Introduction
Popularity of the reverse total shoulder arthroplasty (rTSA) continues to increase each year as an option to correct end-stage degenerative glenohumeral arthritis or irreparable rotator cuff arthropathies. In the US from 2016 to 2020, the percentage of rTSA increased from 14,781 (55%) to 20,590 (70%) of all primary shoulder arthroplasties (Mayfield et al. 2023). The technique was first described by Paul Grammont in 1985 using a 155º humeral inclination design with the goal of medializing the center of rotation and distalizing the humerus to increase deltoid muscle recruitment and restore active forward flexion (Boileau et al. 2005). However, this technique failed to improve active external rotation and often resulted in scapular notching (Bacle et al. 2017; Boileau et al. 2011; Ladermann et al. 2020; Mizuno et al. 2012). More recently, several authors demonstrated that lateralizing the glenoid component and utilization of a more anatomic 135º humeral inclination results in better external rotation and subsequently less scapular notching (Gutierrez et al. 2008; Katz et al. 2016; Ladermann et al. 2020). Although this design eliminated several common problems, overall rTSA still results in post-operative complications, most notably prosthesis dislocation, instability, and glenoid baseplate failure (Gerber et al. 2018; Hermena and Rednam 2024). Therefore, optimizing implant position is a critical component to minimize these complications and improve clinical outcomes and range of motion.
There is conflicting evidence regarding the extent to which radiographic measurements, such as the LSA and DSA, reliably predict clinical outcomes following reverse total shoulder arthroplasty. Boutsiadis et al. found that lateralization shoulder angle (LSA) and distalization shoulder angle (DSA) were determinants of clinical outcomes following rTSA. They reported that a LSA range between 70-95º was correlated with better active external rotation (R2 = 0.553, P < .001) and a DSA range between 40-60º was correlated with better forward flexion (R2 = 0.4, P < .001) (Boutsiadis et al. 2018). However, Mahendraraj et al. demonstrated that these measurements, although highly reproducible, might only have marginal correlation with post-operative patient-reported outcomes and no correlation with range of motion (Mahendraraj et al. 2020). Additionally, Imiolczyk et al. performed a retrospective study on 630 patients undergoing rTSA for cuff tear arthropathy (CTA) using multiple neck-shaft angles and showed no association between LSA and DSA and two-year functional outcomes (Imiolczyk et al. 2024). Jointly, these studies suggest that different patients may achieve different clinical outcomes despite having identical radiographic measurements (Bernal et al. 2021; Berthold et al. 2021; Mahendraraj et al. 2020).
Although several studies do suggest that implant positioning plays a role in post-operative outcomes and complications, many other factors likely contribute to the overall success of a patient’s recovery (Berhouet, Garaud, and Favard 2014; Li et al. 2013). Literature addressing this multifactorial nature of recovery following rTSA remains limited. One study attempted to address this by directly comparing patients with satisfactory versus poor post-operative anterior elevation and evaluating corresponding radiographic parameters. Jeon et al. found that post-operative lateral humeral offset was the only factor distinguishing the two groups, suggesting that small variations in implant positioning may meaningfully influence motion recovery (Jeon and Rhee 2018).
Since clinical outcomes are often multifactorial and contingent upon not easily controlled for patient-related factors, such as prior level of function, adherence to PT, unforeseen co-morbidities, and overall patient grit, controllable factors are limited to pre-operative planning and intraoperative implant positioning. This implication poses a challenge for study designs that seek to correlate positive and negative clinical outcomes with radiographic measurements, ultimately leading to inconsistent results and a lack of consensus. To address this challenge, we propose an approach that focuses on the “high achieving” outliers. By observing only patients who achieved excellent post-operative range of motion, we eliminate the negative influence of patient-related factors on post-operative outcomes and can more closely examine the role of implant positioning. These patients’ outcomes were not hindered by uncontrollable factors unique to each individual; instead, all possessed the minimum capabilities necessary to achieve maximal recovery. This method allows correlation between pre- and post-operative implant positioning with the goal of identifying reproducible measurements that will give patients the best chance for maximizing range of motion.
The purpose of this study was to identify pre- and post-operative radiographic measurements in patients who achieved excellent range of motion to optimize implant positioning in patients undergoing rTSA. We hypothesized that restoring the lateral humeral offset to closely align with the patient’s pre-operative anatomy, along with achieving optimal lateralization and distalization shoulder angles as outlined in the literature, will correlate with excellent clinical outcomes.
Material and Methods
Study Design
We retrospectively studied a consecutive series of all patients who received rTSA for the treatment of end-stage degenerative glenohumeral arthritis or irreparable rotator cuff arthropathies from 2021-2023. Data collection and study design were approved by our institutional review board. Of the original cohort, patients who met excellent range of motion criteria were eligible for inclusion. Excellent range of motion was defined as exceeding active forward flexion ≥ 170º and active external rotation > 60º at 6 months post-operation. Patients with a history of prior shoulder surgery, fracture, or infection and patients who underwent revision from anatomic total shoulder arthroplasty to rTSA or concurrent bilateral shoulder operations were excluded.
Surgical Technique
All surgeries were performed by a shoulder and elbow surgery fellowship-trained surgeon as an outpatient surgery either at a hospital or at an outpatient surgery center. Surgeries were performed either using the lateralized implant (Tornier Perform) or medialized implant (Zimmer TM). Because the senior author routinely selects between these systems based on patient-specific anatomy, component sizing, and inherent implant stability, both cohorts were included to ensure that observed radiographic and clinical patterns were assessed across the heterogeneity that reflects real-world practice. No computerized or navigation-based guides were used. All procedures were performed utilizing the standard deltopectoral approach with tenotomy of the subscapularis tendon. The humerus in all cases was prepared according to standard operative technique for each specific system. The glenoid was also prepared according to standard technique for each of the two shoulder arthroplasty systems implemented. The subscapularis tendon was repaired in each case using ethibond sutures in a figure of 8 suture technique.
All patients received the same post-operative rehabilitation instructions. Patients were placed in a simple shoulder sling for four weeks. Passive range of motion exercises were permitted on the first day post-operative. Active range of motion related to daily functions was encouraged post-operative as pain permitted. All patients were permitted to return to full activity (i.e. sport, weightlifting, manual labor) at 6 months post-operative.
Radiographic measurements
All patients received pre- and post-operative full-length anteroposterior radiographs, y view, and axillary. Two independent viewers performed radiographic assessment on the standard anteroposterior (AP) view. Pre-operative measurements included acromiohumeral interval (AHI) and lateral humeral offset (LHO). Post-operative measurements included AHI, LHO, lateralization shoulder angle (LSA), distalization shoulder angle (DSA), and spinospheric angle.
AHI was measured as the perpendicular distance between the most lateral portion of the undersurface of the acromion and a line parallel to the superior border of the greater tuberosity (Jeon and Rhee 2018). The change in humeral distalization (∆ AHI) was determined by subtracting the pre-operative AHI distance from the post-operative AHI distance (Figure 5). LHO was measured as the distance from the AHI line to the most lateral projection of the greater tuberosity (Jeon and Rhee 2018). The change in humeral lateralization (∆ LHO) was determined by subtracting the pre-operative LHO distance from the post-operative LHO distance (Figure 6). LSA was determined by drawing a line from the superior glenoid tubercle and the most lateral border of the acromion and a second line from the most lateral border of the acromion to the most lateral border of the greater tuberosity. The angle formed between these two lines was defined as LSA (Boutsiadis et al. 2018). DSA was determined by drawing a line from the most lateral border of the acromion to the superior glenoid tubercle and a second line from superior glenoid tubercle to the most superior border of the greater tuberosity. The angle formed between these two lines was defined as the DSA (Boutsiadis et al. 2018) (Figure 7). The spinospheric angle (glenoid inclination) was determined as the angle between the floor of the supraspinatus fossa and the glenoid fossa (Maurer et al. 2012).
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics 29.0.1.1 (SPSS Inc., Armonk, NY, United States). Continuous data were reported as mean, standard deviation, and range and categoric data reported as percentage. Pre- and post-operative radiographic measurements were compared using the paired student t-test and the medialized and lateralized components were compared using the independent student t-test with significance set at p < 0.05 and a 95% confidence interval (CI). Inter-rater reliability was determined by calculating the intraclass correlation coefficient (ICC).
Results
Patient characteristics
A total of 425 rTSAs were performed during the study period. Of those, 392 did not meet excellent range of motion criteria (<170º of forward flexion or <60º of external rotation) at 6 months post-operative. Of the 33 shoulders that met the range of motion criteria, six were excluded, leaving 27 shoulders in 26 patients for inclusion (Figure 1). The mean age of the patient was 68.2 ± 7.0 years (range 50 – 78). The study group consisted of 14 women and 13 men (Table 1).
Inter-rater reliability
The inter-rater reliability was calculated for LSA, DSA, pre- and post-operative AHI, pre- and post-operative LHO, and spinospheric angle. The reliability was found to be in excellent agreement (ICC > 0.90) for every radiographic measure. Post-operatively, the LSA averaged 88º and the DSA 43º. The combined mean LSA + DSA measured 131.9 ± 8.5º (Table 2).
Medialized inlay vs. lateralized inlay
Comparing the medialized (n = 13) and lateralized (n = 14) inlays, the only significant difference found was that the post-operative LHO was significantly higher in the lateralized inlay group (65.6 ± 4.6 mm vs. 55.2 ± 3.1 mm, p < .001). Although not significant, there was a notable difference in post-operative AHI, with the medialized inlay displaying a mean of 26.3 ± 5.5 mm and the lateralized inlay displaying a mean of 31.1 ± 7 mm (p = .058) (Table 3).
Pre- to post-operative change in LHO and AHI
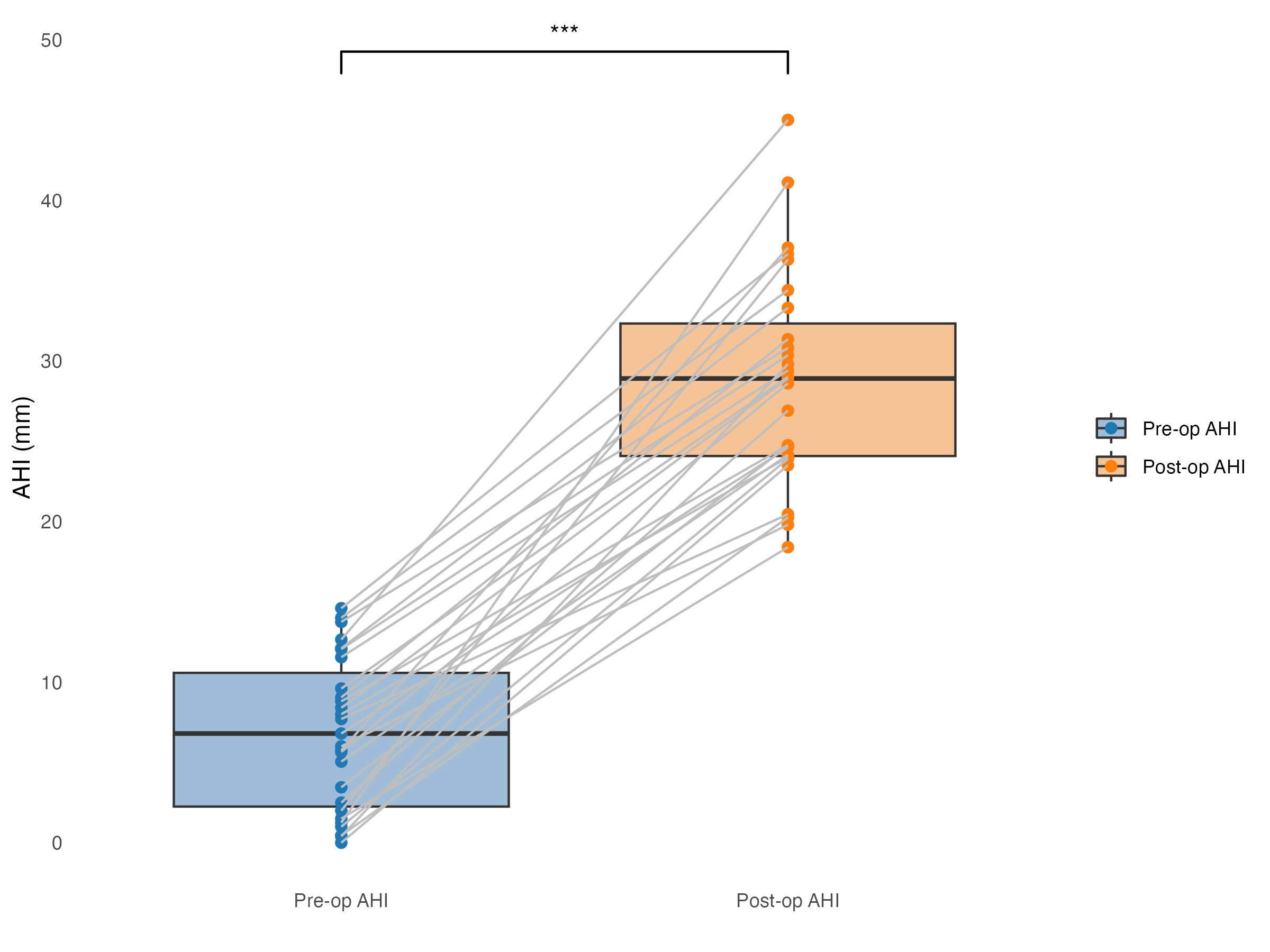
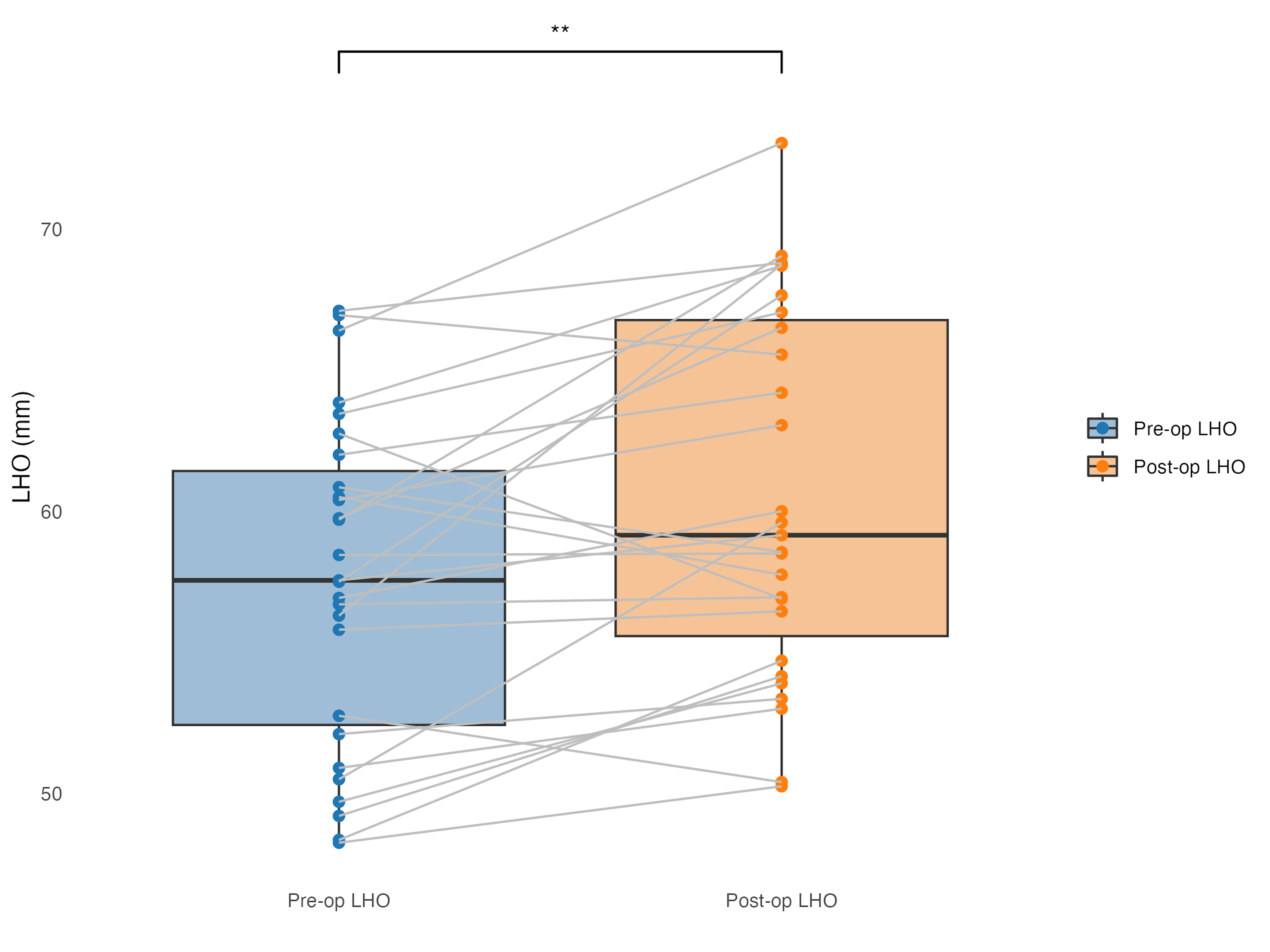
There was a significant increase in AHI from 6.8 mm pre-operatively to 28.8 mm post-operatively, with a mean change of 22.0 ± 6.4 mm (p < .001) (Figure 2). The LHO displayed a small increase from 57.5 mm pre-operatively to 60.6 mm post-operatively, with a mean change of 3.1 ± 4.4 mm (p < .001) (Figure 3). The range of the change in LHO was 5.85 mm medialized to 12.45 mm lateralized compared to the patients’ pre-operative measurement. Of those, 81% (n = 22) were lateralized and 19% (n = 5) were medialized (Figure 4).
.png)
.png)
Discussion
The results of this study demonstrate that patients who achieved excellent post-operative range of motion and underwent rTSA for end-stage degenerative glenohumeral arthritis or irreparable rotator cuff arthropathy had restoration of their pre-operative lateral humeral offset. Furthermore, the mean post-operative LSA and DSA measurements were within ranges for optimal clinical outcomes as defined in the literature (Boutsiadis et al. 2018; Valenti et al. 2024). Our findings suggest that reproducing the patient’s anatomy while preserving LSA and DSA measurements is closely associated with excellent range of motion, offering a valuable framework for guiding pre-operative implant positioning.
In a recent study, Imiolczyk et al (Imiolczyk et al. 2024). investigated the prognostic value of LSA and DSA measurements on a cohort of 630 patients with cuff tear arthropathy following rTSA. They used linear and parabolic regression analyses to attempt to correlate these measurements with patient reported outcomes (Subjective Shoulder Value and Constant Score) and range of motion (anterior forward elevation and external rotation) following implantation using four different neck shaft angles. Notably, they did not find that the two angles directly correlated with 2-year range of motion (ROM) or functional outcomes in any implant design. Also, they noted that the optimal range values of the LSA (75-95º) and DSA (40-65º) defined by Boutsiadis et al. did not fully match the means resulted in their study (Boutsiadis et al. 2018). Imiolczyk et al. concluded that LSA and DSA are reproducible measurements to estimate implant positioning, but their value as prognostic factors remains yet to be proven. Despite notable strengths, including a large sample size and a homogeneous cohort, this study – like several other cohort comparison studies – does not consider the patient-related factors that, while challenging to control, play an influential role in post-operative outcomes. These confounding factors may be contributing to the discrepancies found between Boutsiadis et al., Imiolczyk et al., and several other studies that fail to reach a consensus (Berthold et al. 2021; Boutsiadis et al. 2018; Imiolczyk et al. 2024; Mahendraraj et al. 2020; Valenti et al. 2024).
The unique approach adopted in our study contributes a valuable perspective to the ongoing discussion on optimizing implant positioning and assessing the prognostic value of radiographic measurements following rTSA. Psychosocial factors, such as lifestyle, resilience, adherence to post-operative rehabilitation, pre-operative baseline ROM, and pain tolerance, significantly influence post-operative recovery and ultimately impact surgical outcomes (Mavros et al. 2011; Pignay-Demaria et al. 2003; Rosenberger, Jokl, and Ickovics 2006; Weinerman et al. 2023). While it might be presumed that these factors impact each cohort uniformly within a single study, this assumption falters when comparing studies with distinct patient demographics and inherent selection biases. These patient-specific variabilities complicate the ability to draw meaningful conclusions from small radiographic discrepancies to guide implant positioning. While our outlier approach, focusing on patients who achieved excellent outcomes, cannot replace a true comparative cohort, it offers a meaningful way to reduce the influence of patient-specific variability and to highlight radiographic patterns that may be relevant to post-operative function.
The post-operative mean LSA and DSA measurements found in our study fall within ranges suggested by several studies to correlate with improved range of motion and patient-reported outcomes. Our results demonstrate that patients with an excellent range of motion 6 months post-operatively had a mean LSA of 88.9 ± 6.8º and DSA of 43.0 ± 9º (Table 2). Boutsiadis et al. found that a LSA between 75º and 95º predicted better active external rotation (R [Berhouet, Garaud, and Favard 2014] = 0.553, P < .001) while a DSA between 40º and 60º predicted better active anterior elevation (R [Berhouet, Garaud, and Favard 2014] = 0.4, P < .001) and a DSA between 45º and 65º predicted the highest abduction (Boutsiadis et al. 2018). One possible explanation as to why LSA measurements between 75º and 95º may optimize active external rotation is that it more closely restores the anatomic center of rotation of the subscapularis and teres minor muscles, allowing maintained muscle tension throughout active rotation (Greiner et al. 2013).
More recently, Valenti et al (Valenti et al. 2024). also reported a correlation between specific LSA and DSA measurements and improved patient-reported outcomes. They compared the LSA and DSA measurements of patients with a 1-year post-operative American Shoulder and Elbow Surgeons Standardized score (ASES) > 76 with those of patients scoring < 76 following rTSA. Patients with an ASES score > 76 displayed a mean LSA of 86.4 ± 11.4º and a mean DSA of 48.6 ± 12.4º, whereas patients with an ASES score < 76 displayed a mean LSA of 100.1 ± 7.6º and a mean DSA of 37.8 ± 9.8º. Additionally, the LSA had an IQR of 79.5 – 93.5 and DSA had an IQR of 39.5º – 57.5º. Our means closely align with those reported and fall within the interquartile range reported by Valenti et al (Valenti et al. 2024).
Our study found an average change in the acromiohumeral interval (AHI) of 22.0 ± 6.4 mm, a reflection of the total distalization following implantation, aligning closely with prior studies investigating humeral position and arm length (Figure 2). One of the main goals of rTSA is to maximize deltoid tension and improve the patient’s active anterior elevation (AAE) by lowering the humerus relative to the acromion (Boileau et al. 2005). Jobin et al. reported an average acromiohumeral difference of 23 ± 9 mm, with patients having intervals > 23 mm associated with improved active anterior elevation (Jobin et al. 2012). However, Schwartz et al. reported an average increase between the acromion and the greater tuberosity to be 18.9 mm but found no association with improved ROM (Schwartz et al. 2014). Several other studies used bilateral scaled radiographs to measure the same distance. Markedly, Werner et al. improved AAE with arm’s lengthened between 1 cm and 2.5 cm, but worsened AAE > 2.5 cm (Jobin et al. 2012). In our cohort, patients with excellent ROM had a mean AHI of 22 mm, which aligns with prior studies reporting average acromiohumeral intervals of approximately 2 cm without exceeding 2.5 cm.
In line with our hypothesis, patients who achieved excellent post-operative range of motion predominantly had restoration of their lateral humeral offset toward native position. The average change in lateral humeral offset (LHO) was 3.1± 4.4 mm overall, with the medialized inlay being slightly less at 1.93 ± 3.5 mm and the lateralized inlay being 4.2 ± 4.9 mm (P = .219) (Figure 1). A recent study from Charles et al (Charles et al. 2024). looked at post-operative strength and range of motion in 30 patients receiving rTSA to correlate changes in LHO using computed tomography. While absolute post-operative LHO was associated with increased strength, they found that a pre- to post-operative change of > 5 mm in LHO was associated with decreased strength, and patients with LHO measurements equal to or slightly less than their anatomic position demonstrated greater strength and ROM. Although our results demonstrate a small increase in LHO compared to pre-operative position (+3.1 mm, P < .001), 74% (n = 20) of the patients had a LHO change < 5 mm and of those patients, 25% (n = 5) were slightly medialized, with post-operative LHO less than pre-operative (Figure 4). These findings, taken in the context of current literature, support the theory proposed by Oh et al. that replicating a patient’s native anatomy despite the nonanatomic nature of rTSA might allow for optimal ROM (Oh et al. 2020). With respect to our findings, limiting the amount of LHO to 3 mm might allow for optimal external rotation and forward flexion by maintaining muscle tension throughout the motion.
One potential drawback to using the LSA and DSA is that they do not differentiate how much of the lateralization and distalization is attributable to the glenoid and the humerus. Instead, they describe the “global” lateralization and distalization which could oversimplify unique differences in anatomy between patients. Thus, Schippers et al. recently proposed a new method to characterize these discrepancies by further splitting LSA and DSA into two new angles with respect to the glenoid and humerus (Schippers et al. 2024). This method would allow further analysis into patient-specific anatomical differences in glenoid and humeral position. Future studies investigating postoperative outcomes of patients utilizing glenoid versus humeral lateralization angles is warranted.
The primary strength of this study lies in its unique approach to minimizing patient-specific factors that are challenging to control while relating radiographic measurements of rTSA implant positioning with excellent range of motion outcomes. However, our findings must be considered in the context of the study’s limitations. This is a retrospective analysis conducted on a small patient population, primarily due to the stringent criteria set to define “excellent” range of motion. By focusing exclusively on high-performing outliers, we acknowledge the potential for selection bias, likely resulting in a cohort that is healthier than the broader rTSA population. Importantly, the study lacks a control group with negative outcomes, which prevents us from making definitive comparisons or correlations; however, this decision aligns with our methodology, which was designed to minimize the confounding effects inherent to the complex recovery process. As such, our findings should be interpreted as associative rather than correlative or causal.
Finally, we did not evaluate patient-reported outcomes; future studies could continue these findings by assessing patient perspectives on recovery through long-term follow-up. Additionally, future studies comparing patients with excellent versus poor range of motion could evaluate implant positioning and account for social factors to identify potential correlations. While our study was not intended to establish descriptive measurements for preoperative planning, future research could explore how the radiographic patterns identified here might be integrated into 3D planning platforms to support surgical decision-making. Comparative cohorts will be essential to determine which measurements most reliably differentiate functional outcomes and could therefore inform adjustments to version, inclination, or lateralization. Additional prospective work using navigation systems may help translate these relationships into practical intraoperative guidance.
Conclusion
In patients who achieved excellent range of motion following rTSA, the lateral humeral offset was restored very closely to pre-operative anatomy, the lateralization and distalization shoulder angles were also restored within optimal ranges defined in the literature, and the acromiohumeral interval was distalized by an average of 22 mm. This study demonstrates that post-operative restoration of lateral humeral offset to pre-operative measurements is correlated with excellent post-operative outcomes.
Figure Legend
Figure 1. Inclusion criteria
Figure 2. Pre-op vs. post-op AHI (*** p < .001)
Figure 3. Pre-op vs. Post-op LHO (** p < .001)
Figure 4. Degree and direction of LHO change
Figure 5. Acromiohumeral interval preoperative (top) vs. postoperative (bottom)
Figure 6. Lateral humeral offset preoperative (top) vs. postoperative (bottom)
Figure 7. Lateralization shoulder angle (left) and distalization shoulder angle (right)