


Introduction
Anterior inferior shoulder instability when complicated by glenoid bone loss remains a challenging problem for patients and surgeons alike. Recurrent instability negatively affects patient quality of life, often necessitating complex surgical stabilization, and lost productivity in vocational and athletic endeavors. Many surgical techniques to restore glenoid bone loss have been employed historically, but currently coracoid transfer (Latarjet) and free bone block (FBB) procedures are popular choices for addressing these difficult problems due to the unacceptably high failure rates in arthroscopic soft tissue based procedures.
Arthroscopic and open enhancements of labral repair, including remplissage, dynamic anterior stabilization and labral scaffolds, have yielded promising results without utilizing bone augmentation (Keeling et al. 2023). In cases of subcritical glenoid bone loss among non-collision athletes undergoing primary stabilization, arthroscopic and open Bankart repair with remplissage remain effective treatment options; the addition of remplissage may decrease recurrent instability from 30% to 9.6% (Woodmass et al. 2024). Nonetheless, numerous studies have demonstrated inferior results of soft tissue stabilization when greater than 20-25% of glenoid bone loss is present (Shin et al. 2016). Some authors support bony procedures, such as Latarjet or FBB, with bone loss as low as 13.5% (Dickens et al. 2017). Other indications include revisions following failure of primary soft tissue repair, high Instability Severity Index Scores (ISIS), and involvement in high-contact or collision sports. The Latarjet has a long-standing history of successful stabilization and involves the transfer of the coracoid process with an attached conjoint tendon. Conversely, FBB procedures anatomically reconstruct the glenoid defect and emphasize preservation of native soft tissues and anatomic relationships. What is clear, however, is that appropriate surgical management with bony augmentation in the setting of significant bone loss remains paramount to reduce recurrent glenohumeral instability and posttraumatic osteoarthritis (Dickens et al. 2017; Leroux et al. 2014).
This review will compare the benefits of open Latarjet versus arthroscopic FBB procedures in the athlete with respect to surgical efficiency, complications and efficacy. This review will focus on the current state of knowledge, highlight areas of contention, and provide an overview for clinicians navigating the decision on how best to address glenoid bone loss.
The Role for Open Latarjet
The Latarjet technique has been lauded as the gold standard for conferring shoulder stability via Patte’s proposed triple blocking effect. First, the coracoid autograft recreates the anterior arc of the glenoid (osseous blocking). Second, the rerouted conjoint tendon tensions the subscapularis, creating a sling, which provides soft tissue stability in external rotation and abduction (musculotendinous blocking). Finally, repair of the anterior capsule and inferior glenohumeral ligaments aids in stability by mimicking a capsulolabral repair (capsulolabral blocking).
Yamamoto et al. demonstrated restoration of translational force to the intact-condition level after Latarjet in cadaveric biomechanical studies (Yamamoto et al. 2013). The triple blocking effect was validated with the sling effect and anterior capsular repair conferring 77% and 23% of stability, respectively, in end-range arm position. In mid-range arm position, the sling effect and glenoid cavity reconstruction contributed 51% to 62% and 38% to 49% of stability, respectively. These findings are further supported by Giles et al. who showed that the dynamic sling effect prevented dislocations in 100% of specimens compared to 75% of specimens without the sling effect (Giles et al. 2013). Despite these biomechanical advantages, the clinical benefit of the sling has been challenged in a recent meta-analysis. (Hao et al. 2025).
After open Latarjet procedures, recurrent instability and dislocation rates remain below 10%, underscoring the effective restoration of shoulder stability (Hurley, Jamal, et al. 2019; Mizuno et al. 2014). Furthermore, postoperative Rowe and SANE scores are reported to approach 90 (Hurley, Lim Fat, et al. 2019; Mizuno et al. 2014). However, long term follow up studies have identified a risk of development or progression of osteoarthritis in approximately 23% of patients (Mizuno et al. 2014). Despite reports suggesting a reduction in external rotation, Smith et al. observed postoperative restoration of range of motion in all directions in as early as six months, when compared to both the ipsilateral and contralateral shoulder (Smith et al. 2024).
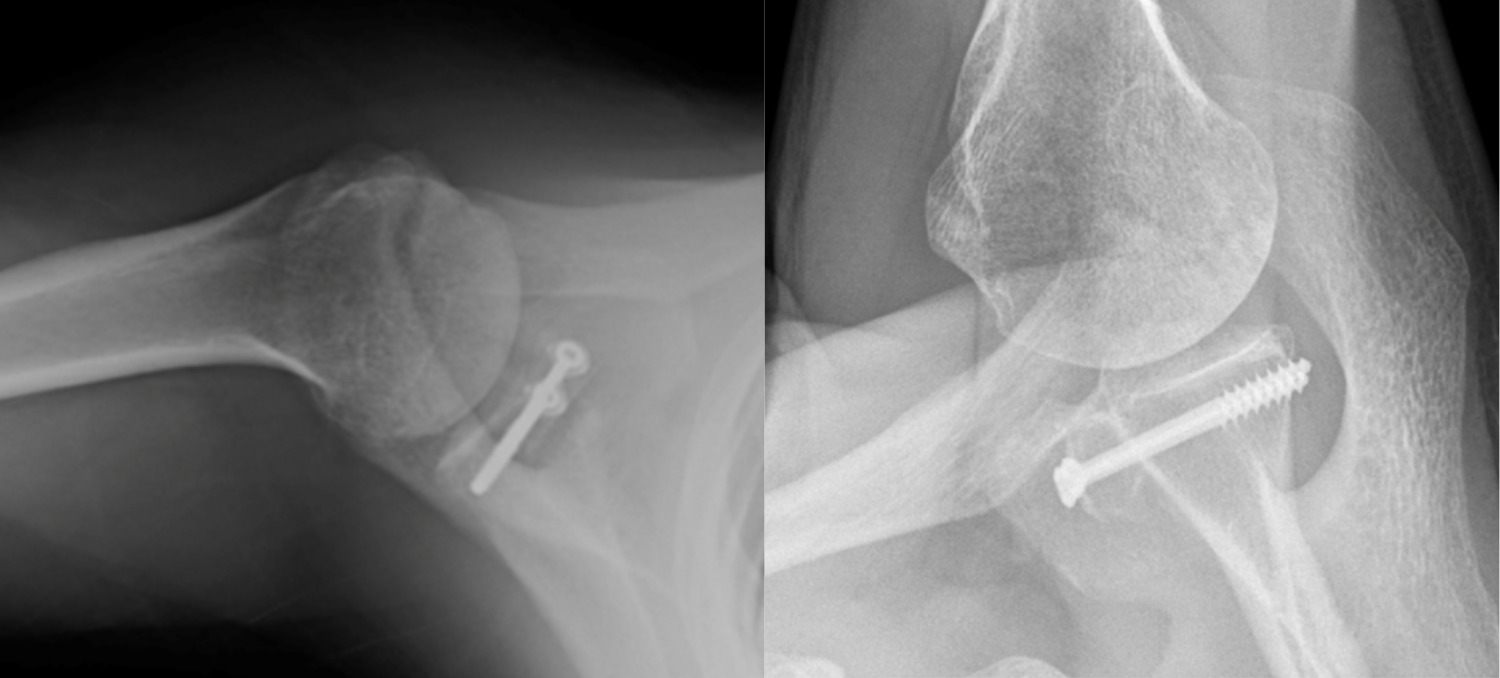
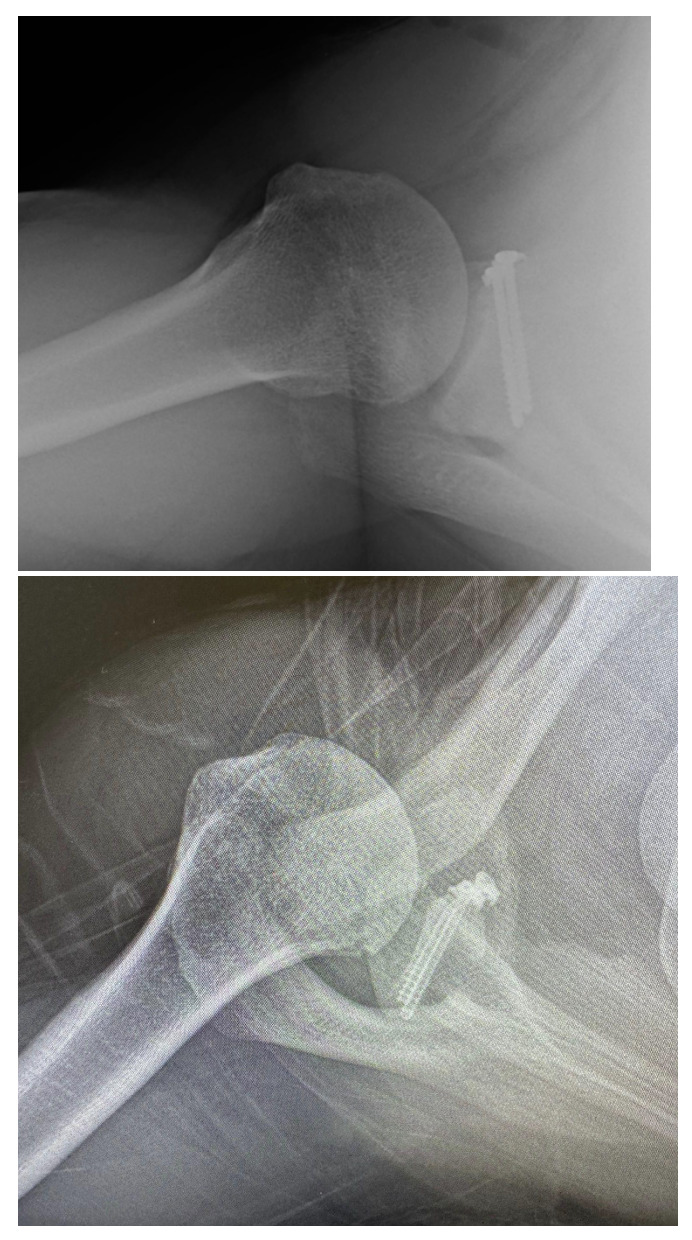
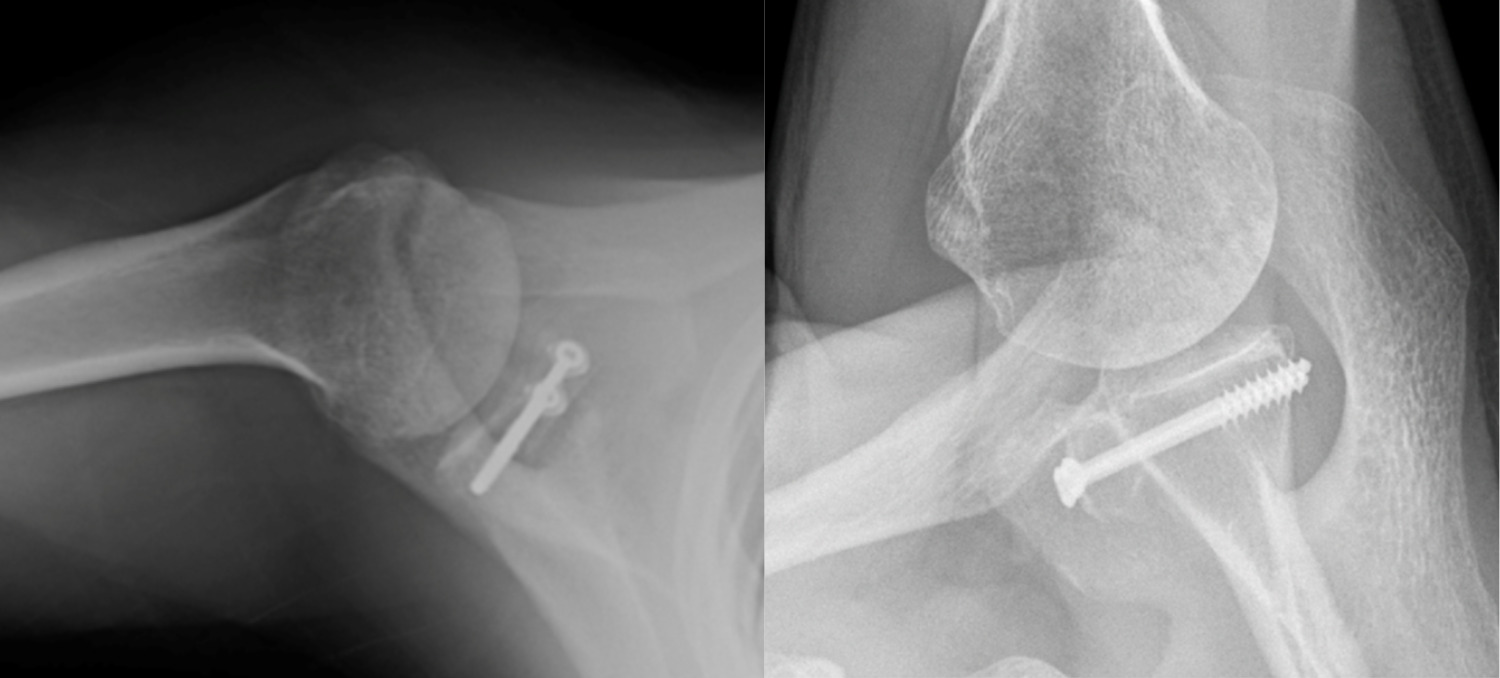
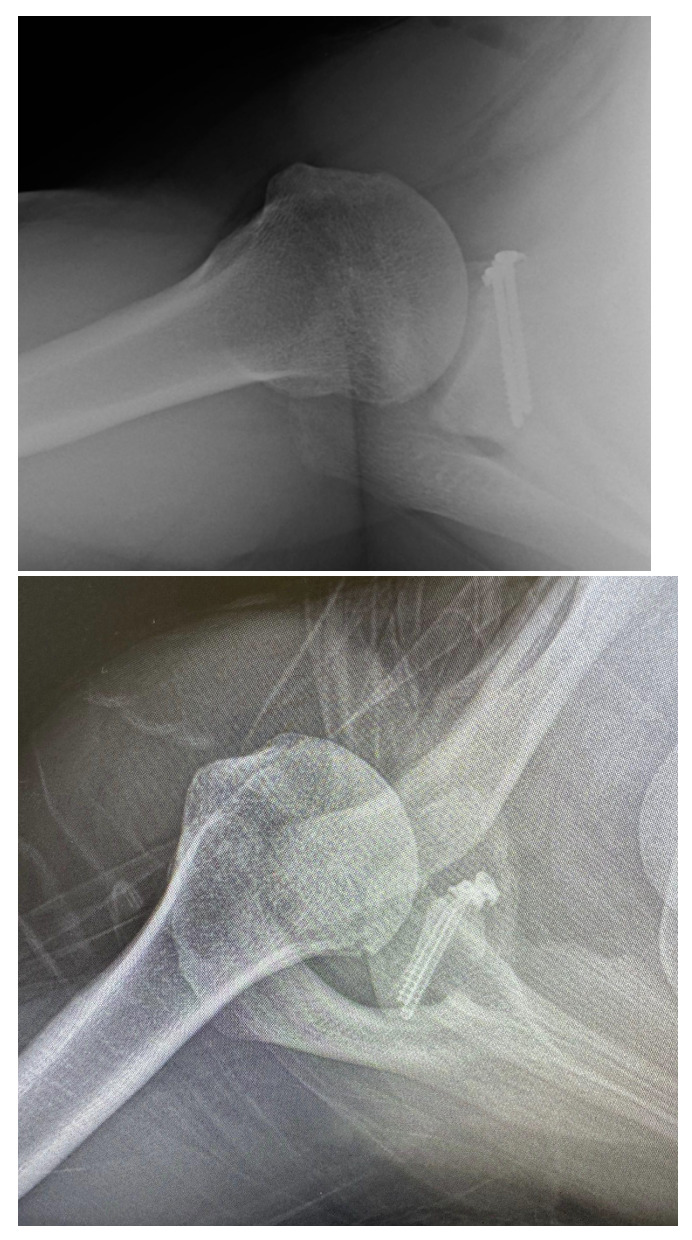
Success of the Latarjet may be predicated on surgical technique. Screw and graft placement are vital components of successful glenoid reconstruction. The ideal screw positioning is perpendicular to the anterior wall of the glenoid and parallel to the joint line (Figure 1). Screws should be placed at an alpha angle less than or equal to 10° to avoid suprascapular nerve injury and minimize graft displacement (Lädermann et al. 2012; Hsu et al. 2022). Improper screw orientation can negatively affect graft healing, cause neurovascular complications, and increase symptomatic hardware rates (Figure 2). Malpositioned screws can increase the rate of screw removal due to loosening caused by oblique compression between graft and glenoid. Medially oriented screws typically have poorer purchase due to the thinner posterior glenoid cortex. Additionally, superior and medial screws have an increased likelihood of causing suprascapular nerve palsy (Maquieira et al. 2007). Accurate graft positioning is also crucial, with the ideal placement being 1.5-3 mm lateral to the flush position. Excessive medialization increases the risk of recurrent instability. Excessive lateralization elevates contact pressure between the glenoid and humeral head, increasing the risk of osteoarthritis (Martins et al. 2022). Additionally, bone grafts placed at 4 o’clock on the anteroinferior glenoid rim reduce displacement in external rotation and anterior translation (Nourissat et al. 2014).
Long term subscapularis function remains another theoretical concern after the Latarjet procedure. One study utilized magnetic resonance imaging (MRI) to evaluate subscapularis functional integrity with a mean follow up of approximately eight years and demonstrated no evidence of partial or full thickness tears. Additionally, negative belly-press and lift off tests demonstrated no decrease in internal rotation strength after eight years (Azizi et al. 2022). Both Caubere et al. and Azizi et al. demonstrated no fatty infiltration of the subscapularis at one year and eight years, respectively (Caubère et al. 2017; Azizi et al. 2022). These studies suggest that despite the subscapularis split performed during surgery, range of motion, function and muscular integrity of the tendon are preserved.
Prior to shoulder stabilization surgery, many patients identify the ability to return to sport as their greatest concern (Warth et al. 2013). A systematic review of open Latarjet with ten year follow-up reported a return to sport rate of 85%, with 76% returning to preinjury level (Hurley, Jamal, et al. 2019). When comparing outcomes between competitive and recreational athletes, Rowe scores significantly increased in competitive athletes after open Latarjet (Baverel et al. 2018). Overhead athletes have successful outcomes after Latarjet, with 73% of European handball players reporting no pain while throwing and returning to ball training and competitive play at 3.2 and 4.9 months, respectively (Bauer et al. 2024). A separate study of non-overhead athletes found no difference in throwing velocity or distance following open Latarjet when compared to a control group. Although external rotation at the side was reduced in this study, external rotation at 90° abduction remained unaffected, likely explaining the preservation of throwing ability (Yokoi et al. 2024).
Open Latarjet has however been associated with longer operative times, higher minor and major complications and an increased risk for return to the OR when compared to standard arthroscopic Bankart techniques. Other authors have attempted to define the learning curve and time to surgical proficiency for the procedure. Operative time decreased significantly after the first 15 cases and plateaued after 30 cases in this single surgeon series (Papalia et al. 2024). Complications, while high at nearly 11%, do not appear to be affected by hospital or surgeon volume in some large studies (Alkaduhimi et al. 2023).
The success of the Latarjet procedure relies on precise execution of the surgical technique, specifically accurate screw and graft placement, which ensures stable fixation, minimized complications, and reduced recurrent instability. In addition to low rates of persistent glenohumeral instability, this procedure yields excellent clinical outcomes, including a restored range of motion. When performed with meticulous attention to screw and graft positioning, the open Latarjet continues to serve as a reliable option for restoring shoulder stabilization and returning to sport in a timely manner.
While the Latarjet remains the gold standard for managing shoulder instability with glenoid bone deficiency, there remains a 10-15% complication rate (Athwal et al. 2016; Domos et al. 2018). The complication risk and relatively long learning curve highlights the need to assess other stabilization options. FBB procedures, although lacking the benefit of the sling effect, may confer joint stability without anatomical alteration associated with conjoint transfer and may help reduce the complication risks of Latarjet reconstruction. Arthroscopic Latarjet deserves mention as an effective alternative to open Latarjet, with theoretically lower complications. A full discussion of this goes beyond the scope of this article. Nonetheless, North American adoption of the arthroscopic technique has lagged due to the technical difficulties for surgeons without a high volume of this procedure (Hurley, Lim Fat, et al. 2019).
Arthroscopic Free Bone Block Procedures
The first described FBB procedure was reported in 1918 with an iliac crest autograft (Eden 1918). Several autograft options have since been described, including scapular spine, distal clavicle and hardware-free sculpted grafts (Xiang et al. 2021; Auffarth et al. 2008). In 2008, Provencher popularized use of fresh distal tibial allografts (DTA) as an alternative to autografts (Menendez et al. 2023; Provencher et al. 2009). In 2015, Wong described the use of an arthroscopic osteochondral FBB to manage glenoid bone deficiency (Wong and Urquhart 2015). Currently, FBB graft options include fresh or frozen DTA or distal radius allografts.
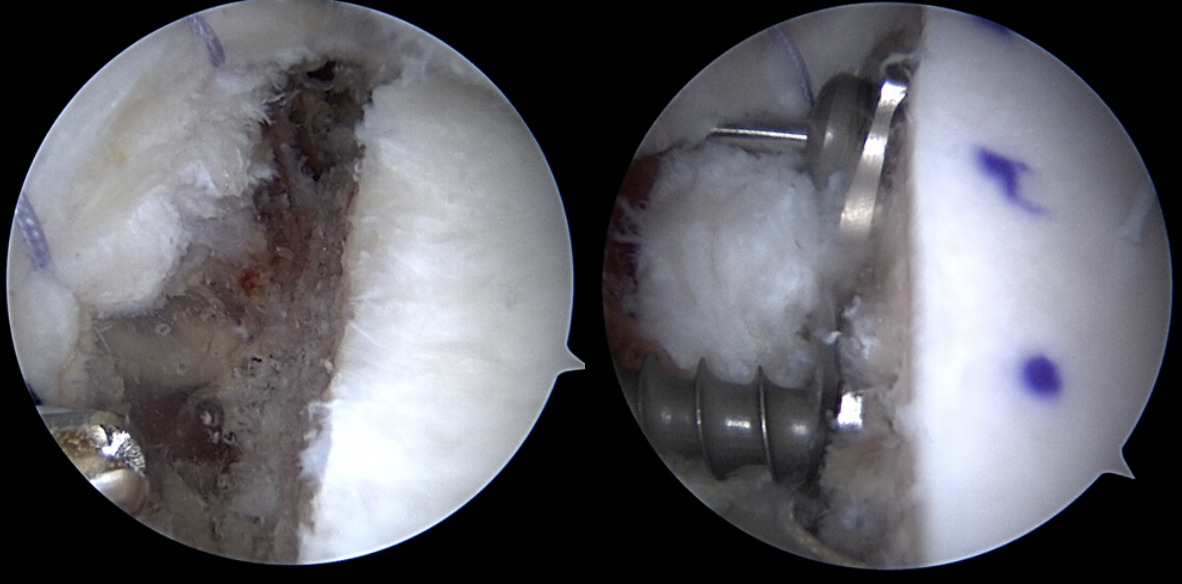
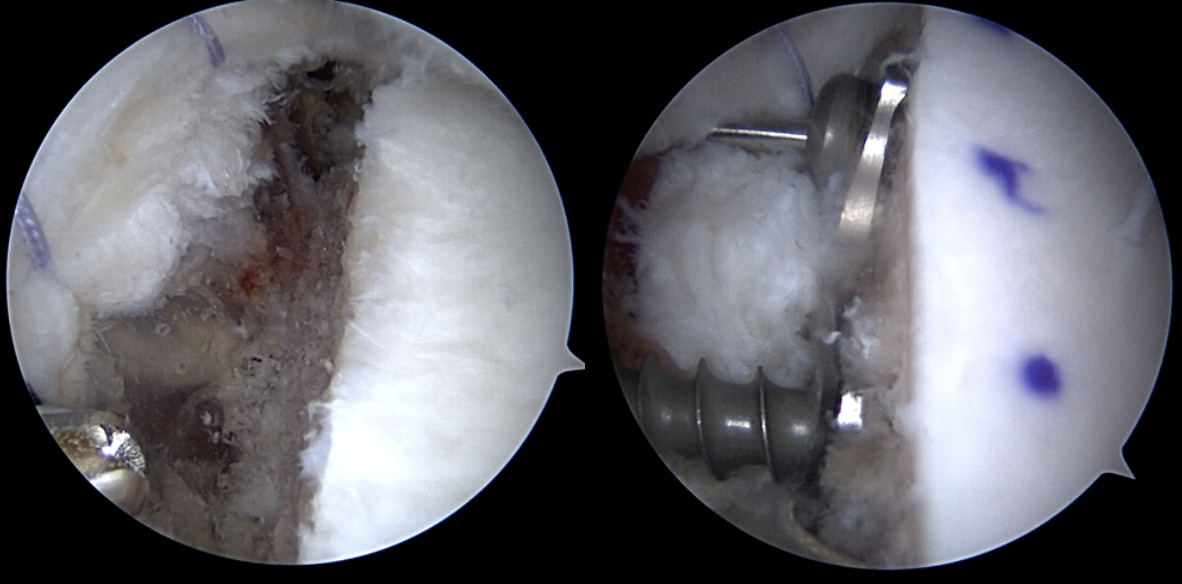
Arthroscopic FBBs serve as an alternative to traditional Latarjet with both theoretical and practical advantages. Proponents of arthroscopy contend that the articular surface visualization and graft placement are improved compared to its open counterpart. Furthermore, sling procedures are non anatomical and may complicate future surgery (Figure 3) (Lafosse et al. 2010). The relevance of graft position is critical, as 1 mm of graft lateralization can lead to poorer outcomes (Ernstbrunner et al. 2023). Avoiding harvest of the coracoid minimizes the risk of neurovascular injury as well as intraoperative coracoid fracture. Additionally, the use of osteochondral allografts removes prior size limitations given the fixed size of the coracoid autograft. Finally, the shape and contour of the DTA may provide a more anatomic match with the native glenoid (Provencher et al. 2009).
Comparison
The results of open Latarjet and arthroscopic FBB both yield satisfactory outcomes, with a recurrent instability rate of less than 10% (Hurley, Lim Fat, et al. 2019). In comparison studies, both Frank et al. and Gilat et al. found no significant difference in recurrent instability rates between Latarjet and FBB procedures (Frank et al. 2018; Gilat and Haunschild et al. 2021).
Graft incorporation is slower in FBB, with allografts requiring approximately 6.9 months versus Latarjet autografts requiring 6-12 weeks (Dawe et al. 2025; Kordasiewicz et al. 2019). While achieving bony union of the glenoid bone block may not be absolutely required for clinical success, a malunited, nonunited, or overly resorbed bone block may contribute to recurrent instability, pain or hardware complications. While both graft types experience resorption, the degree of resorption is substantially higher in FBB (Wong et al. 2018; Delgado et al. 2024). Excessive resorption may contribute to screw prominence and consequent hardware-related complications. Despite resorption of ≥50%, one study reported patients can still achieve excellent clinical outcomes, suggesting that such resorption levels are not consistently associated with poor outcomes or increased rates of revision surgeries (Wong et al. 2020).
Fixation of the graft is typically achieved with screws, buttons or cerclage fixation. A systematic review of arthroscopic versus open Latarjet stabilization with attention to hardware complications demonstrated a higher rate of screw removal in the arthroscopic group (Lacouture-Suarez et al. 2023). When comparing open Latarjet screws and arthroscopic buttons, Nascimento et al. found comparable clinical and radiological outcomes; however, a letter to the editor highlighted that 16% of the button group had postoperative complications (primarily neurologic injury) compared to 2% in the screw group (Nascimento et al. 2025; Lädermann 2025). Similarly, Pancura et al. compared button and screw fixation in arthroscopic FBB and found that patients who underwent button fixation were significantly more likely to suffer from recurrent dislocations. Over 40 percent of the button group in the study had recurrent dislocations versus zero dislocations in the screw group with one of the conclusions cautioning against using buttons in allograft FBB (Pancura et al. 2025).
Graft and screw positioning after open and arthroscopic Latarjet have been analyzed using computed tomography (CT) imaging. Neyton et al. performed a retrospective multicenter study demonstrating a significantly lower mean angulation in both superior and inferior screws in the open group versus the arthroscopic group. Graft positioning also differed between each technique on both axial and sagittal views. In the axial plane, arthroscopic grafts were placed significantly more laterally. In the sagittal plane, the open group showed more reliable placement of grafts below the equator (Neyton et al. 2018). These findings are corroborated by Marion et al. who noted more lateral and inferior graft placement in arthroscopic Latarjet when compared to the open technique (Marion et al. 2017). While these previously mentioned studies are from arthroscopic Latarjet, and not FBB studies, certain similarities may be drawn. This highlights the technical challenges of graft position and fixation in the arthroscopic techniques.
Arthroscopic bone restoration of the glenoid is technically demanding and can be difficult to master. Multiple studies have demonstrated a substantial improvement in proficiency and corresponding decrease in operative time for arthroscopic Latarjet and DTA from an initial range of 103 to 183 minutes to a range of 76 to 95 minutes after 20-45 arthroscopic procedures (Leuzinger et al. 2019; Cunningham et al. 2016; Bishai et al. 2022; Moga et al. 2018; Castricini et al. 2013; Kany et al. 2016; Getz and Joyce 2020; Ekhtiari et al. 2018). A multisurgeon, large volume analysis showed achievement of an operative time steady state after 30-50 cases (Valsamis et al. 2020). However, Zhu et al. observed that, regardless of surgical experience, arthroscopic Latarjet remained 30 to 40 minutes longer than the open approach (Zhu et al. 2017). Arthroscopic FBB techniques are less frequently described in the literature, but may be associated with a faster learning curve, as the procedure may be comparatively easier to perform. Surgeons who endeavor to perform arthroscopic glenoid bone procedures may consider this when their operative case load (15-30 per year) supports the time commitment to the associated learning curve.
When choosing between open Latarjet and arthroscopic FBB other important considerations include cost and graft procurement. The open Latarjet provides a zero-cost bone block compared to the thousands of dollars associated with fresh or frozen DTA. Uffmann et al. performed a cost minimization analysis comparing DTA, open Latarjet, and arthroscopic Bankart repair. Open Latarjet was approximately 66% and 15% less costly than DTA and arthroscopic Bankart repair, respectively (Uffmann et al. 2019). In addition to cost, access to allograft bone in FBB procedures can pose logistical challenges, particularly in centers without an onsite bone bank. Autograft iliac crest, distal clavicle and scapular spine remain viable economical options. A more detailed analysis of total costs when taking recurrence, complications, and additional surgery are all considered, however, has not been performed to our knowledge.
Return to sport rates following arthroscopic FBB approach 80%, with most non-returning patients citing reasons such as reprioritization of work and life (Ojaghi et al. 2024). A systematic review showed a higher return to sport rate for FBB procedures for autografts than allografts in both open and arthroscopic procedures (Gilat et al. 2021). In a cohort of competitive collision or overhead athletes, open Latarjet demonstrated a faster return to sport (5.07 months), compared to the arthroscopic approach (5.87 months) (Abdul-Rassoul et al. 2019).
Conclusion
While the open Latarjet procedure remains a reliable surgical option for anteroinferior instability, FBB procedures present a compelling alternative. The Latarjet’s high historic success rate is appealing, especially for surgeons well-versed in the open approach, but is not without its challenges in terms of complications, learning curve and long-term alteration of anatomy. Consequently, arthroscopic FBB has become an attractive option, addressing many concerns with its subscapularis-sparing technique, lower neurovascular risk, and favorable learning curve for the arthroscopic surgeon. Long term follow up is not yet available. FBB procedures conserve patients’ anatomy, specifically the subscapularis and coracoid, which are relevant if and when additional reconstructive surgery may become necessary. Conversely, allograft bone is costly, has a longer return to sport, is subject to greater resorption and the arthroscopic technique is not without its challenges in graft positioning or fixation.
Ultimately, in the hands of a skilled surgeon, both techniques are safe and effective. As more long-term prospective data is collected, the specific indications for each will be refined.
Sethi Final Take

My instability patient population shapes my preference for the surgical procedures I offer. While many instability operations (remplissage, DAS) gain popularity, there remains to be a role for glenoid bone restoration in the young collision athletes and revision cases that make up my practice. I value the advantages of an all arthroscopic bone block, subscapularis sparing operation that does not alter the shoulder’s neurovascular anatomy. However, at this time, allograft bone procedures exhibit greater resorption and have higher failure rates when screw fixation is not used. Furthermore, a predictably faster return to sport, and the additional stability benefit conferred by the conjoint tendon make Latarjet my choice operation in the competitive collision athlete. As these gaps in recovery are inevitably narrowed, I imagine further adoption of the Arthroscopic Anatomic Glenoid Reconstruction (AAGR) techniques for the collision athlete.
Bishai Final Take

When treating patients with bone loss shoulder instability, the pathology often dictates the surgical treatment plan. Although the coracoid serves as a local graft with no cost, the amount of bone that can be made up for the glenoid may not be enough. In these cases the distal tibial allograft utilizing the AAGR technique is a great tool in the armamentarium. Secondly, the ability to maintain the remaining labrum and capsule to help augment the repair and attach it to the paleoglenoid helps with keeping the humeral head positioned more posterior as a secondary rein. The AAGR also maintains the integrity of the subscapularis which allows for decreased concerns of subscapularis failure for those doing open peels and tenotomies or even a split. These patients with shoulder instability with bone loss can be very difficult to treat therefore it is paramount to have the ability to stratify these patients into the correct treatment algorithm whether it be an autograft or allograft reconstruction with techniques like the Latarjet and AAGR respectively.
Alberta Final Take

Recurrent instability with bone loss remains one of the unsolved challenges in my practice. While it’s hard to argue with the long term results and success of Latarjet reconstruction (both published and personally experienced), there are limitations in terms of graft size and patient selection that remain. Reconstruction is limited to the width of the local coracoid graft in Latarjet and while that addition of the sling effect is beneficial, it is at the cost of severely altered anatomy which presents many future challenges. The return to sports in the highest level athletes also tends to dictate the procedure when all else is equal. Because the return to sport rates, recurrent dislocation rates and time to return to sports tend to favor open Latarjet in this group, that is typically my choice, especially in contact/collision athletes. In recreational athletes, laborers, seizure disorder patients, and those with defects too large to be reconstructed with the local coracoid, I favor AAGR with allograft. In either case, extreme attention to detail with accurate graft placement and solid fixation with screws is mandatory. In both procedures, what has become clear is that resorption is common, especially when the graft exceeds the native glenoid size and that does not necessarily affect clinical outcomes. Both procedures are highly effective at solving the recurrent instability problem which is the primary goal and it is up to us as surgeons to offer our patients the procedures we can reliably perform with their best interest in mind. And ultimately it is our responsibility to take advantage of all of the many learning tools available to us to become better for our patients.