excluded. Additional exclusion criteria included studies not reporting outcomes of interest, case reports, case series, reviews, editorials, conference abstracts without full texts, animal or cadaveric studies, biomechanical or technical studies without clinical outcome data, and studies with mixed populations where data specific to athletes or graft types could not be separately extracted. Only studies published in English, Spanish, French, or Italian up to March 2025 were considered eligible. Quadriceps tendon grafts may be harvested as either soft-tissue–only or with a patellar bone block. However, none of the included studies reported outcomes stratified by QT subtype. Therefore, QT grafts were analyzed as a single category. Hamstring tendon autografts were intentionally excluded because they differ substantially from BPTB and QT in structure, fixation, healing biology, and return-to-sport timelines. Including hamstrings would introduce clinical heterogeneity and shift the study away from the focused comparison of QT vs BPTB in athletes.
Information Sources and Search Strategy
A systematic search of the published literature was conducted across four major databases: PubMed, EMBASE, the Cochrane Library, and Web of Science. The search included studies published up to 2025, with no restriction on the start date, to ensure a broad capture of relevant literature. Additional sources, such as clinical trial registries and reference lists of included studies, were also screened. The search terms included combinations of keywords and medical subject headings (MeSH), connected with Boolean operators. The search strategy combined keywords and MeSH terms using Boolean operators, adapted to each database’s indexing to optimize retrieval, The search terms included:
(“Athlete” OR “High-Impact Sport” OR “Football” OR “Soccer” OR “High-Demand Sports”) AND (“Anterior Cruciate Ligament” OR “ACL”) AND (“quadriceps tendon” OR “quadriceps soft tissue”) AND (“Patellar Tendon” OR “Patellar Tendon Autograft” OR “bone-patellar tendon-bone”).
Selection Process
All records identified through the search strategy were screened by four independent reviewers during the title/abstract stage. Discrepancies between reviewers were resolved through discussion or with the involvement of two other reviewers when necessary. The automation tool Rayyan© (2025 Cambridge, MA, USA) (Ouzzani, Hammady, Fedorowicz, et al. 2016) was used to facilitate the screening process by allowing blinded, independent screening and helping identify conflicts efficiently. However, no machine learning classifiers were used to eliminate records automatically or replace human screeners. No crowdsourcing methods or pre-screened datasets were used. No additional contact with study authors was necessary to confirm study information. Full texts of potentially relevant articles were assessed independently.
Data Collection Process
Data extraction was performed independently by three reviewers using a standardized form. Extracted data included study design and characteristics, follow-up duration, participant demographics, graft type, and clinical and functional outcomes. Disagreements were resolved through discussion. No automation tools or machine learning software were used for data extraction. No contact with study authors was made to obtain or verify data. In cases where multiple reports referred to the same study population, the most complete and recent version was included to avoid duplication.
Data Items
The primary outcomes extracted were graft failure and return to sport, which were considered the most clinically relevant endpoints for athletic populations undergoing ACL reconstruction. Secondary outcomes included the Lysholm score and IKDC score, used to assess functional recovery. Outcomes were extracted at the longest follow-up reported in each study, with a minimum follow-up duration of two years. All available results within each outcome domain were considered; when multiple time points were reported, data from the latest follow-up were prioritized. Additional variables collected included patient age, sex, meniscectomy or meniscus repair status, and follow-up duration. No changes were made to the outcome domains or the criteria for selecting outcomes during the review process.
Risk of Bias Assessment
Risk of bias was assessed independently by two reviewers using the Cochrane Risk of Bias 2.0 (RoB-2) tool for randomized controlled trials and the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool for observational studies. Each domain was rated as low risk, some concerns, or high risk of bias. Disagreements were resolved through discussion and consensus. No automation tools were used in the assessment process.
Effect Measures
For dichotomous outcomes (graft failure and return to sport), odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. For continuous outcomes (Lysholm and IKDC scores), mean differences (MDs) with 95% CIs were used. Although standardized mean differences (SMDs) are commonly used when measurement scales differ, they were not necessary in this review since all included studies reported outcomes on consistent scales. If applicable, SMDs would have been interpreted using Cohen’s thresholds: 0.2 (small), 0.5 (moderate), and ≥0.8 (large). No transformation or re-expression of synthesized results into alternative effect measures wasperformed.
Statistical heterogeneity was assessed using the I² statistic, with thresholds of 25%, 50%, and 75% interpreted as low, moderate, and high heterogeneity, respectively. All analyses were conducted using Review Manager (RevMan) version 5.4 (The Cochrane Collaboration 2020). A sensitivity analysis was performed by excluding the Renfree 2023 study to assess its impact on the pooled estimate and heterogeneity.
Synthesis
Eligibility for each synthesis was determined by tabulating study characteristics, including graft type, study design, participant demographics, and outcome measures. Only studies that directly compared quadriceps tendon (QT) and bone–patellar tendon–bone (BPTB) autografts in athletes, and that reported data for at least one of the predefined outcomes (graft failure, return to sport, Lysholm score, or IKDC score) were included in quantitative synthesis. For dichotomous outcomes (e.g. graft failure, return to sport), if studies reported results as percentages, the absolute number of events was inferred by applying the reported percentage to the total sample size. Individual study characteristics and outcome data were presented in structured summary tables. Results of meta-analyses were visually displayed using forest plots, showing effect estimates and 95% confidence intervals for each study and the pooled estimate. Risk of bias assessments were summarized in tables, and risk of bias graphs were generated in Review Manager (RevMan) (The Cochrane Collaboration 2020). Due to the limited number of studies, subgroup analyses and sensitivity analyses could not be performed.
Reporting Bias Assessment
Despite the limited number of included studies (n=3), formal assessment of publication bias using funnel plots was still performed. Additionally, reporting bias was qualitatively assessed based on the comprehensiveness of the literature search and examination of trial registries.
Certainty Assessment
The certainty of evidence for each outcome was evaluated using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach. The assessment considered five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Based on these criteria, the overall certainty of evidence was rated as high, moderate, low, or very low. Judgments were made independently by two reviewers, and disagreements were resolved by consensus. The results were summarized in a Summary of Findings (SoF) table.
Equity, diversity and inclusion (EDI). We used inclusive eligibility (no restrictions by sport, sex or competitive level). Full-text assessment was limited to English/spanish/french/italian due to resource constraints, which may introduce language bias.
RESULTS
Study selection
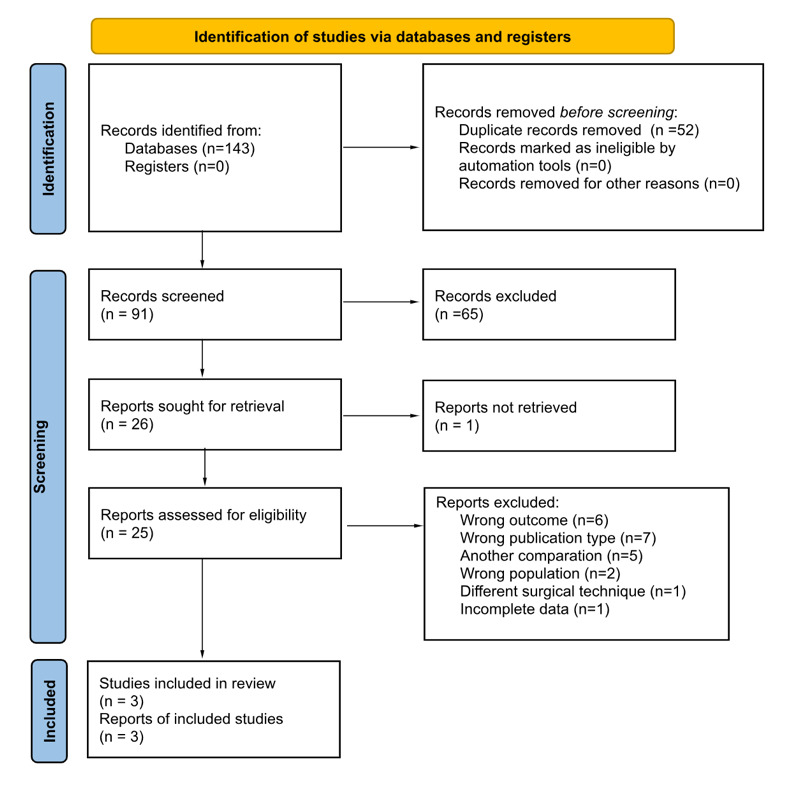
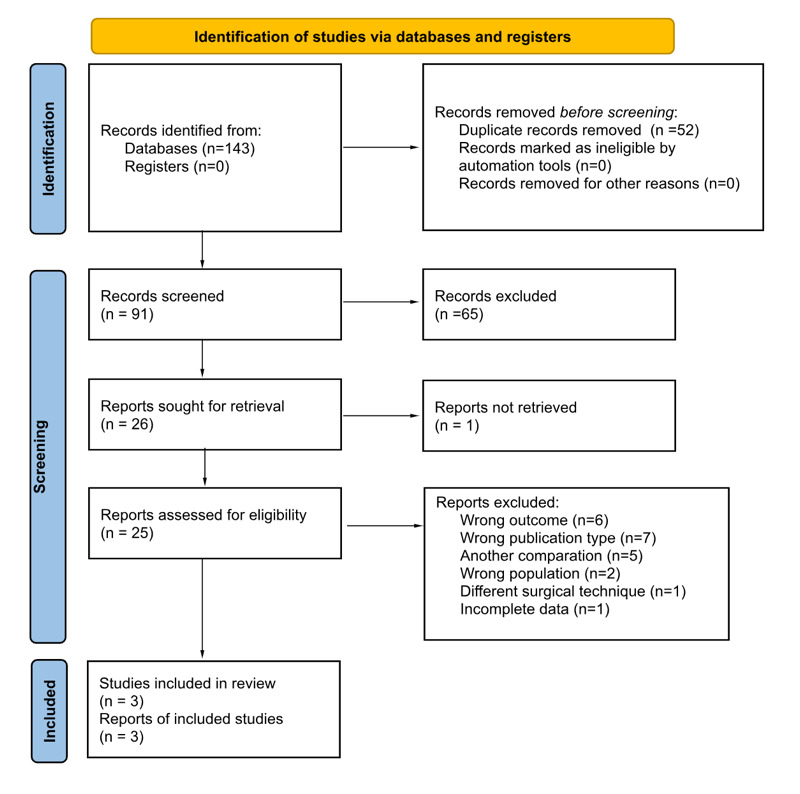
A total of 143 records were identified through database searching. After removing duplicates, 91 records remained for title and abstract screening. Of these, 65 were excluded based on irrelevance to the research question. The full texts of 25 articles were assessed for eligibility, of which 6 were excluded due to wrong outcomes, 7 due to publication type (e.g., review articles or conference abstracts), 5 due to an ineligible population, 1 due to an incorrect surgical technique, and 1 due to incomplete reported data. Finally, 3 studies met the inclusion criteria and were included in both the qualitative synthesis and the meta-analysis (Renfree et al. 2023a; Herman et al. 2023; Barie et al. 2020).
The study selection process is illustrated in the PRISMA flow diagram (Figure 1A).
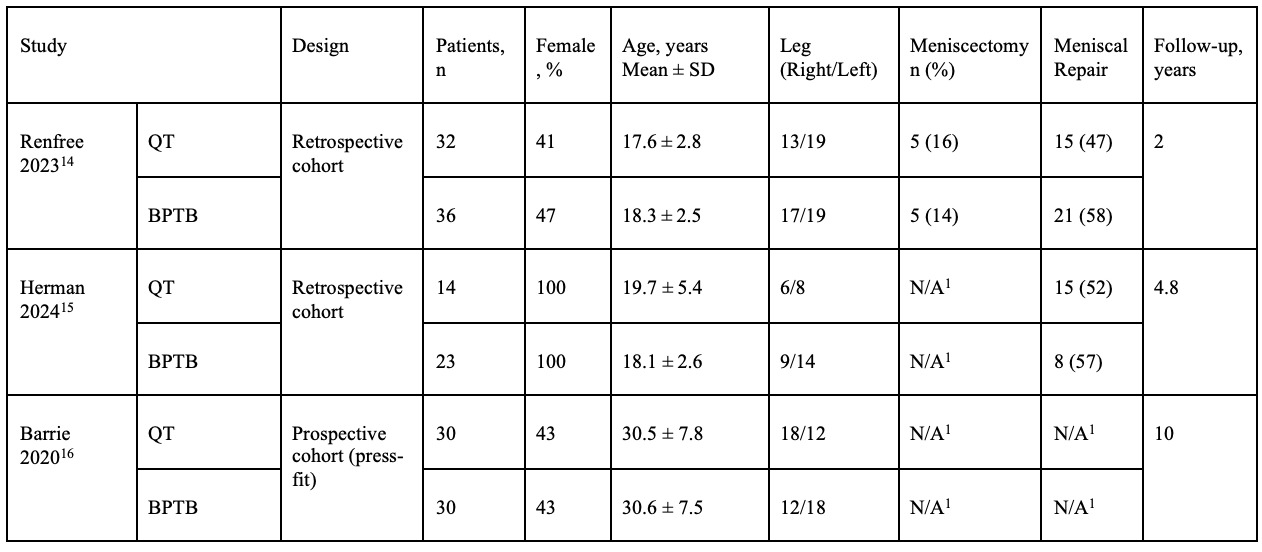
Study Characteristics
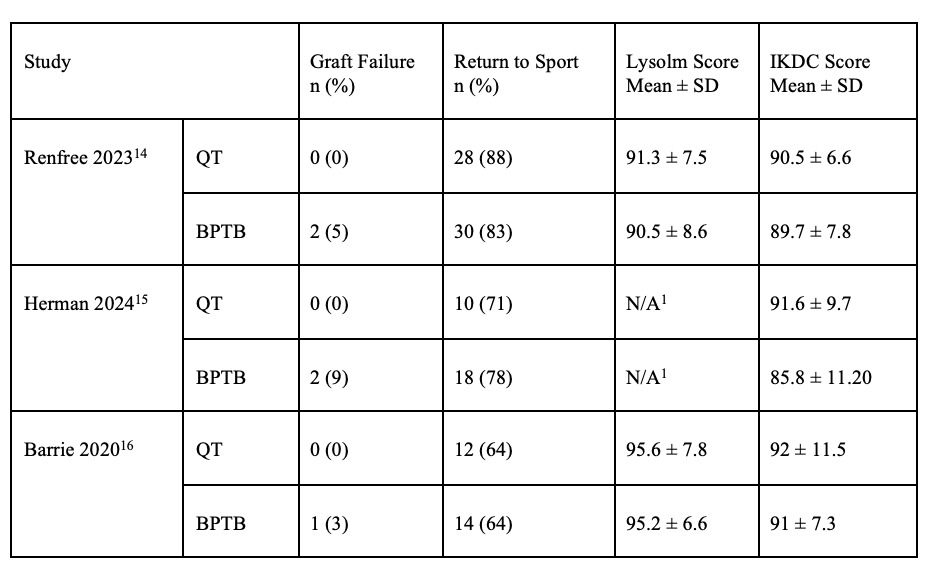
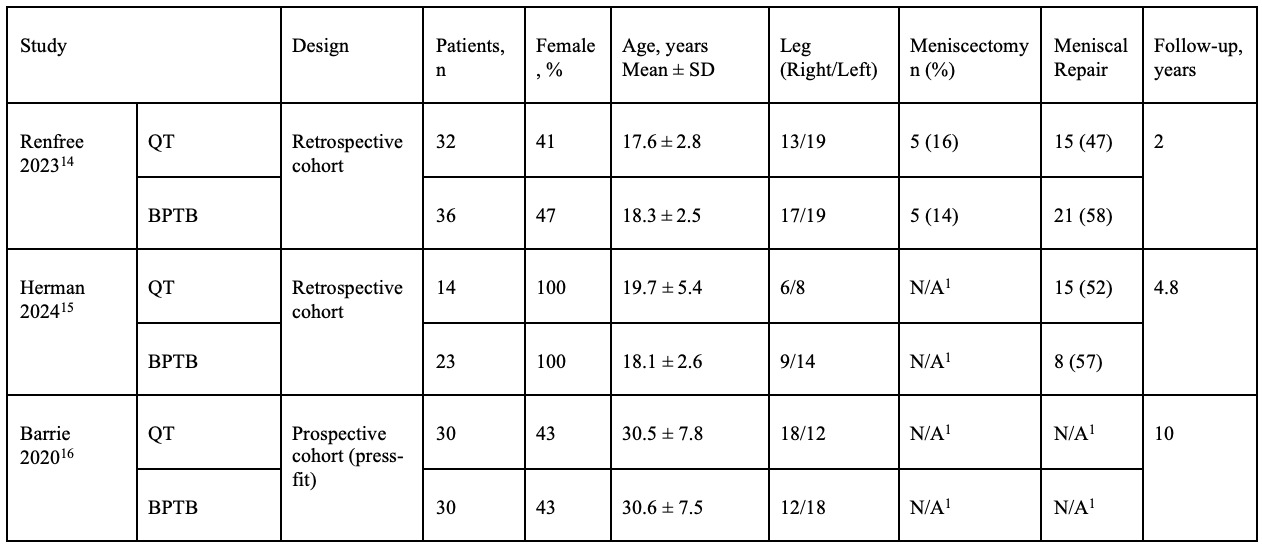
The three included studies were conducted in athletic populations undergoing anterior cruciate ligament (ACL) reconstruction using either quadriceps tendon (QT) or bone–patellar tendon–bone (BPTB) autografts. Study characteristics are summarized in Table 1, including design type, patient demographics, laterality, concomitant meniscal procedures, and follow-up duration. These parameters provide the clinical context for evaluating the comparative outcomes of each graft type. Although QT grafts can be constructed with or without a patellar bone block, none of the included studies provided separate subgroup outcomes. As such, we were unable to perform QT subtype–specific analysis.
Risk of bias
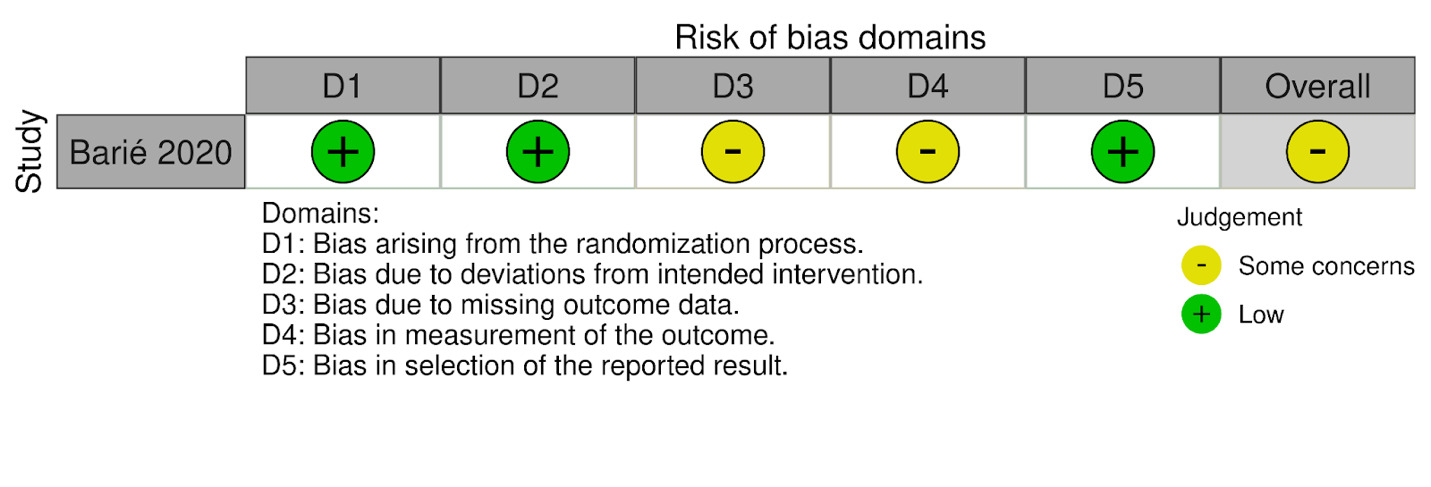
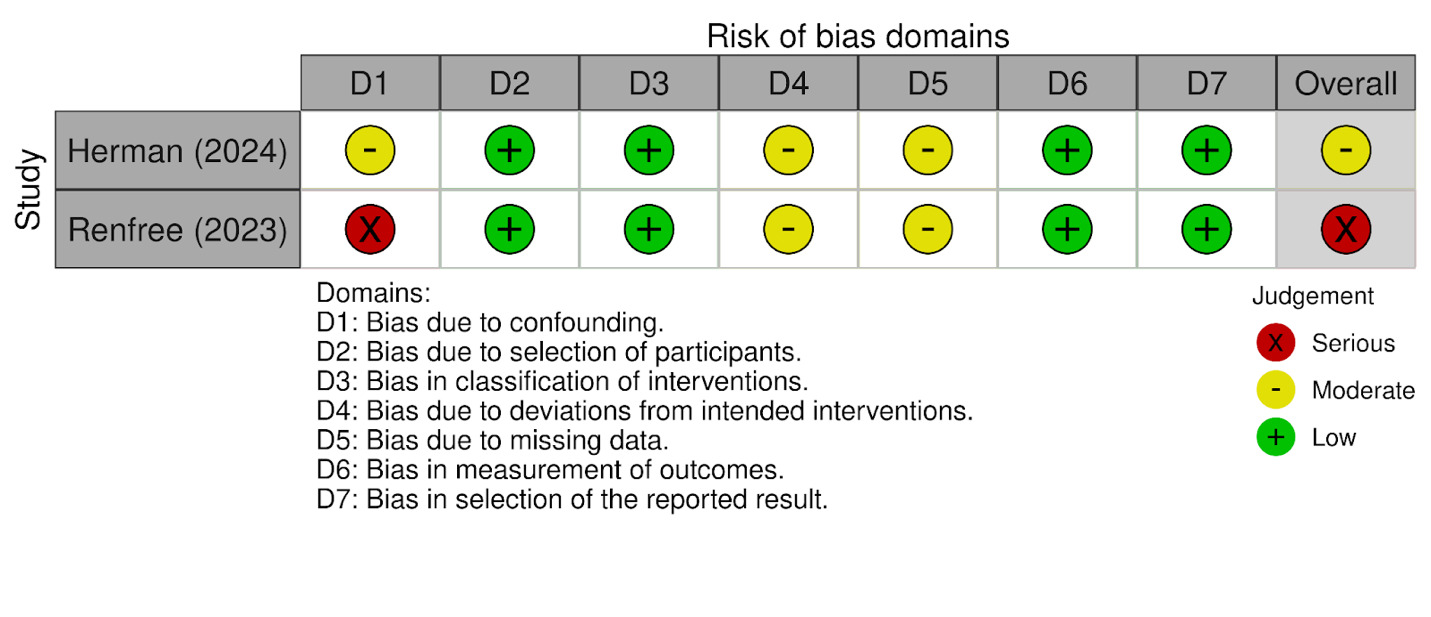
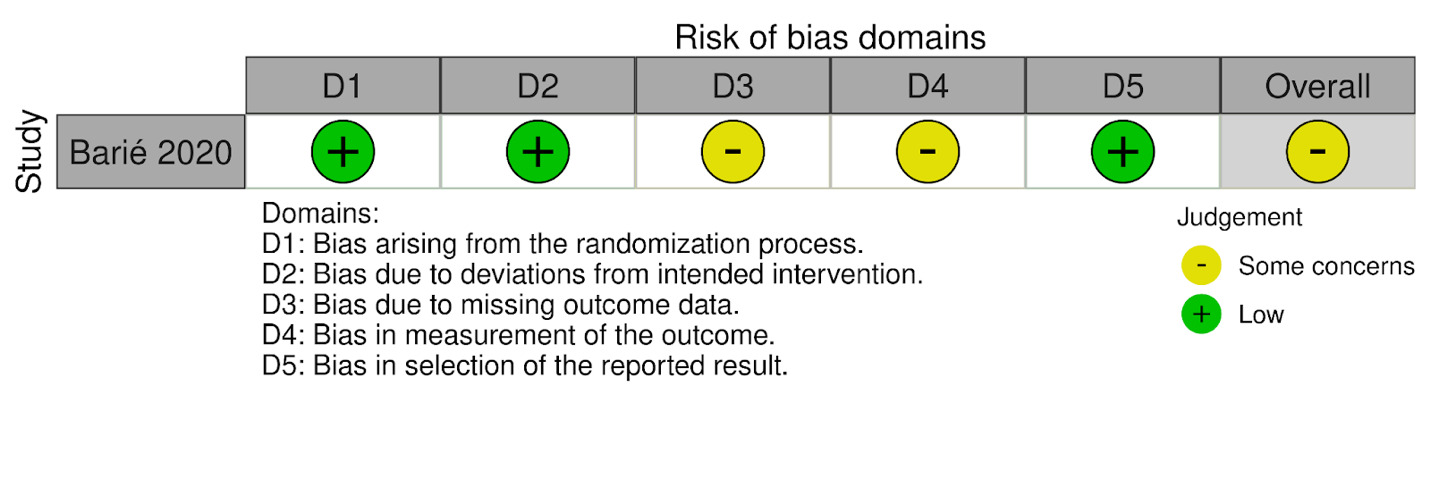
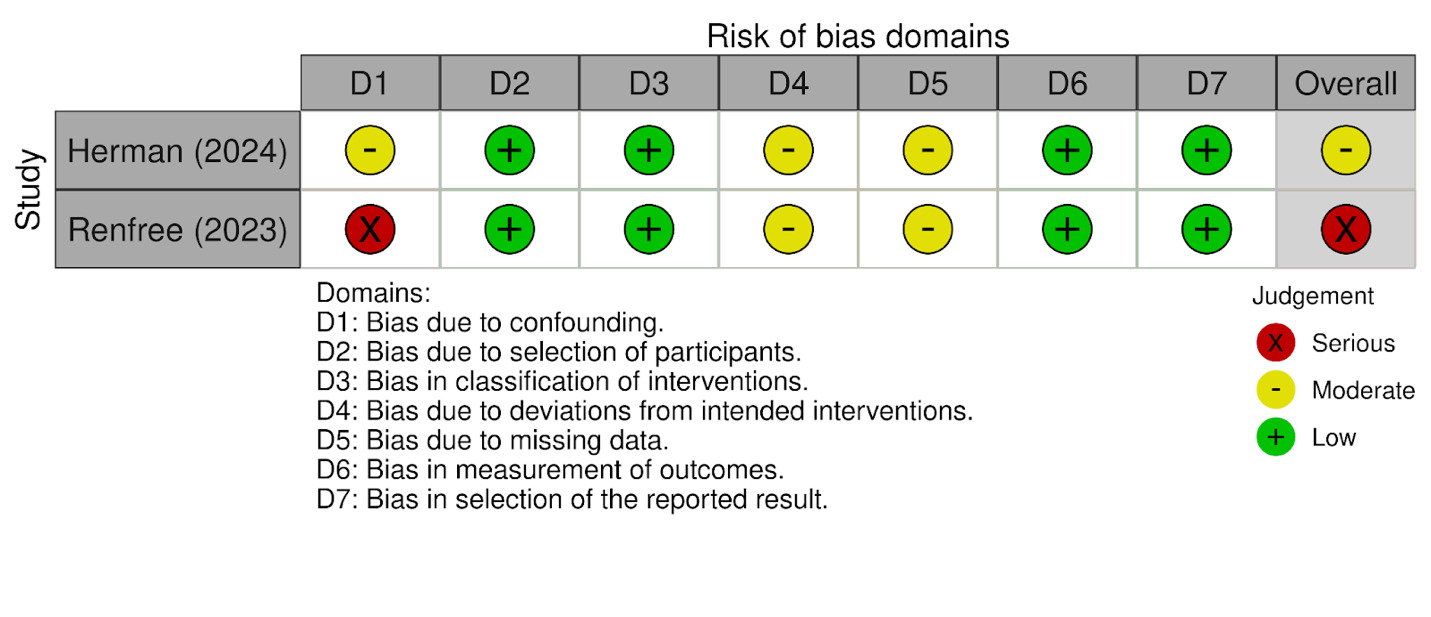
Risk of bias was assessed using the ROBINS-I tool and RoB-2, and visualizations were generated using the robvis web application (McGuinness and Higgins 2020). Of the three studies included, two were judged to have some concerns, and one was considered to have a high risk of bias. The most frequent limitations were related to a lack of blinding and incomplete outcome data. The single randomized study (Barié 2020) showed an overall judgment of “some concerns,” primarily due to missing outcome data and potential issues in outcome measurement. Among the non-randomized studies, Herman (2024) was rated as having a “moderate” overall risk of bias, with concerns mainly related to confounding and deviations from intended interventions. Renfree (2023) was judged to have a “serious” risk of bias, driven primarily by confounding and potential selective reporting.
A visual summary of the domain-level judgments for each study is presented in Figure 2A (RoB-2 summary) and Figure 2B (ROBINS-1 summary).
Risk of bias summary for randomized studies (RoB-2) and Risk of bias summary for non-randomized studies (ROBINS-I)
Results of individual studies
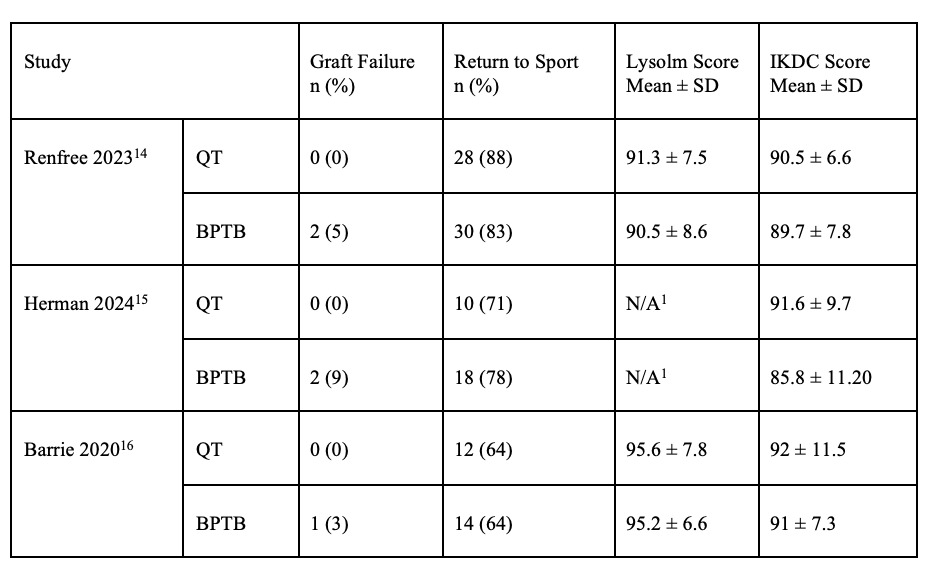
The three included studies reported clinical outcomes following ACL reconstruction with either quadriceps tendon (QT) or bone–patellar tendon–bone (BPTB) autografts in athletic populations. Key outcome measures are summarized in Table 1, including graft failure rates, return to sport percentages, and functional scores such as the Lysholm and IKDC. Across studies, outcome trends were evaluated to compare the efficacy and safety of each graft type. Forest plots further illustrate the pooled effects for each variable, allowing visual interpretation of between-study differences and overall effect estimates.
Statistical Synthesis
Graft Failure
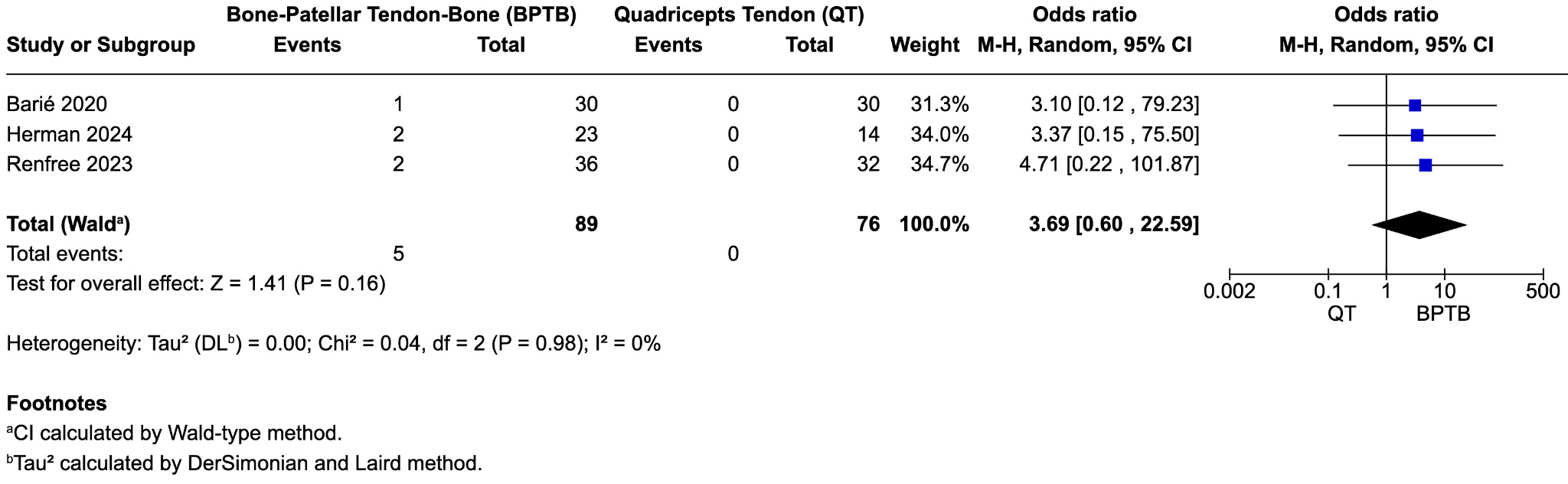
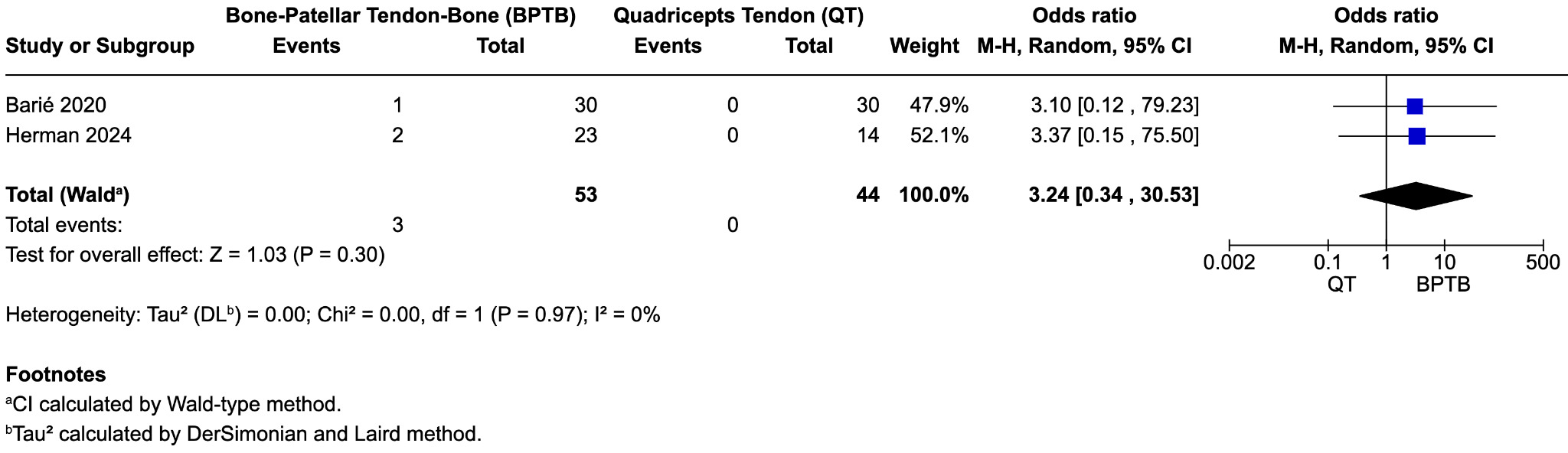
Three studies (Barié et al. 2020; Herman et al. 2024; Renfree et al. 2023) reported on graft failure following ACL reconstruction. The pooled analysis showed no statistically significant difference in graft failure rates between bone–patellar tendon–bone (BPTB) and quadriceps tendon (QT) autografts (odds ratio [OR] = 3.69; 95% confidence interval [CI], 0.60 to 22.59; p = 0.16; I² = 0%) (Figure 3A). Across the included studies, five graft failures were reported in the BPTB group (two in Renfree, two in Herman, one in Barie), and none in the QT group. Due to the low event rate and wide confidence interval, definitive conclusions could not be drawn. Odds ratios were used for dichotomous outcomes due to rare event frequency and methodological robustness.
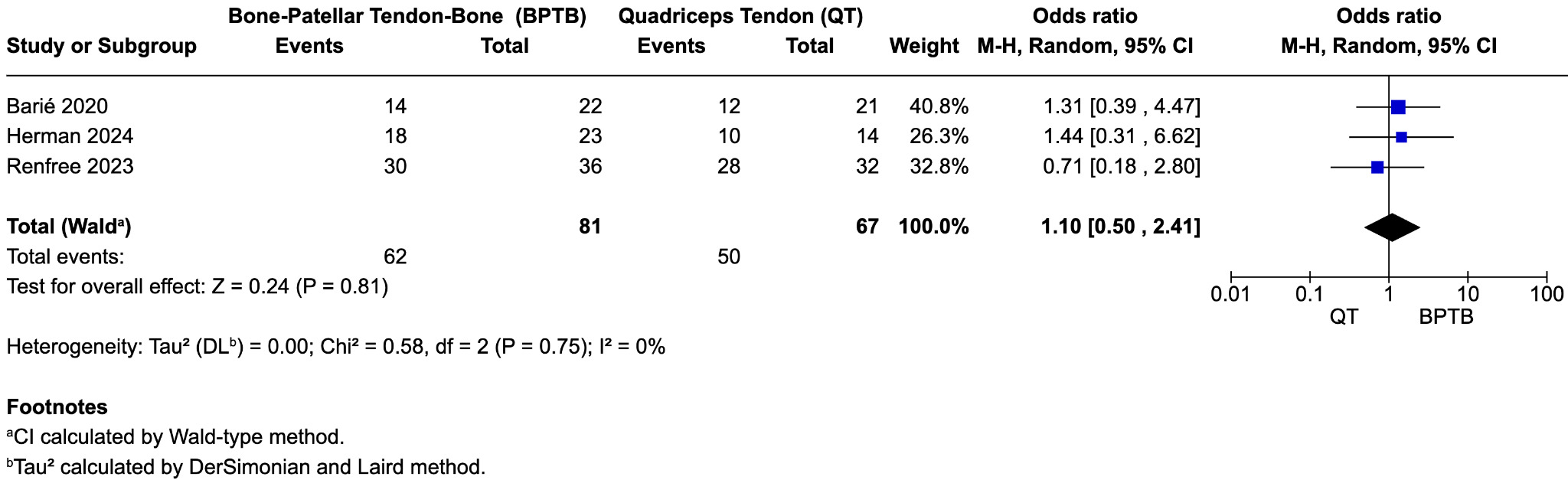
Return to Sport
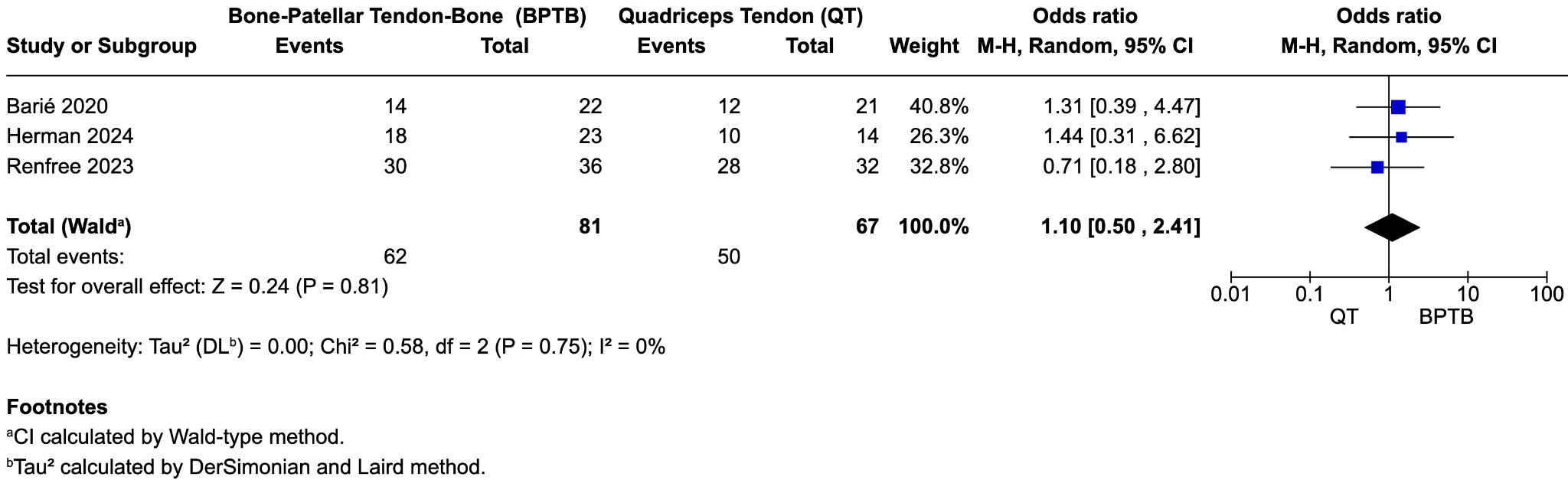
All three studies reported data on return to sport (RTS), generally defined as a return to preinjury activity level, primarily assessed using the Tegner activity scale. Meta-analysis showed no significant difference in RTS rates between BPTB and QT grafts (OR = 0.90; 95% CI, 0.37 to 2.20; p = 0.81; I² = 0%) (Figure 3B). In Barié et al., 64% of patients returned to their preinjury activity level by 10-year follow-up, with no statistically significant difference between BPTB and QT groups (p = 0.960). Because graft-specific RTS counts were not reported, we imputed events proportionally based on group size (14/22 BPTB, 12/21 QT) to preserve the published total of 27 responders. These counts were used in the meta-analysis under the assumption of group-level equivalence. Findings suggest comparable long-term functional recovery in athletes undergoing ACL reconstruction with either graft type.
Lysholm Score
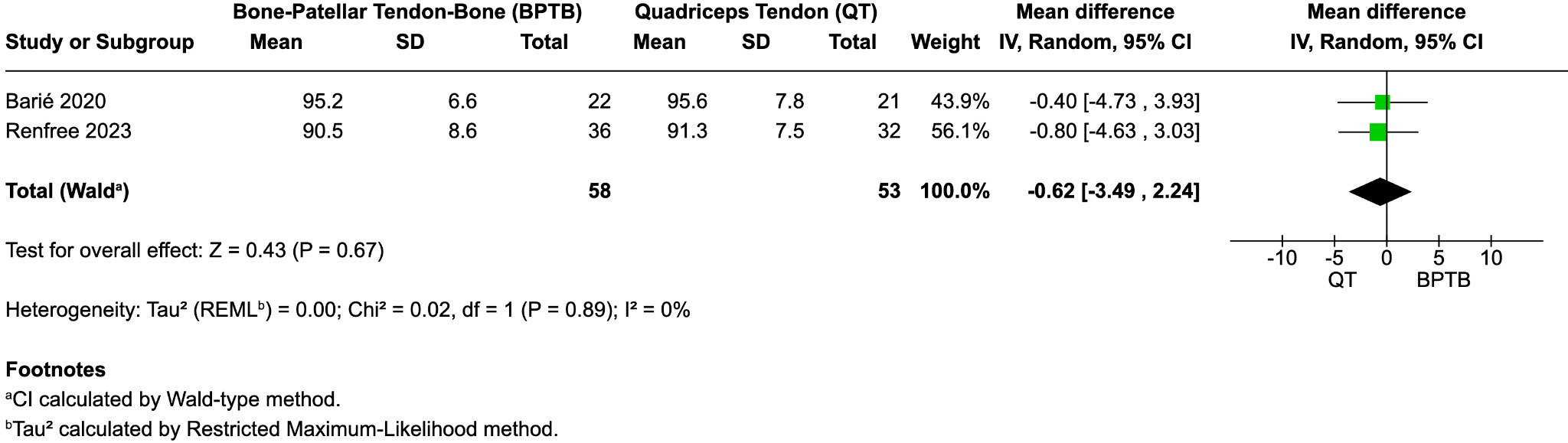
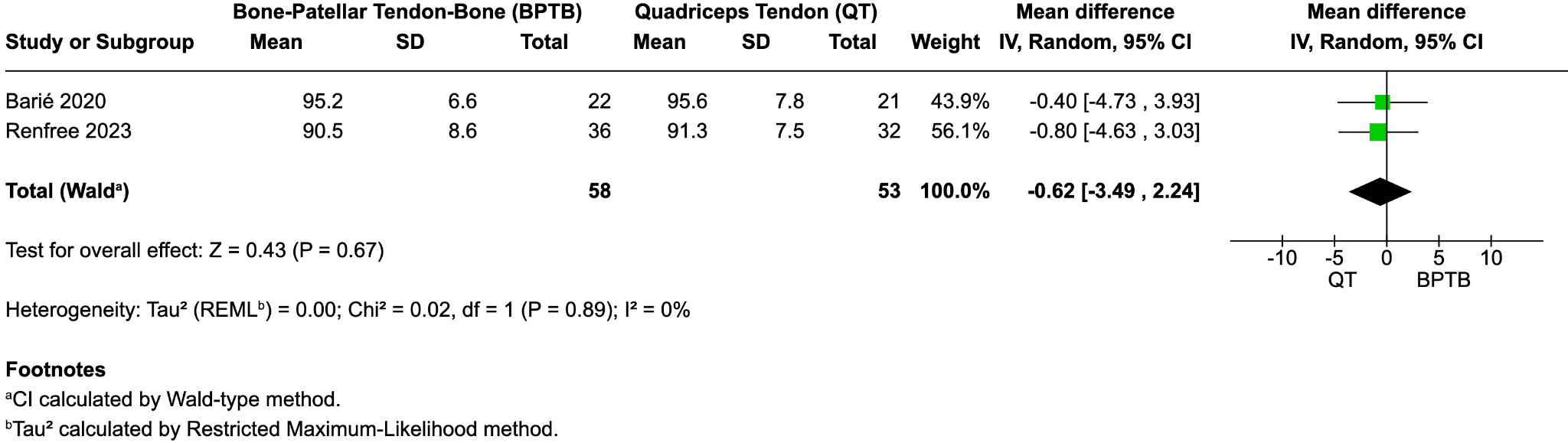
Two studies (Barié et al. 2020; Renfree et al. 2023) reported Lysholm scores at final follow-up. The pooled mean difference between groups was not statistically significant (mean difference = –0.62; 95% CI, –3.49 to 2.24; p = 0.67; I² = 0%) (Figure 3C). Both BPTB and QT groups demonstrated high postoperative Lysholm scores, indicating satisfactory subjective knee function.
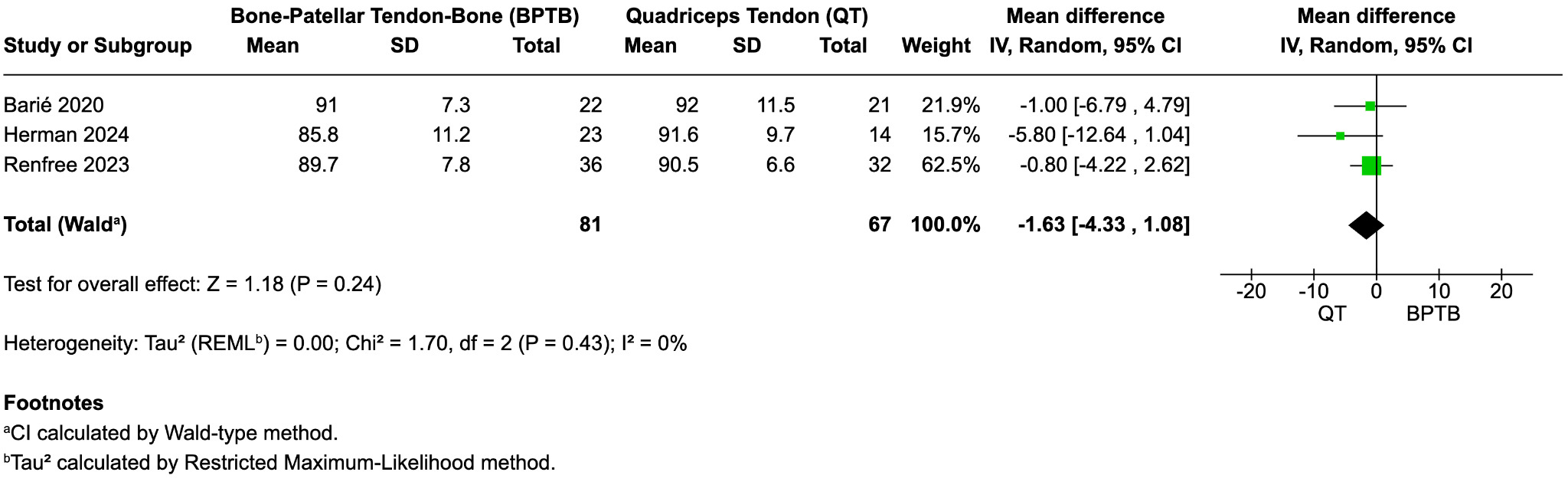
IKDC Score
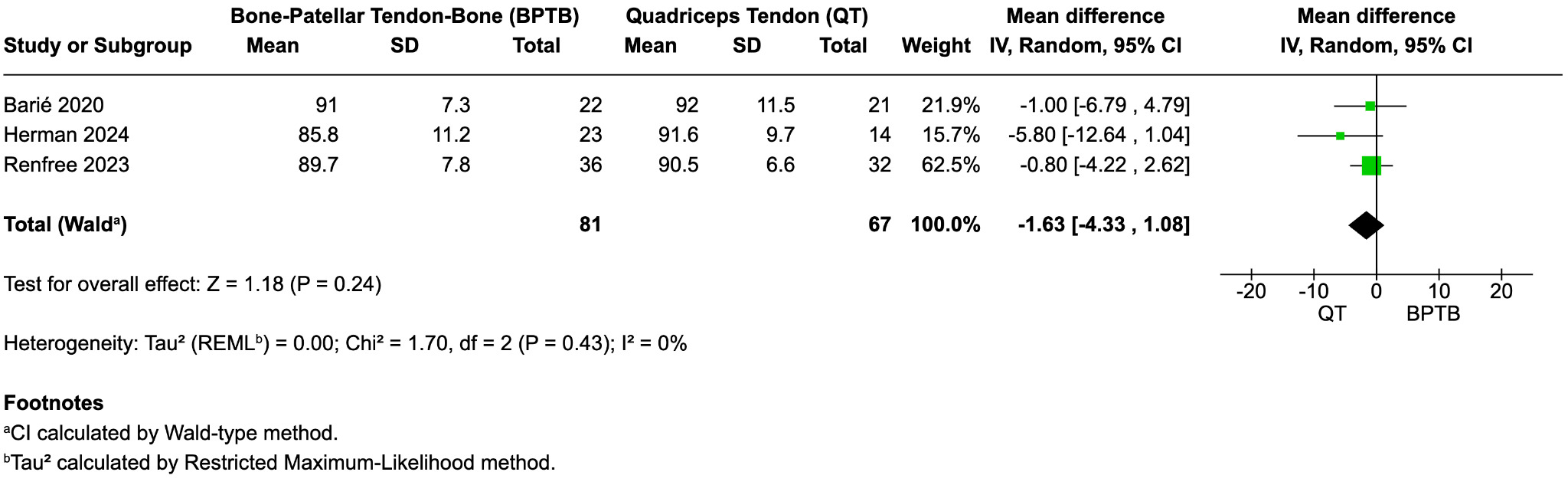
All three studies reported subjective IKDC scores at final follow-up. Pooled analysis revealed no significant difference between graft types (mean difference = –1.63; 95% CI, –4.33 to 1.08; p = 0.24; I² = 0%) (Figure 3D). Mean IKDC scores ranged from 85.8 to 92 across studies, suggesting favorable outcomes for both QT and BPTB autografts.

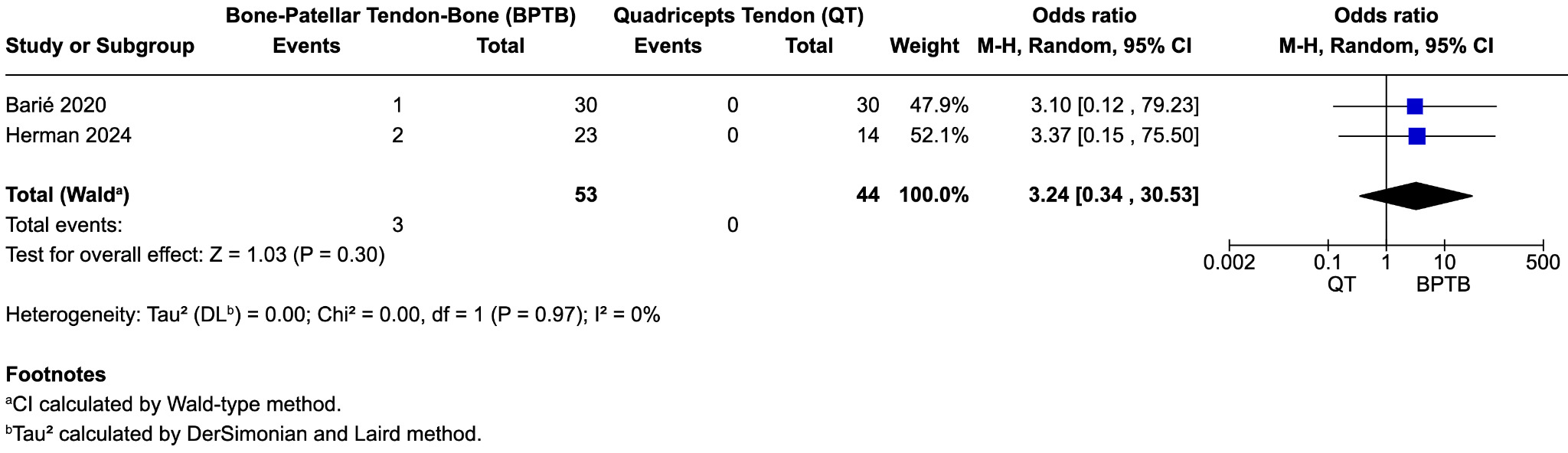
Sensitivity analysis
Given the small number of studies included, formal assessment of publication bias was not feasible. A sensitivity analysis was performed by excluding the Renfree 2023 study to assess the robustness of the overall findings. Upon removal, the pooled odds ratio decreased slightly from 3.69 (95% CI: 0.60-22.59) to 3.24 (95% CI: 0.34-30.53), and the heterogeneity remained at 0% (I² = 0%). The direction of effect remained consistent, indicating that the overall results are stable and not influenced by any single study.
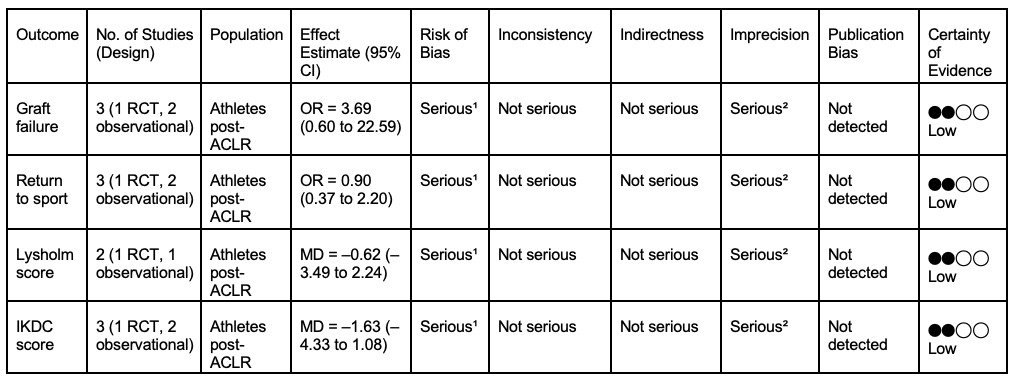
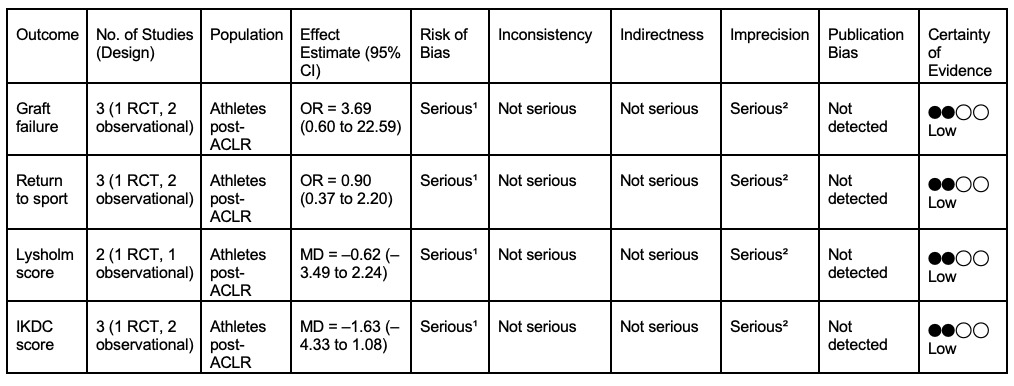
Certainty of evidence
Table 2 presents the pooled effect estimates for each outcome, along with the certainty of evidence as assessed by the GRADE approach. The certainty of evidence was rated as low for all outcomes, mainly due to study methodological limitations and imprecision.
DISCUSSION
This systematic review and meta-analysis compared quadriceps tendon (QT) and bone–patellar tendon–bone (BPTB) autografts in athletes undergoing anterior cruciate ligament reconstruction (ACLR). The pooled analysis revealed no statistically significant difference in graft failure between QT and BPTB autografts (OR = 3.69; 95% CI, 0.60 to 22.59; p = 0.16). Similarly, return to sport outcomes were statistically equivalent (OR = 0.90; 95% CI, 0.37 to 2.20; p = 0.81). Functional scores measured by Lysholm score (MD = –0.62; 95% CI, –3.49 to 2.24; p = 0.67) and IKDC score (MD = –1.63; 95% CI, –4.33 to 1.08; p = 0.24) were also comparable, with both groups demonstrating high postoperative values. These findings suggest equivalent clinical performance between QT and BPTB autografts in athletic populations. An important methodological point is that QT grafts can be harvested as soft-tissue or bone-block constructs, which differ biomechanically. However, the included studies did not report outcomes stratified by QT subtype, preventing subgroup comparison. This limitation should be addressed in future athlete-specific studies.
While previous meta-analyses have reported similar outcomes for QT and BPTB autografts in general populations (Dai et al. 2022; Kurkowski et al. 2025; Mouarbes et al. 2019), this study is the first to restrict inclusion to competitive or high-demand athletes. This is a critical distinction, as athletes often face higher reinjury risk, greater physical demands, and greater pressure for accelerated return to sport. Despite these elevated performance expectations, QT autografts did not show inferiority, supporting their viability in elite athletic settings.
From a biomechanical perspective, QT grafts offer several theoretical advantages, including a larger cross-sectional area and reduced donor site morbidity. Additionally, unlike BPTB grafts, they are associated with a lower incidence of anterior knee pain and kneeling discomfort, features particularly relevant for athletes in sports requiring frequent contact with the ground, kneeling, sprinting or explosive knee extension such as wrestling, football or track and field (Slone et al. 2015; Kraeutler, Bravman, and McCarty 2013). Despite these advantages, QT autografts remain underutilized, largely due to concerns about surgical familiarity and limited long-term outcome data.
Emerging evidence from large cohort studies and long-term follow-ups, such as those by Mouarbes et al. and Kurkowski et al (Kurkowski et al. 2025; Mouarbes et al. 2019)., supports the safety and durability of QT grafts even in young and athletic patients. The present findings from our meta-analysis reinforce this growing body of literature, suggesting that QT grafts may offer a safe and effective alternative to BPTB grafts, without compromising functional recovery or increasing failure risk.
Graft failure remains a central concern in anterior cruciate ligament reconstruction (ACLR), with outcomes influenced by factors such as graft type, patient demographics, chronicity of ACL deficiency, and surgical technique. Early graft failure is more prevalent in patients with chronic ACL deficiency, particularly when the duration exceeds two years, with bone–patellar tendon–bone (BTB) autografts demonstrating the lowest failure rates in this subgroup (9.2%) (Tanaka et al. 2023). It has also been noticed that graft failures occur nearly twice as often in revision ACL repairs compared to primary procedures (Ouillette et al. 2019). Among adolescent athletes, quadriceps tendon (QT) autografts have shown a lower risk of graft failure, despite an increased rate of ipsilateral reoperations. Surgical nuances also appear to influence failure rates, with increased failure risk in BTB reconstructions associated with greater patellar tendon thickness at the inferior and longitudinal midpoint (Kanakamedala et al. 2019), whereas other studies observed no significant difference in failure rates between full-thickness and partial-thickness QT grafts (Laboute et al. 2018). Laboute et al (Samuelsen et al. 2017) found that younger athletes, particularly those under 25 years of age a higher incidence of graft failure. In the same study, BTB grafts were associated with a longer mean time to failure (17.4 months) compared to hamstring tendon (HT) grafts (10.7 months). A meta-analysis published on the subject confirmed that BTB grafts had significantly lower short- to mid-term failure rates compared to hamstring autografts, though both demonstrated low failure rates with long-term follow-up (Salem et al. 2019a). Similarly, reports were made of low failure rates in young wrestlers who received BTB grafts versus HT grafts (Marigi et al. 2022), and Salem et al (Salem et al. 2019b) highlighted that female sex and younger age remain significant risk factors for graft failure. Meanwhile, other studies (Li, Gu, and Wei 2020) (Renfree et al. 2023b) reported no significant difference in failure rates when comparing BTB and QT autografts.
Return to sport (RTS) is one of the critical benchmarks of success in anterior cruciate ligament reconstruction (ACLR), particularly for athletes. However, rates and timelines of RTS can vary significantly depending on graft type, patient demographics, surgical history, and psychosocial factors. RTS rates are unexpectedly lower in revision ACLR compared to primary procedures, underscoring the impact of surgical history (Ouillette et al. 2019). A systematic review on the use of QT with the bone block (QT-B) and without bone block (QT-S) in ACLR found that approximately 80% of patients returned to sport at a mean of 24 months postoperatively (Meena et al. 2023). However, return to pre-injury levels of sport was substantially lower, with multiple studies, including Renfree et al, reporting that only 50–70% of patients achieved their previous performance level. Psychological barriers were also prominently observed; fear of reinjury was cited by nearly half of patients who failed to return to sport, while 70% attributed their non-return to lack of time (Dadoo et al. 2024). Graft type appears to influence outcomes, with BPTB autografts yielding an 80% RTS rate in competitive wrestlers at 15-year follow-up, outperforming hamstring grafts (Marigi et al. 2022). Similarly, another meta-analysis found higher RTS rates in BTB grafts than hamstring graft (Xie et al. 2015). In contrast, Brinkman et al noted that patients receiving QT autografts returned to sport earlier (mean 8.9 months) compared to those receiving BTB grafts (10.3 months), although no significant difference in overall RTS rates between BPTB and QT autografts was found (Brinkman, Tummala, and Economopoulos 2023). QT grafts have also demonstrated good functional recovery in adolescent athletes, with significant post-operative improvements after a minimum of two years. Additionally, sex differences have also been implicated, with males experiencing longer sports careers than females after ACLR, regardless of graft type (Dadoo et al. 2024).Worth noting is the increase in contralateral ACL injury following RTS, where the rate of contralateral ACL injury was markedly higher in athletes who returned to sport (28%) compared to those who did not (4%), with females demonstrating both a higher contralateral injury rate (32% vs. 23% in males) and a higher revision surgery rate (12% vs. 7%) (Lindanger et al. 2019).
Biomechanical recovery may also vary by graft type as Mueske et al (Mueske et al. 2018) reported that adolescent athletes receiving QT, HT and BTB grafts exhibited greater symmetry in hip and knee flexion during drop-jump loading tasks than those receiving HT grafts, potentially contributing to faster and more stable return to athletic performance.
Functional recovery following anterior cruciate ligament reconstruction (ACLR) is commonly evaluated using patient-reported outcome measures such as the Lysholm Knee Score and the IKDC and MARX activity score. Across various studies, Lysholm scores tend to reflect high levels of postoperative satisfaction and function in both bone–patellar tendon–bone (BTB) and quadriceps tendon (QT) autografts, though some differences emerge based on timing and surgical context. Evidently Lysholm scores would be significantly lower in revision ACLR cases compared to primary reconstructions, highlighting the compounded challenges of repeat surgeries. In contrast, there was no significant difference between graft types, with a median Lysholm score of 95 observed in both BTB and QT groups scores generally classified as “excellent” (Perez et al. 2019). Even though reports showed slightly higher Lysholm scores in the QT group during short-term follow-up (6 to 12 months), this difference diminished over time, with long-term outcomes averaging similarly across both grafts (Li, Gu, and Wei 2020). These findings were echoed in meta-analyses (Brinkman, Tummala, and Economopoulos 2023) (McGuinness and Higgins 2020) where both found no statistically significant difference in Lysholm scores between BTB and QT autografts, further supporting the conclusion that both graft options offer comparable functional recovery in the long term.
When it comes to the Patient-reported outcomes using the International Knee Documentation Committee (IKDC) scores, both bone–patellar tendon–bone (BTB) and quadriceps tendon (QT) grafts show favorable profiles in current literature. Across multiple studies, scores consistently fall within the “good” to “excellent” range with a median Lysholm score of 95 for both graft types, suggesting uniformly high functional outcomes (Perez et al. 2019). Mild short-term increase in Lysholm scores with QT grafts between 6 to 12 months postoperatively, but the long-term scores equalized between QT and BPTB, averaging around 94.8 (Li, Gu, and Wei 2020). In terms of operative IKDC scores, significant improvements from preoperative to postoperative values were observed across multiple studies, a statistically significant increase in IKDC scores from a mean of 54.8 ± 17.5 to 86.2 ± 3.5 post-surgery was reported. Among adolescent athletes, the postoperative IKDC score reached 88.5 compared to a baseline of 37.5, highlighting substantial gains in perceived knee function (Dadoo et al. 2024). Brinkman et al (Li, Gu, and Wei 2020) also reported higher early follow-up IKDC scores with QT grafts (71) compared to BTB (61), though long-term follow-up showed no significant difference, with both groups reaching similar mean scores of approximately 94.8. These long-term findings were supported by other meta-analyses (Renfree et al. 2023b) (Brinkman, Tummala, and Economopoulos 2023) which reported comparable IKDC outcomes for QT and BPTB grafts over extended follow-up periods
Our findings also support the increasing interest in QT grafts and suggest they may provide similar effectiveness to BPTB grafts, without a higher risk of failure or functional impairment. The small number of available comparative studies (n=3) and modest total sample size limit statistical power and widen confidence intervals, particularly for graft failure. However, these conclusions must be interpreted with caution due to several limitations. Only three studies met the strict inclusion criteria due to the limited availability of comparative data in athletic populations. Of these, two of the included studies were observational in design and subject to increased risk of bias and confounding, while the lone randomized controlled trial (RCT) was rated as having “some concerns” regarding risk of bias. Moreover, the low event rate, particularly for graft failure, led to imprecise estimates with wide confidence intervals and reduced statistical power.
Additionally, the small number of studies also precluded a formal assessment of publication bias, and subgroup analyses could not be performed. Furthermore, while all included studies defined athletes as competitive or high-demand individuals, heterogeneity in athletic level and sport specificity may still introduce variability in outcomes. We chose not to broaden inclusion to hamstring autografts, as doing so would introduce biomechanical and clinical heterogeneity inconsistent with our focused comparison of QT versus BPTB in athletes.
Despite these limitations, this review has several strengths. It adhered to PRISMA guidelines, implemented a rigorous risk of bias and GRADE assessment, and a comprehensive search strategy, and included only studies with a minimum of two years follow-up. The exclusive focus on athletes addresses a critical gap in the literature and enhances the clinical applicability of findings to this high-performance population.
In conclusion, QT and BPTB autografts demonstrate comparable clinical and functional outcomes in athletes undergoing ACLR. Given the lower donor site morbidity associated with QT and the comparable efficacy observed in this analysis, QT may represent a valid alternative for athletes, particularly for patients concerned with anterior knee symptoms. As the included studies did not distinguish between soft-tissue QT and bone-block QT constructs, subtype-specific conclusions could not be drawn. Future high-quality, sport-specific randomized controlled trials with larger sample sizes are needed to validate these findings and support individualized graft selection in athletic practice.
Funding
The authors declare that no financial support was received for this study.
Competing interests
The authors declare no competing interests
Author contributions (CRediT)
-
Conceptualisation: Paula Salazar Mendoza (PSM)
-
Methodology: PSM, Emre Adalier (EA), Thierry Grimm (TG), Jakub Kaszyński (JK), Frank Lartey (FL), Diego José Lopes de Lima (DJLL)
-
Investigation/Data collection: PSM, EA, TG, JK, FL, DJLL
-
Data curation: PSM, EA, TG, JK, FL, DJLL
-
Formal analysis: PSM, EA, TG, JK, FL, DJLL
-
Writing—original draft: PSM, EA, TG, JK, FL, DJLL
-
Writing—review & editing: PSM, EA, TG, JK, FL, DJLL
-
Supervision: DJLL
-
Guarantor: DJLL
-
Corresponding author: EA