

Introduction
Effective control of pain following orthopedic procedures remains a major challenge despite advances in regional anesthesia and the advent of locally delivered sustained-release formulations. Exparel, a liposomal formulation of bupivacaine (LB), extends local drug exposure but generally does not provide meaningful activity beyond ~72 hours (Shing and Tighe 2022). Recent data have demonstrated the potential of neuromodulation in the long-term treatment of postoperative pain (Ilfeld et al. 2021). These findings have prompted the clinical investigation of a platform, RELAY, which combines peripheral nerve block and neuromodulation with the aim of enhancing and prolonging analgesia following orthopedic surgery.
The RELAY System
The RELAY system (Gate Science, Moultonborough, NH) is a dual-mechanism platform that delivers simultaneous and sequential nerve block and neuromodulation to a targeted peripheral nerve or plexus. The system consists of a percutaneous lead with multiple electrodes, powered by a wearable pulse generator. Parameters such as current amplitude, frequency, and cycling can be adjusted noninvasively via a Bluetooth-enabled mobile app, Gate Keeper. This app allows dynamic titration of neuromodulation intensity. The preoperative placement of the device and subsequent deployment have been reported previously (Ilfeld et al. 2025).
Methods
The intent of this analysis is to define the interplay between nerve block and neuromodulation in controlling post-operative pain.
To isolate the effects of neuromodulation and sodium channel blockade, we analyzed six patients selected from a 20-patient safety and efficacy trial of RELAY at the University of California, San Diego (NCT06818708). The inclusion criteria for the analysis —shoulder surgery, continuous peripheral nerve block (cPNB) with bupivacaine through postoperative day three, neuromodulation through postoperative day 7, and completion of follow-up through day 14—were chosen to enable direct comparison with published outcomes for liposomal bupivacaine (LB) in shoulder procedures. Note the inclusion of patients receiving continuous peripheral nerve block (cPNB) through postoperative day three with the RELAY device was specified to match the local exposure associated with LB. Demographics for the RELAY cohort follow.

Randomized controlled trials of LB in shoulder surgery that were considered for this analysis included Okoroha et al. 2016; Sethi et al. 2021; Namdari et al. 2017; Abildgaard et al. 2017; and Kim et al. 2022. A pooled analysis of Sethi et al. 2021 and Okoroha et al. 2016 was chosen for comparison to RELAY data in shoulder surgery. These two studies provided favorable early analgesic effects relative to the other studies of LB, included data up to postoperative day 14 (Sethi), matched indications of Total Shoulder Arthroplasty and Rotator Cuff Repair, and had similar demographics, and had positive controls.
Consideration was also given to inclusion of cPNB without neuromodulation as the comparator to RELAY. Across randomized and prospective comparative studies in shoulder arthroplasty and arthroscopic shoulder surgery, pain scores during POD 1–3 are generally similar between cPNB and LB, with no consistent, clinically important between-group differences (>1 point on a 0–10 scale). Some trials show early advantages for the catheter within the first 24 hours, but by POD 1–3 most report non-inferior or comparable analgesia with LB; one cohort found lower day-2 pain with LB (Abildgaard et al. 2017; Kim et al. 2022; Sabesan et al. 2017; Panchamia et al. 2024; Wall et al. 2022).
Comparative Analysis
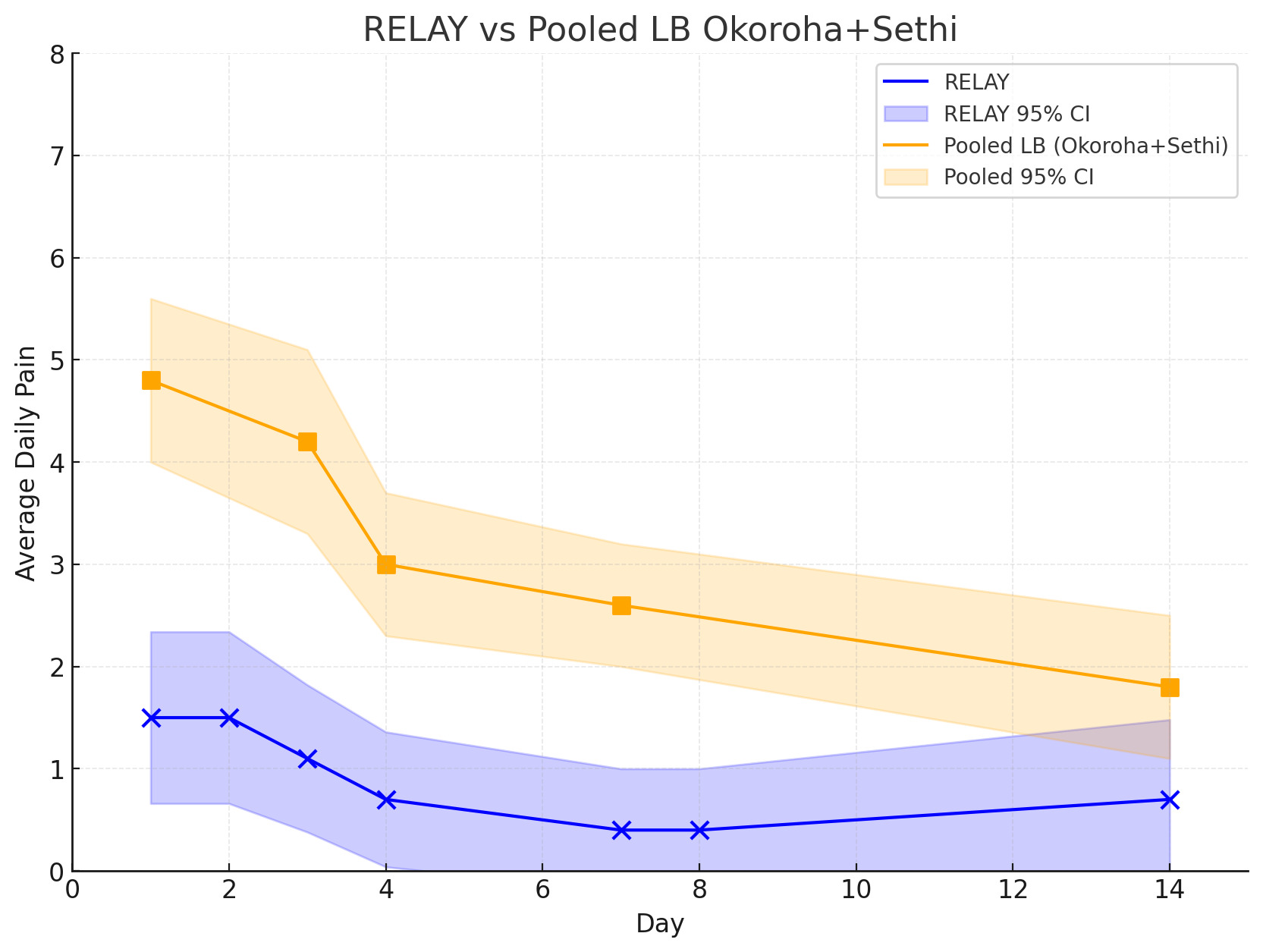
Pooled pain outcomes of LB (Sethi et al. 2021 and Okoroha et al. 2016) are compared to the pain outcomes for RELAY between post-op day 1 and 14.

The LB curve demonstrates incomplete reductions in acute pain (>3-4.8 points on a 10-point scale) through the early postoperative period, with a gradual decline to ~2 by day 14. By contrast, the RELAY curve demonstrates lower scores at all time points, rapid suppression of pain within the first 48 hours, and durable control approaching floor levels (≤1) by day 7. Confidence intervals (CIs) for both LB and RELAY were estimated from published standard deviations or estimated variance, with RELAY’s CIs reflecting small-sample pilot variability and LB’s reflecting pooled RCT-derived spread.
The LB profile is in fact advantaged relative to the other available data for LB in the literature [1].
Isolating the effect of Neuromodulation
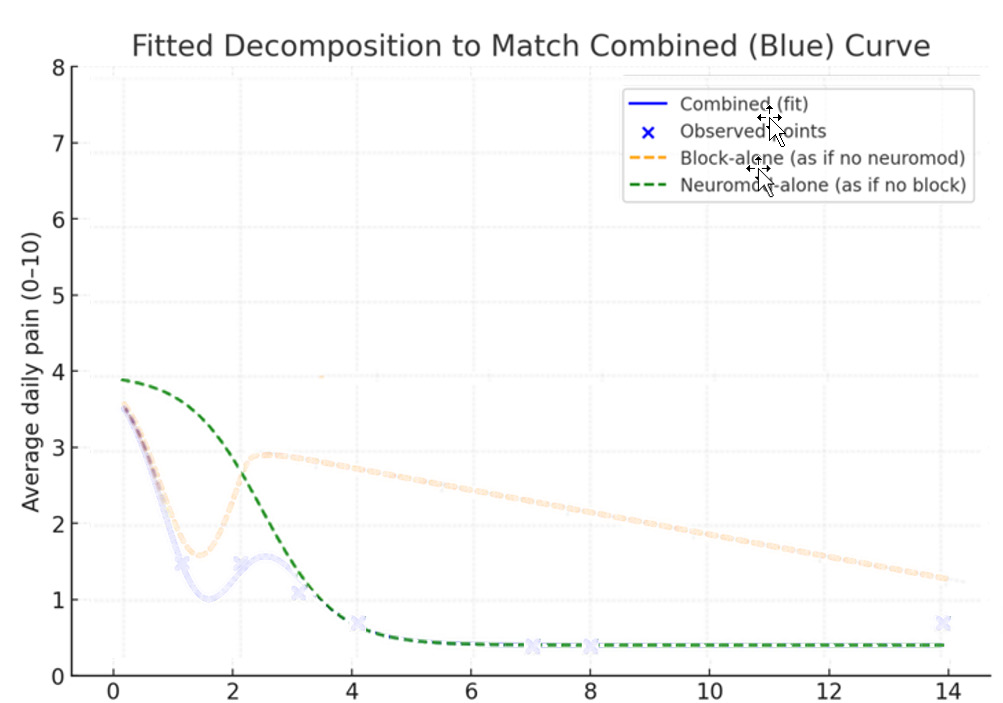
The present analysis employs fitted decomposition to isolate the contributions of nerve block x3 days and neuromodulation x7 days to RELAY’s observed analgesic trajectory over 14 days. The working assumption in the analysis is that observed differences in the pain curves can be attributed to the effect of neuromodulation.
.png)
The blue RELAY curve was constructed by decomposing the observed analgesic trajectory (the blue “combined” pain curve in figure 2) into two modeled components: an early, short-lived effect representing nerve block (Yellow), and a delayed, more sustained effect representing neuromodulation (Green). The sodium channel blockade contribution was parameterized as a rapid logistic decay consistent with local anesthetic pharmacokinetics, while the neuromodulation contribution was modeled as a logistic rise and plateau beginning as block effects waned. Summing these functions reproduced the observed RELAY data (represented in Figures 2 and 3 by the blue Xs) illustrating the additive interaction between the two mechanisms.
_of_neuromodulation_in_this_patient_population.png)
Mechanistic Interpretation
In the nerve plexus, C fibers (small, unmyelinated fibers) carry slow, dull, burning pain signals. They are central drivers of nociception and central sensitization. Aβ Fibers (large myelinated fibers) are responsible for touch, vibration, and proprioception. Importantly, Aβ fibers project into the dorsal horn where they gate nociceptive transmission (Melzack and Wall 1965). Neuromodulation selectively activates Aβ fibers, generating non-painful input that closes the gate at the dorsal horn. This reduces transmission of C-fiber nociceptive input to higher centers, blunting central sensitization.
Early after surgery, nerve block (Sodium-channel blockade) reduces both C fiber transmission, quelling the nociceptive signal from the periphery, and Aβ input is largely silenced. This limits neuromodulation’s effectiveness, since Aβ conduction is required for therapeutic gating in the dorsal horn. As the block begins to wane, Aβ conduction recovers but C-fiber nociception also reemerges. At this point, neuromodulation suppresses spinal amplification, providing a second wave of analgesia. After the block is fully resolved, neuromodulation alone continues to provide pain relief by dampening central sensitization, a known effect in chronic indications (Lo Bianco et al. 2025; Karcz et al. 2024).
Clinical Implications
In clinical practice, nerve block provides reliable analgesia at early time points. When combined with neuromodulation, however, the analgesic effect is smoothed, deepened, and prolonged.
As the effect of the nerve block dissipates on or around day three, neuromodulation sustains control of pain, preventing rebound and extending analgesia beyond the pharmacologic window of cPNB with bupivacaine. The combination of modalities has the potential to acutely and sub-acutely lower pain scores and to reduce opioid consumption in comparison to LB or cPNB alone.
Conclusions
The role of central sensitization has only recently been demonstrated as a key driver of postoperative pain (Ilfeld et al. 2021). Without directly addressing this mechanism, peripheral nerve block alone likely cannot achieve the same depth or durability of analgesia demonstrated here by RELAY. In the acute phase (days 1–3), both modalities are active in the control intense pain. As the block dissipates, neuromodulation continues to provide relief by suppressing central sensitization, thereby maintaining control in the subacute phase (days 3–30). Also, RELAY offers the unique advantage of adjustable titration of neuromodulation without modifying the drug regimen.
The combined approach of nerve block and neuromodulation leverages independent but convergent mechanisms that stack rather than compete. Given their lack of central activity, sustained-release sodium-channel formulations, whether delivered as liposomes or other biopolymers, are unlikely to reproduce the flexibility, durability, and depth of analgesia achieved by RELAY.
RELAY is the first device to combine nerve block and neuromodulation in a single platform, and the simultaneous and sequential use of these modalities provides novel insight into an important role of central sensitization in controlling post-operative pain and the therapeutic utility of neuromodulation in controlling acute pain.
Limitations
While these initial findings are coherent, they rely upon comparing data across studies. Further confirmation in larger, controlled, prospective studies will be required before final conclusions can be drawn.
Six other studies were considered for pooled analysis but not included. Sabesan et al. (2015) and Flaherty et al. (2020) showed a sharp rise in pain intensity within the first 12–24 hours, with mean scores reaching 4–5 on a 10-point scale. Namdari et al. (2017) reported more moderate pain levels (~3–4) that remained relatively stable over the first day, while Abildgaard et al. (2017) and Hillesheim et al. (2021) both documented higher initial values near 5. Vandepitte et al. (2017) observed persistently elevated pain (~6.6) at day 2. In general, each of these studies had pain scores ≥4 on day1 and lacked long-term follow-up.