Introduction
Hip fractures involving the proximal femur represent a significant and growing public health concern. These fractures predominantly affect the geriatric population, with incidence increasing two-fold each decade as patients age (Tosteson et al. 2007). They result in a multitude of severe consequences most notably by increasing mortality rates, especially within 1 year of fracture (Schnell et al. 2010). The impact of hip fractures extends beyond the immediate consequences of the injury, encompassing long-term reductions in mobility, independence, quality of life, and increased risk of subsequent fractures (De Joode et al. 2019).
Subsequently, the risk of sustaining a second fracture is increased particularly in patients who do not receive appropriate bone health evaluations and interventions post-fracture (Patel, Judge, Johansen, et al. 2024). There is a persistent increase in risk of subsequent fragility fractures over time in patients who do not receive appropriate osteoporosis management after their initial fracture as previous studies have reported rates of 7% at 1 year, 9% at 2 years, and 11.3% at 3 years (Bogoch, Marcano-Fernández, Schemitsch, et al. 2022; Dang, Zetumer, and Zhang 2019; LeBlanc, Muncie, and LeBlanc 2014). Studies have shown that patients who receive comprehensive bone health assessments and management, including dual-energy X-ray absorptiometry (DXA) scans and appropriate pharmacotherapy, have better outcomes in bone density and fracture prevention (Pflug et al. 2024).
The International Society for Clinical Densitometry (ISCD) and Bone Health and Osteoporosis Foundation (BHOF) recommend DXA scans for women aged 65 and older, men aged 70 and older, and those who have broken a bone after age 50 or who have other risk factors for bone health screening. Current barriers to care have revealed to be patient, physician and system based (Choksi et al. 2023). There are differences in reported barriers by physicians and patients, with physicians reporting barriers such as patient non-adherence and low priority (Launois, Cabout, Benamouzig, et al. 2022). On the contrary, patient reported barriers are lack of communication regarding the assessment or etiology of their fracture, and concerns related to cost of treatment (Office of the Surgeon General (US) 2004). Some barriers systematically affect men and race/ethnic minorities, where older white women are more likely to be viewed as at risk and subsequently more likely to be referred for evaluation (Barton, Behrend, and Carmouche 2019).
This study aims to determine the rate of referral completion for bone health evaluations in patients who experience fragility fractures of the hip to identify barriers for attending bone health evaluations. We also aim to explore potential correlations between patient demographic, surgical, or injury factors with likelihood to be referred for a bone health evaluation. By identifying patients most at risk for missed bone health evaluations following hip fractures, we can inform future clinical practices and improve the overall management of bone health by filling knowledge gaps within the healthcare system.
Methods
With institutional review board approval, this study used a retrospective cohort analysis, reviewing patients presenting with hip fractures at a Midwest Academic Level 1 Trauma Center at a University Hospital between January 1, 2019, and December 31, 2022. Eligible participants include individuals 65 years and over, who experienced hip fractures (femoral neck, intertrochanteric, or subtrochanteric fractures) with at least 6 months of follow-up. This age range was chosen due to the prevalence of hip-related fragility fracture in this population, which would justify bone density evaluation to determine risk for subsequent fracture. Exclusion criteria include pregnant patients and prisoners. There were 602 total patients reviewed. The data were extracted using the electronic medical record (EMR) system to access medical record numbers, visit dates, birth dates, surgery dates, medication lists, diagnosis codes, laboratory values (calcium, vitamin D), current smoking, referral information, and patient demographics. Patient demographics included age, zip code, insurance status (Medicare, uninsured, or commercial), sex (male/female), and marital status (married/single). Additionally, radiology procedures were reviewed, including DXA scans and bone density T-score. Mental health was categorized as psychiatric history listed in their intake form, which included a question related to anxiety, depression, and/or other mental health issues such as schizophrenia or dementia.
Visit completion was defined as patients referred to and attending bone health (BH) evaluation appointments. The BH Program is a Fracture Liaison Service (FLS) staffed by a team of doctors and advanced practice practitioners dedicated to evaluating, screening, diagnosing, treating, and educating patients about their bone health. All patients receiving treatment, including fixation/nail treatment or total hip arthroplasty, were assigned into 2 groups: referred (RF) or not referred (NR). Inpatient referrals were initiated postoperatively by the operative orthopedist or resident orthopedist, prior to discharge. The electronic medical record (EMR) system includes multiple pre-made order sets containing postoperative orders, which may or may not include a referral to the bone health program. However, referrals could also be entered separately as individual orders. The referred group was further subdivided into 2 groups: attendance (AT) and non-attendance (DNKA). Patients that were referred but did not establish an appointment, missed or no showed, or canceled the evaluation were assigned to the non-attendance group. This included telemedicine/remote evaluations, though most initial appointments are in person.
Statistical Analysis
The data was analyzed using various statistical tests depending on the nature of the data. A t-test was used for comparing means, while the chi-squared test and Fisher’s exact test were used to assess differences in categorical variables. The Shapiro-Wilk test was used to evaluate normality, and Bartlett’s test was used to assess homogeneity of variances. For non-parametric data, the Wilcoxon test was used.
To investigate the factors associated with BH referral, a multivariate logistic regression was conducted with factors found to be significant in the current study and in historical studies. A multivariate logistic regression was then conducted to examine factors associated with BH evaluation visit completion. For each model, a stepwise approach was used to identify relevant predictors, and coefficients were estimated for each independent variable. All variables were included in each model to control for potential confounding. Hosmer-Lemeshow goodness of fit (GOF) was used to assess the model’s fit to the data.
All analyses were performed using R Studio, with a significance level set at P < 0.05.
Results
Factors Associated with Successful Referral
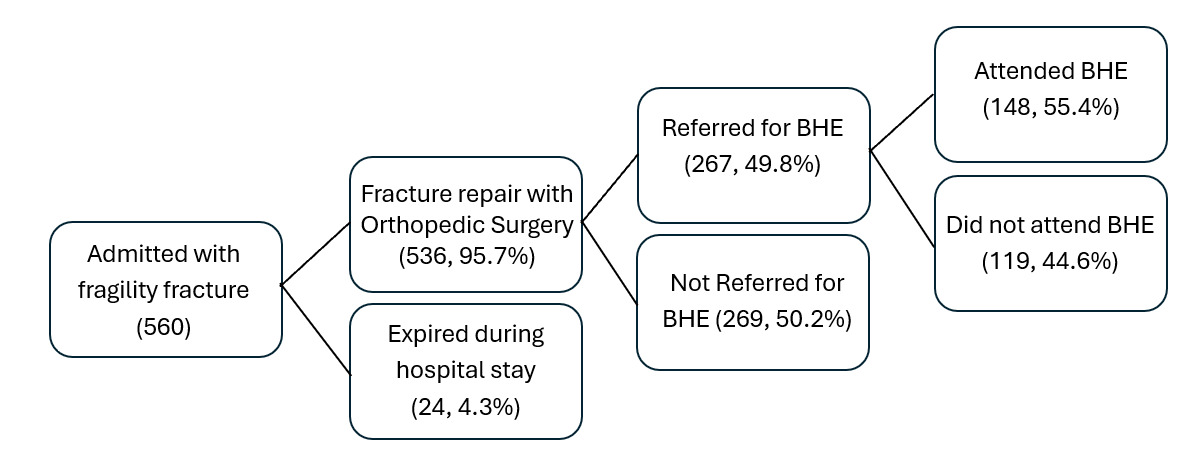
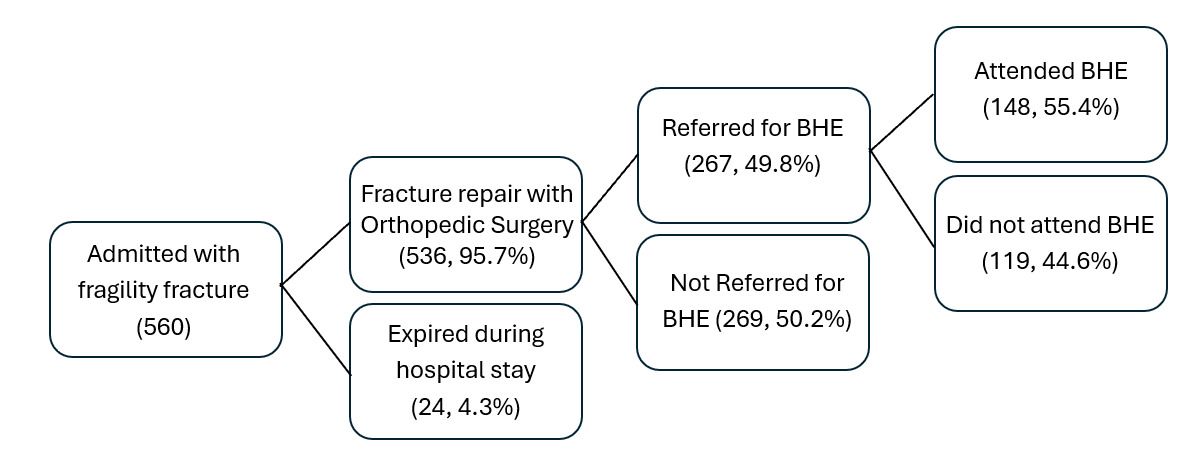
Out of the 560 patients initially assessed after hip fractures, 24 expired during their hospital stay, leaving 536 for this analysis (Figure 1). Referrals for bone health evaluations were made for 267 patients (49.8%), while 269 (50.2%) did not receive referrals. Marital status, age, and mental health history were not significantly different between groups as shown in Table 1. There was no difference in referral status based on patient sex (p=0.093).
Patients undergoing open reduction and internal fixation (ORIF) or nail treatment were referred at the same rate as those who received total or hemi hip arthroplasty (THA) (p=0.052). THA patients have 33% lower odds of being referred when all other factors are held constant. However, hip fracture type emerged as a significant indicator of referral to bone health evaluation (p=0.018).
Referred patients had a statistically shorter hospital stay, averaging 6.8 days compared to 7.7 days for those not referred (p=0.008). Neither smoking status nor readmission rate were significantly different. However, calcium levels were significantly higher in referred patients compared to non-referred patients (p=0.008), but no significant difference was seen based on Vitamin D levels.
In a multivariate analysis that included admission calcium levels, length of stay, age at encounter, and treatment, higher admission calcium levels were significantly associated with increased odds of referral (OR 1.3, p=.039), while undergoing THA was associated with decreased odds compared to ORIF (OR .68, p=.041). Length of stay and age at encounter were not significantly associated with referral. The Hosmer-Lemeshow goodness of fit test revealed an acceptable fit of the model (χ²=9.49, df=8, p=0.30).
Factors Associated with Visit Attendance
Out of the 267 people referred, 55.4% attended their initial bone health appointment. No significant difference was found for appointment attendance by sex (p=0.537). Younger age (p=0.006) and shorter hospital stays (p=0.042) were associated with a higher likelihood of attending scheduled follow-up appointments as shown in Table 2.
Multivariate logistic regression that included patient sex, length of stay, and age found that older age was significantly associated with decreased odds of being seen (OR .96, p=.003), but length of stay and sex were not significant. The model demonstrated good overall fit (Hosmer-Lemeshow: χ²=4.74, df=8, p=0.78), suggesting that older patients may be less likely to complete post-fracture follow-up, even when controlling for other factors.
Discussion
Previous studies have highlighted disparities in osteoporosis management and post-fracture bone health evaluation. Barton et al (Cummings, Nevitt, Browner, et al. 1995). reported that 90% of their cohort did not receive post-fracture care, leading to preventable subsequent fractures. While numerous studies have demonstrated the efficacy of Fracture Liaison Service (FLS) programs in reducing secondary fractures and mortality, access remains a challenge. This study highlights a persistent public health issue, particularly among populations in rural areas who may lack access to an FLS program whether for personal reasons or missed referrals.
This study revealed a 49.8% referral rate to bone health evaluation following hip fracture, highlighting a considerable gap in post-fracture management with nearly half of patients not referred for bone health evaluation. We identified factors such as variation in order sets, comorbidities, disposition planning, and the involvement of different teams during hospitalization that may contribute to the systemic and physician-related referral barriers. For example, patients who transition to other services, such as medicine or skilled nursing facilities after discharge, may face delays in referral or follow-up for BH evaluations. For patients with longer stays, the focus might be on managing acute issues, leading to potential delays or omissions in making referrals. This may suggest bias and/or different clinical practices in those playing a role in medical decision making at hospital discharge. These include the lack of standardized team protocols or inconsistent adherence to clinical guidelines, which can result in missed opportunities for appropriate referrals. Our review identified several pre-made order sets used by physicians. Some include a BHE referral within the set, while others require it to be ordered separately. As a center, we are standardizing order sets to include BHE referral, and recommend other centers do the same, paying careful attention to patients that may fall outside a traditional geriatric hip fracture order set.
Because every patient included in the study was at least 65-years of age and sustained a hip fracture, all fit ISCD and BHOF criteria for bone health evaluation. While majority of the cohort were women, we did not find differences in referral rates between sexes. We would typically expect referral disparity as has been found in previous studies (Phy, Vanness, Melton, et al. 2005). Phy et al. reveals women who experienced a hip fracture were 5 times more likely to die within 3 months compared to age- and sex-matched controls, while men had almost an eightfold increased mortality risk in the same period (Keaveny, Adams, Orwoll, et al. 2024). Because men attended bone health evaluations at similar rates when a referral was received, it is possible that missed referrals for bone health contribute to the increase in long-term mortality risk experienced by men following hip fracture.
A multivariate logistic regression found that those undergoing THA had lower referral odds than those undergoing ORIF, while age and length of stay were not significant. In terms of attendance, older patients had lower odds of attending their appointments. This could be due to barriers faced by older adults, such as transportation or social support issues, preventing easy completion of follow-up visits, though additional studies are needed. While the etiology of missed referrals remains unclear, this study highlights an unmet need for clinician-facing studies to identify and educate healthcare teams on the importance of bone health evaluations following fracture. When referred, patients attended their bone health evaluation at similar rates. Larger populations should be examined to determine if this finding remains consistent, with future studies seeking to examine the cause of this disparity. Because bone health evaluation and treatment has been shown to significantly reduce the risk of subsequent fracture, it is imperative that at-risk patients are provided the opportunity for bone health evaluation (Chattaris et al. 2020; Wolfe, McDonald, and Holmes 2020).
While most barriers to referral were found within the healthcare team, patient specific barriers appear to contribute to missed visits. Patients who were older and patients with longer hospital stays following their fracture were less likely to attend their scheduled bone health evaluation. This may represent an access issue for this subset of the population, with other studies finding older adults and those with more severe injuries less likely to attend healthcare appointments (Wallace et al. 2005; Krasniuk and Crizzle 2023; Chevalley et al. 2002). This is an important factor to address, as patients who are older and who have suffered a hip fracture are significantly more likely to face subsequent fracture and/or higher 1-year mortality rates. One option that may address these gaps in care includes completing bone health screening before the patient discharges from the hospital when patients are at-risk for transportation issues (Åstrand, Thorngren, and Tägil 2006; Hinkamp et al. 2025). While calcium levels were also significantly different, the cause of this finding is unclear and may be incidental.
The study’s retrospective design and reliance on EMR data are its primary limitations. The retrospective design may introduce selection bias due to the inability to control or account for confounding variables and the possibility of incomplete data in EMR. Additionally, this study was completed at a single institution, and findings may not be consistent with other institutions that have different referral protocols following suspected fragility fracture. As such, future studies should include large, multi-site studies to examine referral and visit attendance barriers in diverse populations. Important social determinants of health, such as support systems post- operatively, transportation, cognitive impairment, and discharge location, were not directly evaluated in the present study, underscoring the need for in-depth studies evaluating the factors at-play when hip fracture patients fail to establish care with a BH clinic. We also did not evaluate calcium production pathologies.
Conclusion
Patients with shorter LOS, higher calcium values, and hip fracture type were significantly more likely to be referred for BH evaluation following hip fracture. These findings highlight disparities in referrals, as every included patient met guidelines for bone mineral density screening. Future research should focus on improving referral rates and addressing barriers to attendance, particularly for older patients and those with extended hospital stays. Implementing systematic changes such as universal order-sets including BH referrals hospital wide or initiating bone health evaluation during the first post-operative orthopaedic visit may serve as a critical opportunity to improve adherence to screening and treatment recommendations. Additional recommendations to the referring team should include reevaluation of the standardized referral protocol and collaboration with other disciplines that participate in the referral process.