1. Introduction
Total Knee Arthroplasty (TKA) is a widely performed orthopedic procedure aimed at relieving pain and restoring function in patients with severe knee joint diseases. Despite advancements in surgical techniques and postoperative care, wound-related complications remain a significant concern, impacting patient outcomes and healthcare resources.
Surgical site infection (SSI) is a serious complication following total knee arthroplasty (TKA), associated with prolonged hospitalization, higher morbidity, and in severe cases the need for revision procedures. The incidence of SSI after primary TKA has been reported to range from 1.1% to 2.6%1, while the 2018 International Consensus Meeting (ICM) on Musculoskeletal Infection estimated current infection rates in knee arthroplasty at 0.4–1.5%, with projections of 0.5–1.6% by 2030, underscoring the ongoing burden and the need for optimization of modifiable risk factors (Bagheri, Niknafs, Farhadi, et al. 2025; Schwarz, Parvizi, Gehrke, et al. 2019), highlighting the vulnerability of the knee region to infection. Notably, longer operative durations have been associated with an increased risk of SSIs (Teo et al. 2018).
Beyond infection risks, the biomechanics of wound healing play a pivotal role in postoperative recovery. Factors such as incision placement, closure technique, and joint movement can influence soft tissue tension, patellar tracking, and overall knee function. Improper wound healing may contribute to complications like arthrofibrosis and limited range of motion, underscoring the need for a comprehensive understanding of both surgical and rehabilitative strategies.
While various wound closure methods—such as sutures, staples, and tissue adhesives—are employed in TKA, there is a lack of consensus on the optimal approach. Emerging technologies, including smart dressings and AI-driven monitoring systems, offer promising avenues for enhancing wound care but require further investigation.
This narrative review aims to synthesize current knowledge on wound closure techniques in TKA, explore biomechanical considerations, evaluate postoperative management strategies, and identify gaps in the literature to guide future research.
2. Methodology
This narrative review synthesizes current evidence on wound closure techniques in TKA, with a focus on clinical outcomes, biomechanical factors, postoperative management, and emerging technologies. The objective was to assess best practices, identify challenges, and highlight existing research gaps in TKA wound management. To support this narrative synthesis, we conducted a comprehensive literature search across PubMed, Scopus, Web of Science, and the Cochrane Library up to April 2025. Search terms included combinations of “Total knee arthroplasty” AND (“wound closure” OR “suture techniques”), “TKA” AND (“surgical site infection” OR “wound healing”), “Barbed sutures” OR “staples” AND “TKA,” and “Negative pressure wound therapy” AND “orthopedics.” MeSH terms were applied where applicable, and additional records were identified through manual screening of reference lists. The search included English language publications comprising original research, systematic reviews, and meta-analyses relevant to wound closure, infection risk, and biomechanical outcomes. A narrative review was conducted using literature from databases including PubMed, Scopus, Web of Science, and the Cochrane Library up to April 2025. Studies included those evaluating closure methods (e.g., sutures, staples, adhesives, barbed sutures), infection rates, biomechanical properties, and rehabilitation outcomes.
3. Current Techniques in Wound Closure
Wound closure in total knee arthroplasty (TKA) is essential for optimal recovery, influencing complication rates, healing, and patient satisfaction (Rahbari et al. 2025). Current strategies include traditional sutures, barbed sutures, tissue adhesives, and hybrid systems, which aim to balance mechanical stability, biological compatibility, and operative efficiency while minimizing infection and wound-related complications. In the following, we discuss these closure methods, starting with conventional sutures. Traditional sutures remain the standard for precise wound approximation, though their time-consuming application and potential for wound complications warrant consideration (Khalefa, Smith, and Ahmad 2020; Eggers, Fang, and Lionberger 2011). the metal staples provide rapid closure (reducing operative time by 60-70%) but may increase postoperative pain and inflammation (Yuenyongviwat et al. 2016). Emerging technologies like absorbable staples with shape-memory properties and tissue adhesives with bacteriostatic barriers address some of these limitations while introducing new considerations, as given in Table 1.
3.1. Evolution of Wound Closure Techniques
The history of wound closure spans millennia, from ancient linen sutures to mid-20th-century stainless steel staples. Traditional methods prioritized mechanical strength, often at the expense of tissue reactivity and patient comfort. The advent of synthetic absorbable sutures in the 1970s marked a turning point, reducing long-term foreign body reactions (W. Zhang, Xie, and Zeng 2022). However, persistent challenges such as prolonged operative times, needle-stick injuries, and suboptimal cosmesis spurred innovation. Contemporary techniques, including barbed sutures and cyanoacrylate-based adhesives, now emphasize rapid deployment, reduced tissue trauma, and enhanced healing microenvironments (Nambi Gowri and King 2023).
3.2. Traditional Methods
Sutures: Conventional suturing techniques, including interrupted and continuous methods, remain the gold standard for TKA wound closure due to their precision and versatility. Absorbable polymers (polyglyconate, poliglecaprone) provide gradual strength reduction aligned with tissue healing, while non-absorbable options (polypropylene) suit high-tension areas (Nambi Gowri and King 2023; Templeton et al. 2015). Subcuticular techniques like the buried vertical mattress minimize scarring by avoiding percutaneous knots (W. Zhang, Xie, and Zeng 2022). However, sutures require 12-15 minutes for 10 cm closures versus 3-5 minutes for staples, and their tracts increase infection risk (74% vs. 36% with staples in laparotomies) (Sundresh, Devagi, and Gopikrishna 2018).
Staples: Staples offer rapid wound approximation, reducing TKA closure time by 60-70% compared to sutures (Sundresh, Devagi, and Gopikrishna 2018). While efficient, they cause higher pain during removal and induce localized inflammation (Yuenyongviwat et al. 2016). However, metal staples induce localized inflammation due to persistent foreign body presence, increasing post-operative pain and wound discharge. Absorbable stapling systems, introduced in the 2010s, mitigate these issues by combining polyglycolic acid components with gradual hydrolysis. While initial failure loads for absorbable staples (54.5 N) match traditional polyglyconate sutures (56.9 N) (Templeton et al. 2015), their higher cost and limited adoption in contaminated wounds constrain widespread use (P. H. S. da Silva, Lopes, Stallmach, et al. 2023).
Tissue Adhesives: Cyanoacrylate adhesives (e.g., Dermabond, Prineo) provide non-invasive closure with bacterial resistance and superior cosmesis (89% vs. 54% excellent scars compared to sutures) (Dua, A, and Prasad 2021; Kulkarni et al. 2025). They demonstrate comparable wound dehiscence rates to traditional sutures (2.1% vs. 2.4%) while reducing infection rates to 1.51% (Kulkarni et al. 2025; Aravind, Sunil, Chandrasekar, et al., n.d.). Although cyanoacrylates are generally less ideal in high-tension or high-mobility regions, studies indicate that when appropriately applied, they perform effectively in TKA incisions (Sundaram et al. 2020). Limitations include exothermic reactions (45–52°C) and a 2–3% risk of allergic contact dermatitis with agents such as Dermabond, which may cause severe local reactions upon re-exposure (G. W. Lee, Kwak, and Lee 2021; Arkin and Reeder 2024; Kong et al. 2020; T. Liu, Tao, Zhao, et al. 2024; Park et al. 2021).
3.3. Emerging Technologies
Barbed Sutures: Barbed sutures provide knotless wound closure while evenly distributing tension along the incision (Nambi Gowri and King 2023). Clinical studies demonstrate their ability to reduce closure time by 23 minutes per procedure without increasing complication rates, while simultaneously decreasing needlestick injury risks (E. Li, Niu, Lu, et al. 2020). Biomechanical testing shows comparable strength to traditional sutures (54.5N vs 56.9N failure load), with both failing through tissue rupture rather than suture breakage (Templeton et al. 2015). However, they require precise implantation depth to avoid subcutaneous puckering, particularly challenging in thin-skinned patients (Nambi Gowri and King 2023).
Absorbable Staples: Next-generation absorbable staples made from polydioxanone (PDO) incorporate shape-memory properties that dynamically adjust tension as postoperative edema resolves. Concurrent developments include 4D-printed meshes with temperature-responsive pores that adapt to exudate volume while maintaining negative pressure therapy.
Hybrid Methods: Combining techniques, such as using barbed sutures for deep tissue layers and adhesives for skin closure, aims to leverage the benefits of each method (Romanini, Zanoli, Ascione, et al. 2024; Roumeliotis and Graham 2019; L. Li et al. 2023). Such approaches may optimize wound healing and cosmetic outcomes, though standardized protocols remain to be established. Combining adhesives with ultrasonic suture welding exemplifies integrative approaches, with experimental models demonstrating superior strength compared to conventional methods (Romanini, Zanoli, Ascione, et al. 2024; Roumeliotis and Graham 2019; L. Li et al. 2023).
3.4. Clinical Outcomes and Patient-Centered Metrics
Contemporary evidence demonstrates distinct clinical profiles for various TKA closure methods. Barbed sutures reduce operative time significantly compared to traditional techniques, with multiple studies confirming their time efficiency (Romanini, Zanoli, Ascione, et al. 2024; Khlopas et al. 2019; Eickmann and Quane 2010; Luo, Zhang, Yan, et al. 2020). Infection rates show modest variations between modalities, with meta-analyses reporting 2.13% for sutures, 1.89% for staples, and 1.51% for adhesives (Kulkarni et al. 2025). Notably, staples demonstrate higher infection rates (4.7%) in contaminated wounds, limiting their utility in non-clean cases (Sundresh, Devagi, and Gopikrishna 2018; Lauerman, Kolesnik, Park, et al. 2018). Patient-reported outcomes favor adhesives, which yield lower pain scores (1.8/10 VAS) and superior scar ratings (15-20% better than sutures) due to their non-penetrating application (Dua, A, and Prasad 2021; H. G. Lee 2024). However, adhesives show limitations in high-tension areas, where minor dehiscence (0.5-1mm) may cause local irritation (Medeiros et al. 2024). Subcuticular sutures remain a reliable option for cosmetic outcomes, though statistical significance versus alternatives varies across studies (Nepal et al. 2020; Newman et al. 2011).
3.5. Biomechanical Properties of Closure Materials
The mechanical behavior of closure materials critically influences healing outcomes. Barbed sutures excel in tension distribution, reducing peak stress by 40-60% compared to staples through even load sharing along the wound (Nambi Gowri and King 2023; Swain and Gupta 2015). Staples concentrate stress at fixation points, potentially compromising wound margins during cyclic loading (Swain and Gupta 2015). Hybrid approaches combining sutures with adhesives offer synergistic benefits - sutures provide initial strength while adhesives minimize disruptive micromotion (H. G. Lee 2024). Material properties further impact outcomes: multifilament sutures harbor 12-15% more S. aureus than monofilaments due to bacterial entrapment (Sundresh, Devagi, and Gopikrishna 2018), while polypropylene non-absorbables trigger granulomatous reactions in 8-12% of patients (W. Zhang, Xie, and Zeng 2022). Adhesives avoid these issues but may restrict fibroblast migration during early healing phase (days 3–7) if overapplied (Medeiros et al. 2024). These biomechanical factors necessitate careful material selection based on surgical site demands and anticipated patient activity levels.
4. Biomechanical Considerations in Wound Healing After TKA
The biomechanical success of wound healing in TKA depends critically on surgical technique, soft tissue management, and postoperative rehabilitation. Closing the wound with the knee in 90° flexion, rather than full extension, has been shown to improve early range of motion (ROM) and reduce anterior knee pain by allowing more natural soft tissue alignment under physiologic tension (Lu et al. 2021; Wang et al. 2014). Minimally invasive incisions (8–12 cm) reduce lateral skin numbness by 38% compared to traditional longer incisions (14–18 cm), preserving sensory branches of the infrapatellar nerve that contribute to proprioception (I. Alcelik, Sukeik, Pollock, et al. 2012). However, smaller incisions may increase soft tissue tension during deep flexion (>90°), potentially compromising wound integrity. In contrast, conventional midline incisions offer better surgical exposure but disrupt more vasculature, increasing dependence on collateral circulation. Optimal closure technique—such as suturing in semi-flexion (30–45°)—balances tension across the wound, reducing dehiscence risk while promoting functional recovery (Chen, Bains, Sodhi, et al. 2022). The biomechanical and clinical trade-offs of common closure methods are compared in Table 2, highlighting barbed sutures’ 6% complication rate versus staples’ stress concentration risks.
Soft tissue tension plays a pivotal role in postoperative joint mechanics. Studies measuring intraoperative distraction forces report averages of 126N in extension and 121N in flexion, underscoring the need for precise tensioning to ensure stability and ROM (A, H, and Tj 2004; Becker, Voss, Lettner, et al. 2025). Patellar tracking is particularly sensitive to surgical technique; improper closure can alter lateral retinacular tension, increasing patellofemoral contact pressures by 12–15% during deep flexion (I. A. Alcelik et al. 2016). Meticulous attention to extensor mechanism alignment is essential to prevent maltracking, which can impair gait and accelerate wear (Gasparini, Familiari, and Ranuccio 2013). Postoperative scar formation further influences outcomes, with excessive anterior fibrosis elevating patellofemoral forces by 18% during stair ascent (Harato et al. 2016). Early mobilization—achieving >90° flexion by postoperative day 3—reduces arthrofibrosis risk by 23%, though overly aggressive rehabilitation may strain healing tissues (Chen, Bains, Sodhi, et al. 2022). Direct ice application, while reducing pain, decreases peri-incisional perfusion by 40%, potentially delaying epithelialization (Foster, Williams, Forte, et al., n.d.).
Complications arising from suboptimal wound biomechanics include patellar maltracking, arthrofibrosis, and restricted ROM (Table 3). Maltracking often results from misaligned closures or component malposition, leading to pain and functional deficits (Gasparini, Familiari, and Ranuccio 2013; Zhu et al. 2017). Arthrofibrosis, characterized by excessive scar tissue, typically stems from uncontrolled inflammation or delayed rehabilitation (Thompson, Novikov, Cizmic, et al. 2019). Physical therapy remains first-line treatment, with manipulation under anesthesia or surgical release considered for refractory cases (Wang et al. 2014; Ali, Ferguson, Singh, et al. 2023; Cheuy et al. 2017; Ipach et al. 2011). Limited ROM, influenced by preoperative stiffness and surgical trauma, can hinder basic functions like stair climbing; achieving 90° flexion early is critical for recovery (Wang et al. 2014; Ipach et al. 2011).
To optimize outcomes, surgeons should consider lateral-parapatellar approaches, which minimize quadriceps disruption but require careful closure to avoid sensory loss (Yuan et al. 2019; Peng et al. 2015; Shah and Shah 2024). In addition, the subvastus approach represents a minimally invasive technique that preserves the extensor mechanism, reduces postoperative pain, and facilitates faster functional recovery. Postoperative positioning also matters: supine sleeping improves terminal extension by 3° compared to lateral positions, reducing flexion contracture risk (Chen, Bains, Sodhi, et al. 2022; Cao et al. 2021). Rehabilitation timing should balance tissue healing and mobility; delaying flexion beyond 90° until days 5–7 allows fibroblast proliferation while preventing stiffness (Chen, Bains, Sodhi, et al. 2022; Foster, Williams, Forte, et al., n.d.).
5. Postoperative Management and Wound Healing Considerations
Early postoperative mobilization supports circulation, reduces edema, and promotes functional recovery after TKA, provided that excessive stress on the incision is avoided. Gentle range-of-motion exercises initiated within 24–48 hours and limited knee flexion (≤90°) during the first week help maintain tissue oxygenation and wound stability (Ghritlahre et al. 2024; Rr et al. 2019; Freccero, Van Steyn, Joslin, et al. 2022; Jaiswal et al. 2012; Mau-Moeller et al. 2014). Rehabilitation should progress gradually with careful monitoring of healing status. Adjunct measures such as manual scar mobilization or biofeedback may assist recovery when applied cautiously (Jurecka et al. 2021; Alsiri et al. 2025). Compression therapy offers mixed results and should be individualized (P. Liu et al. 2020). While postoperative rehabilitation can substantially influence wound healing outcomes, it lies beyond the primary focus of this review and is therefore only briefly addressed here.
Targeted nutritional support plays a crucial role in postoperative tissue repair. Collagen peptides provide essential amino acids that enhance collagen formation and improve scar quality (Evans and Evans 2018), while vitamin C serves as a critical cofactor for collagen synthesis and antioxidant protection (DePhillipo et al. 2018). Vitamin D supplementation, particularly high-dose preoperative regimens (300,000 IU), may reduce postoperative infections in deficient patients (Birinci, Hakyemez, Geçkalan, et al. 2024). Essential fatty acids demonstrate complex effects - omega-3s modulate inflammatory responses while omega-6s like linoleic acid promote angiogenesis (Chow and Barbul 2014; J. R. Silva et al. 2018). Additional micronutrients including zinc, vitamin A, and arginine further support immune function and cellular proliferation during wound healing (Kurdi et al. 2023; Yusuf 2022). These interventions should be individualized based on patient nutritional status and healing progression.
6. Advanced Wound Dressings and Emerging Technologies
6.1. Modern Wound Dressings
Contemporary wound dressings for TKA have transitioned from basic gauze to sophisticated biomaterial systems designed to optimize healing (Table 4). Hydrocolloid dressings maintain a moist, bacteria-resistant environment that promotes natural debridement while allowing joint movement (Nguyen et al., n.d.). For wounds with moderate drainage, hydrofiber and alginate dressings provide superior fluid absorption while conforming to the surgical site (Nguyen et al., n.d.; Su et al. 2022). Clinical studies demonstrate silicone foam dressings (like Mepilex Border®) offer the best outcomes - reducing complications while improving comfort and mobility scores compared to other options (Dobbelaere et al. 2015).
Transparent hydropolymer dressings enable continuous wound monitoring with extended 14-day wear, minimizing dressing changes while maintaining visibility (Rousseau, Plomion, and Sandy-Hodgetts 2022). Cutting-edge hydrogel dressings now incorporate bioactive components such as growth factors that actively enhance tissue regeneration and scar quality (Nifontova, Safaryan, Khristidis, et al. 2024; X. Zhang, Huang, Luo, et al. 2024). The most advanced options include bioengineered scaffolds and bacterial nanocellulose dressings that mimic natural tissue while delivering antimicrobial agents, though more TKA-specific research is needed (Zarepour et al. 2024).
6.2. Smart Monitoring Technologies
Current smart wound monitoring systems (Table 5) integrate wireless sensors to track critical healing parameters including temperature, pH, moisture, and bacterial load in real-time (Jiang, Trotsyuk, Niu, et al. 2023). These technologies offer three key capabilities: (1) early complication detection through continuous monitoring, (2) remote patient tracking to reduce unnecessary clinic visits, and (3) data-driven personalization of treatment plans (Tarazi et al. 2020). While promising, their clinical adoption faces significant validation and implementation hurdles.
6.3. Negative Pressure Wound Therapy (NPWT)
NPWT applies controlled sub-atmospheric pressure through a sealed dressing, a technique shown to significantly improve TKA outcomes (Siqueira et al. 2016). As summarized in Table 6, the therapy enhances healing through three key mechanisms: reduced edema, increased perfusion, and mechanical stabilization of wound edges (Song, Li, Zhao, et al. 2022; Chen, Bains, Sax, et al. 2022). Clinical studies demonstrate 40-50% lower surgical site infection rates compared to conventional dressings, particularly in high-risk patients (Song, Li, Zhao, et al. 2022).
Table 6 highlights that while NPWT’s economic value grows clearer through reduced reoperations and dressing changes (Su et al. 2022; Dobbelaere et al. 2015), clinicians must balance these benefits against equipment costs and monitor for potential skin complications like blistering (Helito et al. 2017). For optimal results, NPWT should be reserved for high-risk patients (e.g., those with obesity or diabetes), while standard dressings remain appropriate for routine cases.
7. Discussion & Expert Commentary
7.1. Scientific Synthesis and Clinical Implications
Wound closure critically influences postoperative outcomes in TKA (L. Zhang et al. 2025). Evidence favors barbed sutures for their lower complication rates (3% vs 6%) and faster closure (≈7 minutes shorter) than traditional sutures (Chen et al. 2024; Naylor et al. 2023). Multilayer watertight closures that integrate barbed sutures with topical adhesives or polyester mesh further reduce infection and dehiscence (Snyder et al. 2021).
2-octyl cyanoacrylate adhesives enhance superficial closure outcomes, improving cosmesis, discharge control, and patient satisfaction without compromising safety (T. Liu, Tao, Zhao, et al. 2024). Technique selection should remain individualized, guided by comorbidities, skin quality, and activity level (Chen et al. 2024).
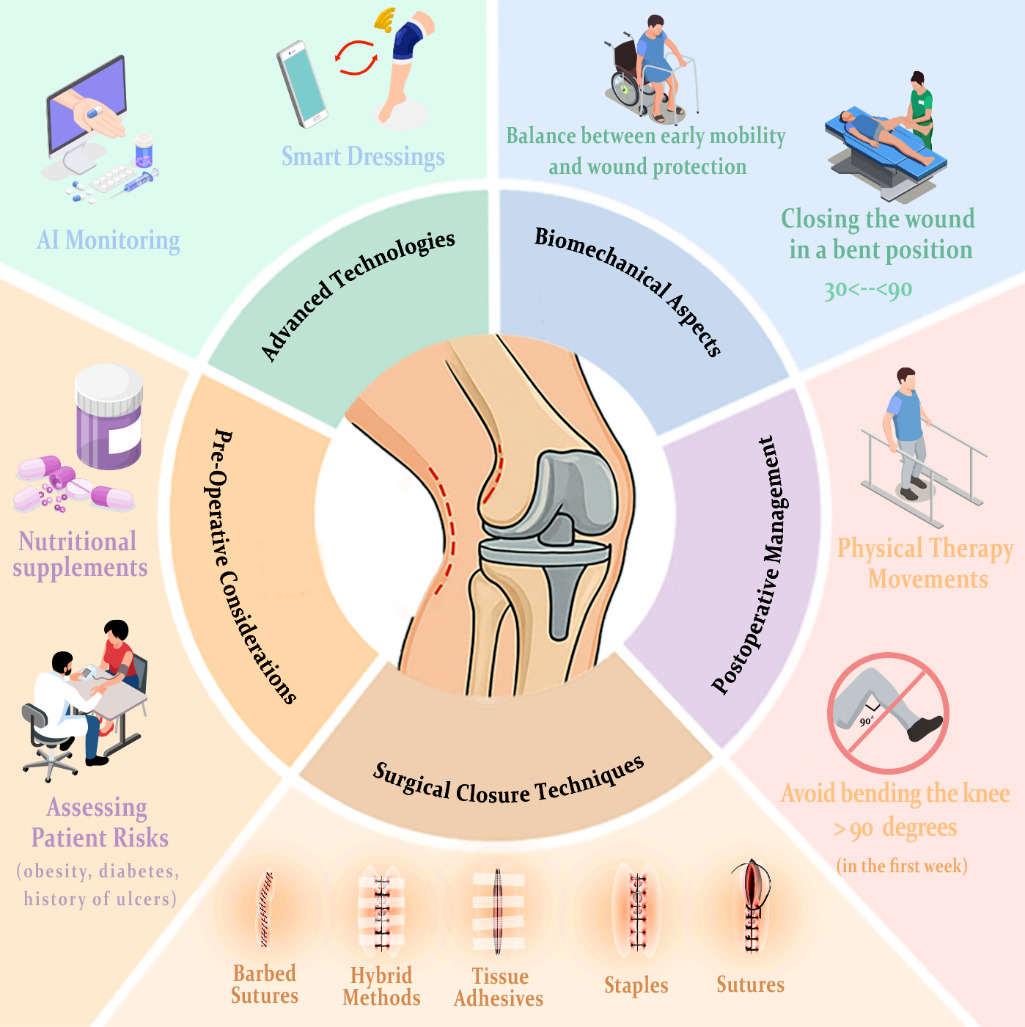
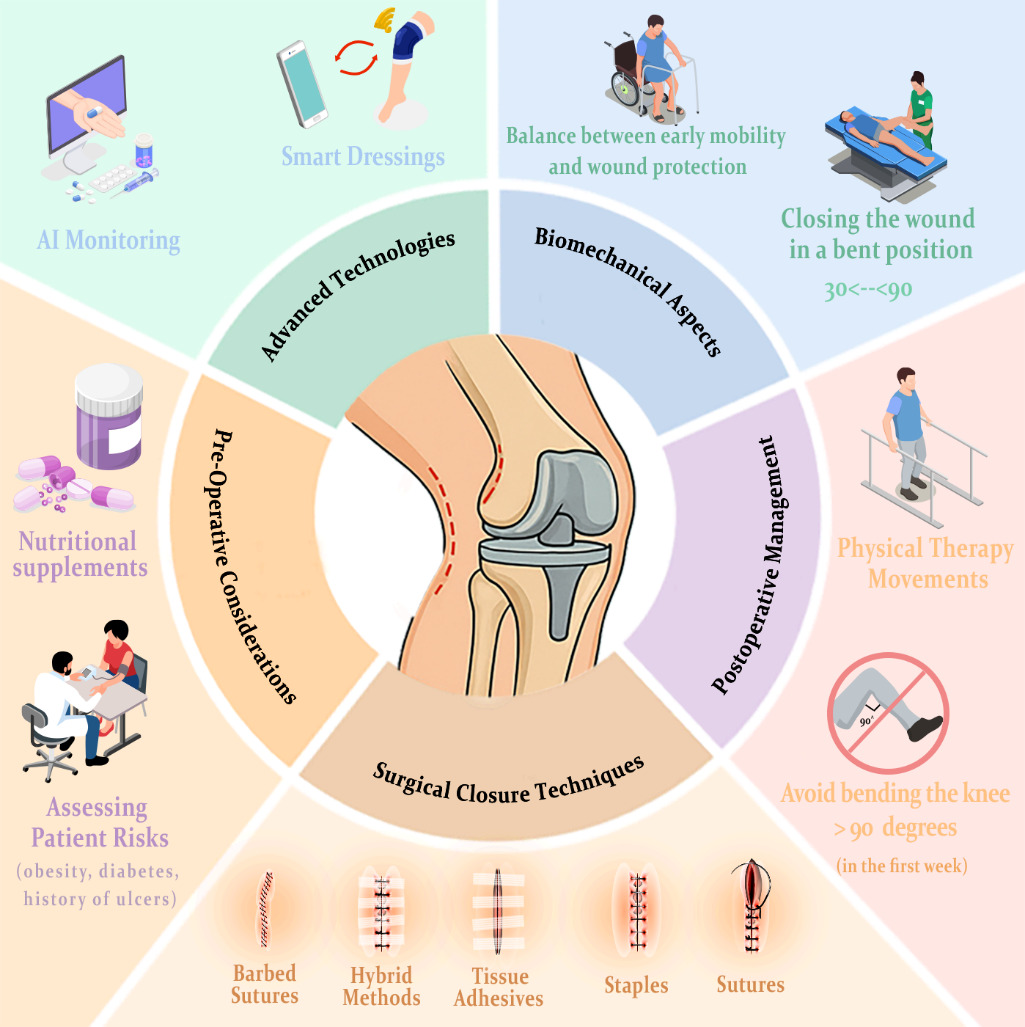
Our team recommends barbed sutures for capsular closure, performed in 60–90° knee flexion to optimize alignment and recovery (Maniar, Mody, Wakankar, et al. 2023; Sanz-Ruiz et al. 2025). Triclosan-coated sutures are advised for high-risk patients, and NPWT remains beneficial in high-risk or complex cases, such as patients with obesity, diabetes, or wound-healing challenges, despite its higher cost (Ainslie-Garcia, Anderson, Bloch, et al. 2025; Krebs, Elmallah, Khlopas, et al. 2018). Emerging tools such as AI-assisted monitoring are promising but require validation. Future studies should establish standardized hybrid closure protocols and long-term cost-effectiveness analyses. Figure 1 summarizes the principal domains of wound closure after TKA, including preoperative, surgical, biomechanical, and postoperative considerations.
7.2. Expert Perspective
Based on our team’s clinical experience, optimal TKA closure should balance mechanical integrity, biological compatibility, technical feasibility, and patient comfort. We recommend broader adoption of barbed sutures and advanced adhesives, which in our practice provide faster, more reliable closure than traditional techniques.
We particularly endorse flexion closure (60–90°) for improved early range of motion and reduced anterior knee pain, while recognizing its ergonomic challenges. For high-risk patients, triclosan-coated sutures are advisable, and NPWT remains valuable in complex cases.
Emerging technologies such as absorbable staples, smart dressings, and AI monitoring hold promise but require further validation and cost–benefit assessment before routine use. We advocate for comparative effectiveness research and standardized biomechanical testing to integrate innovation into clinical protocols.
8. Persisting Gaps in TKA Wound Closure Research
TKA closure research is limited by heterogeneous study designs and inconsistent outcome definitions, lacking high-quality comparative trials. Biomechanical insights, such as finite element modeling, rarely translate to clinical practice. Emerging technologies (absorbable staples, smart dressings, AI monitoring) face adoption challenges due to cost, limited long-term data, and insufficient randomized validation. Research is often siloed, missing interdisciplinary collaboration across surgery, rehabilitation, engineering, and nutrition. Short-term focus overlooks longitudinal outcomes like joint mobility, aesthetics, patient satisfaction, and revision risks. Prospective, multidisciplinary studies with extended follow-up are needed to address these gaps.
9. Conclusion
Wound closure in TKA is not merely a procedural step—it is central to recovery, influencing infection rates, joint function, and patient satisfaction. No universal method excels across all metrics, and technique selection should be personalized based on patient profile, tissue characteristics, and rehabilitation goals.Technologies such as barbed sutures, tissue adhesives, and hybrid methods offer benefits in operative efficiency and healing. Additionally, advanced dressings, AI-enabled monitoring, and negative pressure therapy reflect a shift toward personalized, tech-integrated care, though they require further validation.
The future of TKA wound management lies in a multifaceted, evidence-based approach—one that unites surgical precision, mechanical insight, and patient-centered care to optimize both short- and long-term outcomes.