
INTRODUCTION
Revisions for total knee arthroplasty (rTKA) and total hip arthroplasty (rTHA) are often complicated by extensive bone loss, distorted anatomical landmarks, and the technical challenges of prior surgeries (MacAskill et al. 2022, 2024; Wu et al. 2023; Ngim et al. 2023; Steelman, Carlson, and Ketner 2021; Zhang et al. 2022). While computer navigated (CN) technology, with or without robotics, has become increasingly popular in the primary total joint arthroplasty (TJA) setting, its use in revision procedures remains nascent and relatively understudied (MacAskill et al. 2024; Wu et al. 2023; Ngim et al. 2023; Steelman, Carlson, and Ketner 2021; Cochrane, Kim, Stauffer, et al. 2024; Andriollo et al. 2024).
CN systems used in revision TJA (rTJA) include active and semi-active platforms, which rely on preoperative imaging and/or intraoperative mapping to guide component placement (MacAskill et al. 2024; Wu et al. 2023; Cochrane, Kim, Stauffer, et al. 2024). Computed Tomography (CT)-based systems create patient-specific 3-dimensional models for surgical planning, while imageless systems register anatomy intraoperatively using joint surface or kinetic data (MacAskill et al. 2024; Zhang et al. 2022; Cochrane, Kim, Stauffer, et al. 2024; Tuecking et al. 2021). These platforms can provide real-time feedback on component sizing, component positioning, screw trajectories, knee gap balancing, and impingement free joint range of motion, potentially aiding in the reproducible execution of the preoperative plan (MacAskill et al. 2024; Wu et al. 2023; Ngim et al. 2023; Zhang et al. 2022; Cochrane, Kim, Stauffer, et al. 2024).
Despite these capabilities, CN use in rTJA faces several challenges. When CT planning is required by the particular technology, existing implants may introduce metal artifacts that compromise CT imaging and registration accuracy (MacAskill et al. 2022, 2024; Wu et al. 2023; Ngim et al. 2023). Bone loss and distorted landmarks can further complicate registration (MacAskill et al. 2024; Wu et al. 2023; Ngim et al. 2023). Additionally, current CN software is primarily approved for primary arthroplasty, making its use in revision surgery off-label (MacAskill et al. 2022; Wu et al. 2023; Steelman, Carlson, and Ketner 2021; Kalavrytinos et al. 2020). As such, adoption remains limited, and concerns persist regarding cost, training burden, and uncertain long-term benefit (MacAskill et al. 2022, 2024; Wu et al. 2023; Ngim et al. 2023; Cochrane, Kim, Stauffer, et al. 2024).
Nevertheless, CN systems have shown early promise in managing complex revision cases, such as rTHA with severe acetabular defects and rTKA requiring precise component realignment (MacAskill et al. 2024; Wu et al. 2023; Steelman, Carlson, and Ketner 2021; Zhang et al. 2022; Tuecking et al. 2021; Dretakis, Raptis, and Koutserimpas 2024). However, evidence remains limited and primarily consists of early or short-term outcomes (Wu et al. 2023; Cochrane, Kim, Stauffer, et al. 2024). Further research is needed to assess whether the technical advantages of CN rTJA translate into improved implant survivorship and patient satisfaction (MacAskill et al. 2022, 2024; Wu et al. 2023; Ngim et al. 2023). The purpose of this study is to assess national trends in the utilization of CN rTHA and rTKA using a large claims database and evaluate 2-year complication rates between patients undergoing CN versus conventional revision procedures.
METHODS
Study Design
This retrospective cohort study used the PearlDiver (PearlDiver Technologies, Colorado Springs, CO, USA) Mariner170 dataset. The Mariner dataset has over 170 million U.S. patients covered under commercial insurance, Medicare, Medicaid, government insurance, and self-pay between 2010 and 2023. Patient records were retrieved using procedural and diagnostic codes from the International Classification of Diseases Ninth (ICD-9) and Tenth (ICD-10) Revision, and Current Procedural Terminology (CPT). Institutional review board approval was waived since the dataset has been de-identified for public access.
Study Population
Patients were included in this study if they were (i) over the age of 18 years, (ii) underwent rTKA (CPT-27486, CPT-27487) or rTHA (CPT-27134, CPT-27137, CPT-27138), and (iii) had 2-year follow-up available. Patients with a history of infection, trauma, tumor, or metastases were excluded. Eligible patients were subsequently stratified by conventional or CN procedures using ICD (ICD-9: 00.31-39, 17.41-43; ICD-10: 8E0Y codes) and CPT codes (CPT-20985, CPT-0054T, CPT-0055T), and case-control matched 1:1 by age, sex, Charlson Comorbidity Index (CCI), diabetes, obesity, and tobacco use history. Case control matching was used to ensure statistical equivalence in confounding variables across the two cohorts. Covariates were selected based on their documented impact on outcomes of interest, with CCI encompassing a broad range of comorbidities, thus allowing for equivalent comorbidity burden across cohorts.
Patient Demographics
In total, 1,676 CN and 171,591 conventional rTKA and rTHA patients were included, with a mean age of 65 years, 59% female sex, and a mean CCI of 1.8. CN rTJA patients were younger (CN = 63 years, Conventional = 65 years), had a lower mean CCI (1.5 vs 1.8), and had lower rates of diabetes (35% vs 42%) (all p<0.001) (Table 1). In addition, they less commonly underwent revision for periprosthetic fracture (2% vs 6%), prosthetic joint infection (10% vs 15%), and instability/dislocation (13% vs 15%) (all p<0.01) (Table 2).
After case-control matching, 1,292 patients remained in each group with no significant differences in baseline demographics or comorbidities. Their mean age was 63.6 years, sex 60% were female, mean CCI was 1.2, 33% had diabetes, 18% had obesity, and 40% had tobacco use history (all p=1.000), thus confirming successful cohort balancing (Table 1).
Data Extraction
The following outcomes were observed for all patients: demographics, revision etiology, and 2-year complications. Revision etiology included aseptic loosening, implant failure, periprosthetic fracture, periprosthetic osteolysis, periprosthetic joint infection (PJI), instability or dislocation, bearing wear, and other mechanical complications. Two-year complications analyzed included aseptic loosening, implant failure, periprosthetic fracture, periprosthetic osteolysis, PJI, instability or dislocation, bearing wear, and other mechanical complications.
Statistical Analyses
Postoperative complications were compared using chi-square tests across CN and conventional rTJA patients before and after stratification. All analyses were conducted using the built-in R statistical software within PearlDiver and using SPSS Statistics for Windows, Version 29.0 (IBM Corp, Armonk, NY), with a p <0.05 indicating statistical significance.
RESULTS
Computer-Navigated Epidemiology
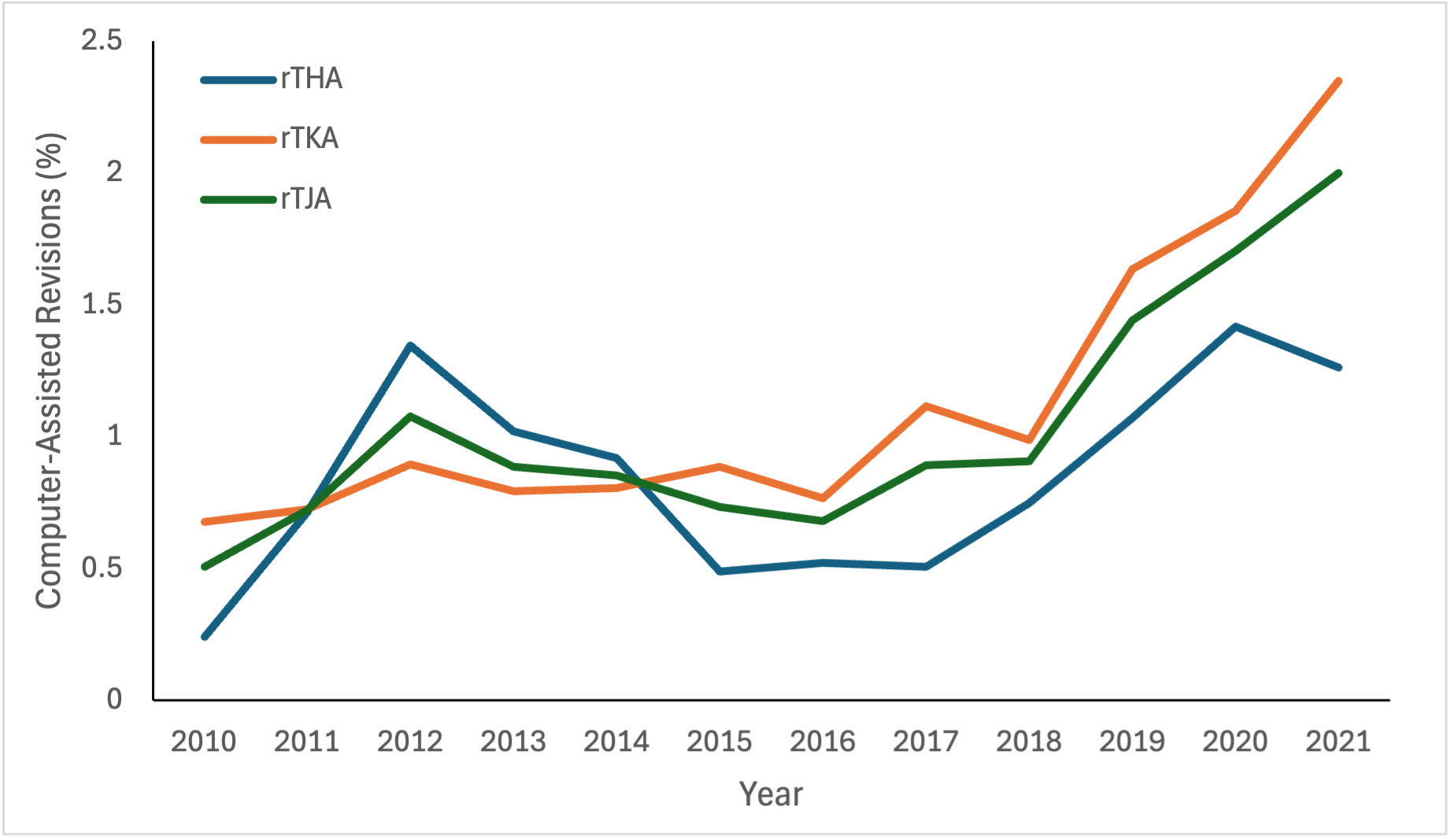
Over the study period from 2010 to 2021, utilization of CN techniques in rTJA steadily increased from 0.5% of revision procedures in 2010 to 2.0% by 2021, corresponding to a more than 250% relative increase in usage. Notably, the increase in utilization was more pronounced for rTKA, where CN cases rose from 0.7% to 2.4% of all rTKAs between 2010 and 2021, compared to a more modest increase from 0.2% to 1.3% of all rTHA (Figure 1).
Complications
Analysis of 2-year complications demonstrated no significant differences between CN and conventional approaches. Within the rTKA cohort, rates of aseptic loosening were 2.0% in the CN group versus 2.7% in the conventional group (p=0.347). Rates of dislocation were 2.0% vs 1.9% (p=1.000), periprosthetic fractures were 0.9% vs 0.2% (p=0.114), and re-revision were 8.9% vs 8.7% (p=0.958), respectively. Likewise, within the rTHA cohort, CN and conventional approaches yielded comparable rates of aseptic loosening (2.2% vs 1.3%, p=0.299), dislocation (1.9% vs 4.0%, p=0.202), periprosthetic fracture (1.6% vs 1.6%, p=1.000), and re-revision (11.1% vs 10.9%, p=0.835) (Table 3).
DISCUSSION
This national insurance claims study evaluated utilization trends and 2-year complications following CN versus conventional rTJA. Our findings demonstrate that while CN revision procedures remain infrequent, their utilization has steadily increased over the past decade. Moreover, rates of mid-term complications, including aseptic loosening, dislocation, periprosthetic fracture, and re-revision, were comparable between CN and conventional rTHA and rTKA cohorts. These results suggest that CN technology may be safely employed in the revision setting without altering patients’ postoperative course. Still, further research remains to be conducted to evaluate the utility of CN rTJA in improving longitudinal outcomes and cost efficacy in lieu of manual revision arthroplasty.
Prior literature on CN revision arthroplasty is limited and consists largely of case reports, surgical technique papers, and small cohort studies. Nevertheless, these early studies have proposed potential advantages of CN assistance in complex revision scenarios, including improved alignment, optimized component positioning, and preservation of bone stock (MacAskill et al. 2022, 2024; Wu et al. 2023; Ngim et al. 2023; Steelman, Carlson, and Ketner 2021; Zhang et al. 2022; Tuecking et al. 2021; Kalavrytinos et al. 2020; Dretakis, Raptis, and Koutserimpas 2024). For instance, Sharma et al. reported reduced postoperative dislocation rates following rTHA, which they attributed to the more accurate placement of hip components, particularly the acetabular cup, facilitated by computer navigation. The authors suggest this improved accuracy was believed to mitigate common causes of instability, including impingement, edge loading, and component malalignment (MacAskill et al. 2024). In contrast, our large national analysis found no significant differences in implant survivorship or failure rates at two years between CN-assisted and conventional rTHA.
Despite these results, CN revision procedures account for less than 3% of all revision arthroplasties in the United States. Most CN platforms were initially designed for primary arthroplasty and are used off-label in the revision setting, which can limit their availability and integration. Furthermore, preoperative imaging artifacts from retained hardware, distorted anatomy, and the need for flexible intraoperative decision-making may make CN use technically challenging in revision cases (MacAskill et al. 2022, 2024; Wu et al. 2023; Ngim et al. 2023; Cochrane, Kim, Stauffer, et al. 2024). A notable learning curve remains with CN utilization, which may gradually flatten as exposure increases among newer generations of trainees, thus helping to demystify the technology and potentially accelerating its adoption in complex revision scenarios (LeRoy et al. 2023; Duensing et al. 2023).
Importantly, however, several CN and robotic systems are now either FDA-approved or in the process of gaining on-label indications for use in revision arthroplasty, expanding their potential applicability beyond the traditionally off-label domain. Modern platforms allow not only improved planning but also robotic-arm–guided bony resection, which can be particularly advantageous in cases with severe bone loss, distorted anatomy, or retained hardware. CT-based systems create high-resolution 3D reconstructions of host bone and residual implant morphology, enabling more precise planning of component orientation, leg length, offset restoration, and screw trajectories in the revision setting. Similarly, robotic-arm execution may help surgeons achieve intended implant positioning even when conventional anatomical landmarks are absent or unreliable. These technical benefits may make CN more useful in challenging revisions, including severe bone defects (e.g., Paprosky III acetabular defects) or cases with abnormal joint line, ligament imbalance, or prior malpositioned components.
Of note, these nuances may not be captured in large administrative datasets. Because database studies lack operative details, defect grading, fixation strategies, bone loss classification, and surgeon decision-making, they cannot account for the fact that CN is frequently reserved for cases of greater complexity. Thus, similar complication rates between CN and conventional cohorts in our study may actually reflect a positive signal: CN-assisted cases, despite presumably greater complexity, did not demonstrate worse outcomes. This limitation underscores that our findings should not be interpreted as evidence that CN provides no benefit in revisions; rather, the observed equivalence should be contextualized within the likely selection bias toward more difficult cases in the CN cohort.
Cost considerations also play an important role in CN utilization. CN and robotic systems involve substantial capital investment, maintenance costs, and disposable instrumentation fees, and reimbursement structures do not currently incentivize their use in the revision setting. Given that payers and institutions may scrutinize cost-effectiveness, our finding of similar mid-term complication rates could be misinterpreted to argue against the necessity of CN in revisions and potentially influence surgeon reimbursement or coverage policy. However, cost-effectiveness analyses must consider surgical complexity, alignment accuracy, long-term implant survivorship, and downstream expenditures related to instability, component malposition, or repeat revisions, factors that cannot be assessed within the limitations of our dataset.
This study has several potential limitations that should be considered. First, as a retrospective analysis, the study remains susceptible to selection bias, and important confounding variables such as surgeon experience, hospital volume, and intraoperative decision-making could not be controlled. Second, as noted by the lower CCI following matching, higher-risk patients were selected out for the analysis which may limit the generalizability of our results. Third, due to coding limitations, we could not stratify by CN type. This generalization of what is otherwise a vast group of assistive technologies should not be overlooked or be used to justify the use of any one CN system in practice based off these findings. Fourth, the database lacked patient-reported outcomes, functional scores, operative time, and radiographic measures such as alignment or implant positioning. Finally, the absence of long-term follow-up beyond two years may underestimate differences in implant survivorship and durability over time.
CONCLUSION
In summary, Computer-Navigated rTHA and rTKA have increased in use nationwide, but adoption remains low overall. Computer Navigation assistance was associated with comparable mid-term outcomes compared to conventional techniques. Early adopters of off-label Computer Navigation in revision arthroplasty should consider their comfort with the technology and their technology’s limitations with planning and registration before proceeding in lieu of manual revision arthroplasty. While these mid-term results suggest the safe and selective use of Computer Navigated systems in revision arthroplasty, further prospective research is needed to define their long-term clinical value and cost-effectiveness.
FUNDING DECLARATION
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.