Introduction
Injuries to the acromioclavicular (AC) joint typically occur in adults due to sports-related trauma and are relatively common, accounting for approximately 9-12% of all shoulder girdle injuries (Stucken and Cohen 2015; Mazzocca, Arciero, and Bicos 2007; Pallis et al. 2012; Simovitch et al. 2009; Peebles et al. 2023; Aliberti et al. 2020; Chillemi et al. 2013; Mahajan, Kumar, and Mishra 2019). AC joint injuries are most commonly observed in young patients aged 20-30 and have a roughly five times greater incidence in men compared to women (Stucken and Cohen 2015; Mazzocca, Arciero, and Bicos 2007; Pallis et al. 2012; Simovitch et al. 2009; Peebles et al. 2023; Aliberti et al. 2020; Chillemi et al. 2013). The most common mechanism of injury is a fall onto the shoulder with the arm in an adducted position, leading to displacement of the acromion medially and inferiorly relative to the clavicle (Simovitch et al. 2009; Peebles et al. 2023; Aliberti et al. 2020; Johansen et al. 2011; Turgut et al. 2022). Injuries to the AC joint can be categorized using the Rockwood classification system, which sorts injuries from Type I to Type VI which increase in severity (Lau et al. 2021; Gorbaty, Hsu, and Gee 2017; Beitzel et al. 2014). Type I and II AC joint injuries are typically managed non-operatively, while injuries graded as Types IV-VI are typically treated operatively with various techniques, including hook plate fixation. There is currently no consensus on the appropriate treatment for type III AC joint injuries; however, these are often treated non-operatively initially and surgery may be considered if conservative treatment fails (Simovitch et al. 2009; Mahajan, Kumar, and Mishra 2019; Frank et al. 2019).
Fixation of AC joint injuries with a hook plate is advantageous in that it provides a high strength construct and initial rotational mobility (Metzlaff et al. 2016; Koukakis et al. 2008). However, hook plates require an additional procedure for implant removal. Additionally, prior literature has shown hook plate fixation to be associated with numerous potential complications such as infection, wound complications, implant migration, loss of reduction after implant removal, and subacromial osteolysis due to interaction of the hook with the acromion (Metzlaff et al. 2016; Arirachakaran et al. 2017; Liu et al. 2018). Major potential intra-operative complications can include fracture of the acromion or tear of the rotator cuff during hook plate placement, especially in patients with poor bone quality (Metzlaff et al. 2016; Arirachakaran et al. 2017; Liu et al. 2018).
There is a paucity of recent literature examining the complications after hook plate fixation. The purpose of this systematic review was to evaluate the most common complications following hook plate fixation of the acromioclavicular joint. We hypothesized that hook plate fixation for AC joint injuries has a wide range of potential complications with variable complication rates.
Methods
A comprehensive search of PubMed, Embase, Web of Science, and Cochrane Library databases was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines in April 2023. The search strategy utilized is reported in Appendix 1.
Studies were included if they evaluated males and females of any age group who underwent hook plate fixation for the management of AC joint injuries, were prospective or retrospective studies, described intra-operative or post-operative complications in patients undergoing hook plate fixation, and were published between 2000 and 2024. Studies that were not written in the English language, were translational or cadaveric, did not evaluate hook plate fixation specifically in the context of AC joint injury, did not report complications, had fewer than 20 months of minimum follow-up, or had study designs that were systematic reviews, narrative reviews, conference abstracts, technical notes, letters to editors, or meta-analyses were excluded. Two authors (A.T.A. and G.E.O.) independently screened titles, abstracts, and full article texts using the online software program Covidence (Veritas Health Innovation Ltd; Melbourne, Australia). Any disagreements were resolved with discussion leading to consensus between the two screening authors and a third senior author (M.K.M.).
Data Extraction and Quality Assessment
The following information was collected from each study: demographics (e.g. gender and age distribution of included patients), mean follow-up time, mechanism of injury causing AC joint injury, athletic level and sport played, level of activity, and history of osteoporosis or osteoarthritis. Other data extracted included type of AC joint injury and outcomes including complications, subjective shoulder function, range of motion (active, assisted active, and passive), radiographic evaluation (coracoclavicular distance), and reported pain level. Pooling of data was avoided due to high risk of bias and significant heterogeneity between included studies. As a result, a qualitative data comparison was conducted.
Assessment of Risk of Bias
Risk of bias was assessed using the default quality assessment on Covidence. Two co-authors (A.T.A. and G.E.O.) individually analyzed each study to search for several forms of biases. Each study was evaluated for sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and any other sources of bias. By searching for these 7 attributes, we attempted to minimize the occurrence of selection bias, performance bias, detection bias, attrition bias, and reporting bias.
Results
Search Results
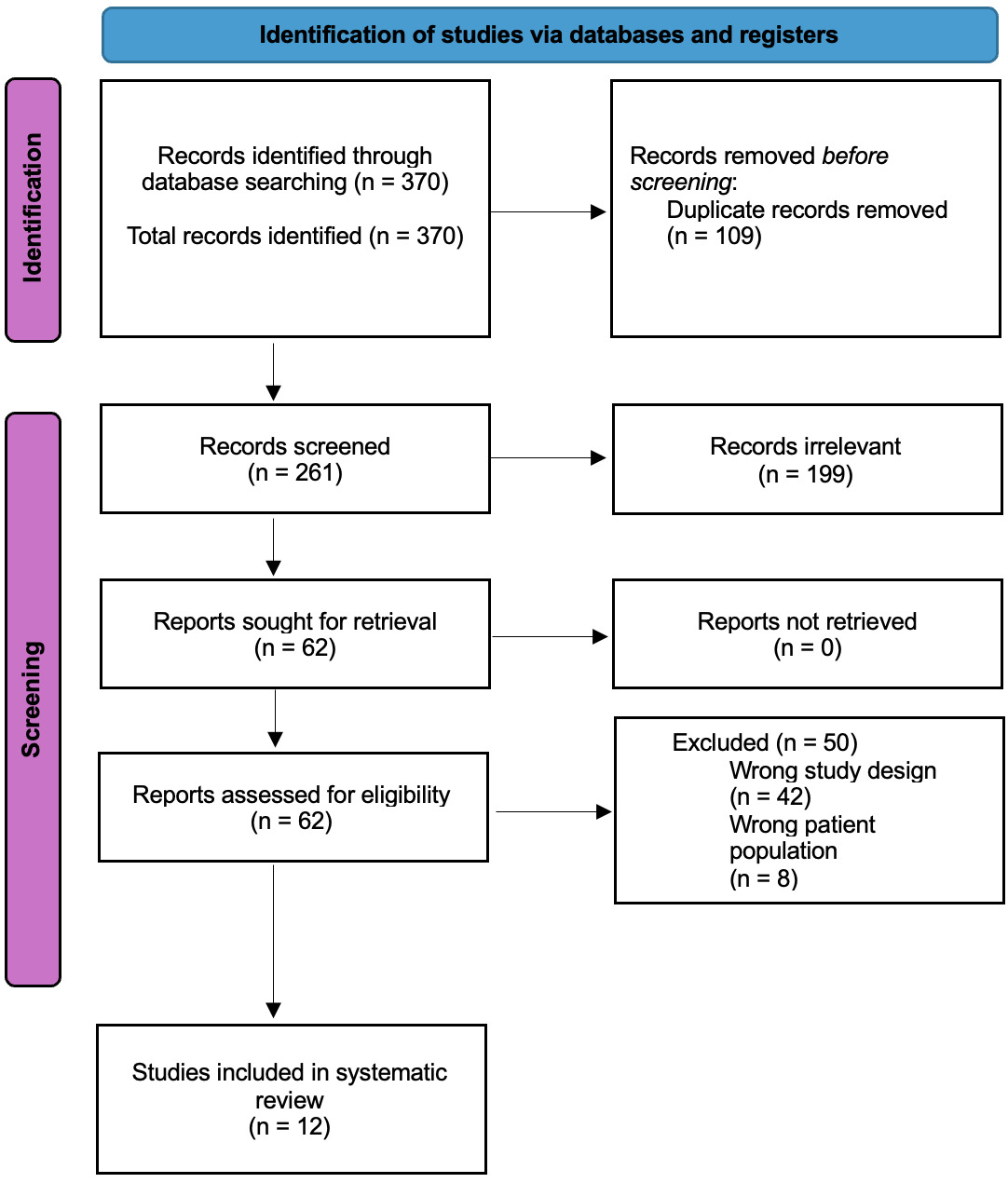
A total of 370 studies were identified in the initial search, 109 of which were duplicates and were subsequently excluded. The remaining 261 studies underwent a title and abstract screening, 199 were found to be irrelevant to the study aims and therefore excluded. The remaining 62 studies were assessed for eligibility with full-text review. After excluding 50 studies for having an incorrect study design or incorrect patient population, 12 studies were ultimately included for data extraction (Figure 1). Each of the included studies reported complications after hook plate fixation for AC joint injury.
_study_selectio.png)
Study Characteristics and Risk of Bias Assessment
The results of the risk of bias assessment can be found in Table 1. Ten studies (83.3%) had a high risk of bias due to their sequence generation, which determines which groups participants are allocated to. These studies are of high risk because they are retrospective, non-randomized, studies which inherently can have some missing statistics and biases that may affect the selection controls. Ten studies (83.3%) lacked randomization of the participants due to being retrospective studies. One study (8.3%) stated that the participants and personnel were not blinded, but rarely was it stated whether individuals assessing the data were blinded or not. Each study had sufficiently low risk of bias to ultimately be included in this systematic review.
Each of the 12 studies included evaluated hook plate fixation. Five studies were prospective (Athar et al. 2018; Fosser and Camporese 2021; Huang et al. 2018; Li et al. 2018; Shen et al. 2021), and seven studies were retrospective (Turgut et al. 2022; Chang et al. 2022; Ejam, Lind, and Falkenberg 2008; Salem and Schmelz 2009; Sheu et al. 2023; Şişman et al. 2022; Yapici 2021). Ten studies evaluated hook plate fixation without any augmentation or concomitant procedure (Turgut et al. 2022; Athar et al. 2018; Chang et al. 2022; Ejam, Lind, and Falkenberg 2008; Fosser and Camporese 2021; Huang et al. 2018; Li et al. 2018; Shen et al. 2021; Şişman et al. 2022; Yapici 2021). Two studies evaluated hook plate fixation with augmented with ligament suturing or suture anchors (Salem and Schmelz 2009; Sheu et al. 2023). A summary of patient demographics is shown in Table 2.
Isolated Hook Plate Cohort
The complications in studies evaluating hook plate fixation without augmentation included subacromial osteolysis and acromial erosion, subluxation and displacement, mechanical block, and infections (Turgut et al. 2022; Athar et al. 2018; Chang et al. 2022; Ejam, Lind, and Falkenberg 2008; Fosser and Camporese 2021; Huang et al. 2018; Li et al. 2018; Shen et al. 2021; Şişman et al. 2022; Yapici 2021). Subacromial osteolysis refers to significant bone loss due to direct contact with the hook plate whereas subacromial erosion refers to lower-grade, less generalized bone loss in the subacromial region. In 2018, Athar et al. found that 17 of 52 (33%) patients experienced complications after hook plate stabilization of AC joint disruption, with 2 (11.8% of complications, 3.8% of all patients) of those complications being erosion of the acromion (Athar et al. 2018). In a 2022 study by Chang et al., 4 of 17 patients (23.5%) sustained acromial osteolysis and 2 of 17 patients (11.8%) developed osteolysis of their distal clavicles (Chang et al. 2022). Similarly, in a study by Huang et al., 9 of 24 patients (37.5%) had subacromial erosions (Huang et al. 2018). In 2021, Shen et al. found that erosion of the acromion occurred in 1 of 19 patients (5.3%) following hook plate fixation (Shen et al. 2021).
In a 2008 study by Ejam et al., all patients (16; 100%) reported some degree of discomfort or pain (Ejam, Lind, and Falkenberg 2008). Two of 16 (12.5%) patients experienced clavicular subluxation after removal of the hook plate. One patient (6.3%) experienced superior displacement of the hook plate 3.5 months postoperatively while doing pushups (Ejam, Lind, and Falkenberg 2008). Similarly, in a 2018 study by Li et al., 2 of 43 patients (4.7%) experienced clavicular subluxation after removal of the hook plate (Li et al. 2018).
In addition, Ejam et al. reported that 6 of 16 patients (38%) experienced impaired abduction after hook plate fixation, but shoulder range of motion improved after removal of the hook plate (Ejam, Lind, and Falkenberg 2008). Similarly, Fosser et al. noted that 12 of 22 patients (54.5%) experienced a mechanical block to shoulder range of motion due to the hook plate (Fosser and Camporese 2021).
Athar et al. found that 4 of 17 patients (23.5%) experienced superficial infections (Athar et al. 2018). In 2008, Ejam et al. found that only one of 16 patients (6.3%) experienced a superficial wound infection (Ejam, Lind, and Falkenberg 2008). Conversely, Şișman et al. noted that 2 of 62 patients (3.2%) experienced superficial wound infections (Şişman et al. 2022). Similar findings were reported by Turgut et al. as 2 of 30 patients (6.6%) in their study had superficial wound infections as a complication of hook plate fixation (Turgut et al. 2022). Additionally, Fosser et al. reported one (4.5%) perioperative fracture of the clavicle (Fosser and Camporese 2021) and Yapici et al. reported one patient (4.5%) who experienced an implant failure due to breakage of the hook plate (Yapici 2021).
Hook Plate with Augmentation
The two studies that evaluated hook plate fixation with augmentation specifically evaluated hook plate fixation with ligament suturing and hook plate fixation with suture anchors (Salem and Schmelz 2009; Sheu et al. 2023). Across these studies, there were 46 total patients. In 2022, Sheu et al. compared the use of a hook plate alone, hook plate augmented with a suture anchor, and arthroscopically assisted tightrope fixation in patients with acute Type V AC joint dislocations (Shen et al. 2021). In this study, 22 of 71 patients (15 male; 7 female, 31%), underwent hook plate fixation alone, 23 underwent hook plate fixation with suture anchor augmentation (18 male; 5 female, 32.4%), and 26 (20 male; 6 female, 36.6%) underwent arthroscopically assisted tightrope fixation. Four (15.4%) patients in the tightrope group had loss of reduction at 3-month follow-up. One (4.3%) patient in the hook plate with augmentation group and 8 (30.8%) in the tightrope group demonstrated loss of reduction at 2-year follow-up (Sheu et al. 2023). In 2009, Salem et al. evaluated the treatment of Rockwood type III-V AC joint injuries using hook plates augmented with ligament sutures (Salem and Schmelz 2009). This study included 25 patients (23 males; 2 females, 92%), with 2 of the patients being lost to follow-up. On follow-up radiographs, minor joint asymmetry was seen in 5 cases (21.7%). Loss of reduction with more than 50% joint separation occurred in 3 (13%) patients after hook plate removal (Salem and Schmelz 2009).
In addition, there were no cases of osteitis, but Salem et al. reported 3 (13%) cases of superficial wound infection that were treated with local debridement and antibiotics (Salem and Schmelz 2009). Loss of reduction was a common complication, occurring in 4 (8.7%) patients across both studies (Salem and Schmelz 2009; Sheu et al. 2023). Other complications noted in this cohort including shoulder pain, discomfort, or paresthesias in 7 (15.2%) patients, and mild localized calcification of the coracoclavicular (CC) ligament in 5 (10.9%) patients (Salem and Schmelz 2009; Sheu et al. 2023). A summary of common complications across included studies can be seen in Table 3.
Discussion
We found that the most common complications following hook plate fixation of the AC joint are erosion of the acromion, osteolysis, loss of fixation, and infection. Our hypothesis that hook plate fixation for AC joint injuries has a wide range of potential complications with variable complication rates was supported by our results.
The results of this study show high levels of variation with regards to complication rates post-operatively after hook plate fixation with and without augmentation. Similar findings were observed in a 2022 systematic review and meta-analysis by Lee et al. that included 474 patients and demonstrated that coracoclavicular augmentation in combination with hook plate fixation resulted in maintenance of reduction of the AC joint after hook plate removal and subsequently had a 73% lower risk of acromial osteolysis (Lee et al. 2022). It is important to consider that hook plate fixation is typically followed by a second procedure to remove the hook plate that is equally invasive as hook plate placement, which likely contributes to the subsequently variable complication rates post-operatively (Metzlaff et al. 2016; Arirachakaran et al. 2017; Liu et al. 2018).
In addition, a 2021 retrospective study by Shih et al. including 67 patients found that patients with acute AC joint dislocation graded as either Rockwood type III or type IV who were treated with hook plate fixation with concomitant coracoclavicular suture anchor augmentation had significantly fewer residual subluxation events compared to patients who received isolated hook plate fixation (Shih et al. 2021).
We found that subacromial osteolysis was more likely to occur after hook plate fixation whereas complications such as loss of reduction and recurrence of deformity were more likely with other fixation techniques, such as tight rope. However, a 2021 systematic review and meta-analysis by Qi et al. demonstrated that in the context of acute acromioclavicular joint dislocation, patients who undergo fixation with tight-rope technique report less post-operative pain without significant increases in operative time, coracoclavicular distance, or risk of reduction loss compared to patients who underwent fixation with clavicular hook plate (Qi et al. 2021). Additionally, a 2018 prospective case-control study conducted by Razak et al. that included 16 patients who underwent tight rope fixation and 10 patients who underwent standard hook plate fixation found that the tight rope cohort had no complications, while the hook plate cohort had three (18.8%) complications including one hook plate cut out, one isolated acromial erosion, and one acromial erosion with a tip fracture that was treated with tension band wiring (Bin Abd Razak et al. 2018). Although this difference in complication rate is statistically significant, it is important to note the small sample size of patients included in this study (Bin Abd Razak et al. 2018). Furthermore, a 2017 systematic review and meta-analysis conducted by Arirachakaran et al. found that unstable acromioclavicular joint dislocations treated with loop suspensory fixation have higher subjective patient reported outcome scores and lower post-operative pain scores compared to hook plate fixation; however, they also reported that higher overall complication rates are observed with loop suspensory fixation compared to hook plate fixation (Arirachakaran et al. 2017). The contradictory findings between our study and prior literature shows that there does not presently exist a gold standard for treatment of acromioclavicular joint dislocation in terms of using hook plate fixation or tight rope.
Limitations
This study is not without limitations. First, the study is limited by the relatively small sample sizes and retrospective design of many of the included studies. Additionally, there is a paucity of data regarding patient reported outcome measures (PROMs), and we were unable to stratify complications data based on patients’ activity level, level of sport, or mechanism of injury. Each of these factors are important in surgical consideration and can affect the treatment option selected. Furthermore, given that only two included studies evaluated complications after hook plate fixation with augmentation, we were unable to make any definitive conclusions regarding complication rates. Another limitation that is inherent to all systematic reviews is the exclusion of potential studies with relevant data, such as studies not written in the English language. Due to the heterogeneity of data and resulting difficulty in associating complications, outcomes, and patient factors, future prospective randomized controlled trials should be performed on patients with AC joint injuries to improve understanding of specific risk factors and how they can be mitigated to avoid complications in the setting of hook plate fixation.
Conclusions
Hook plate fixation for AC joint injuries is associated with high variation in subsequent complications. Common complications include subacromial osteolysis, loss of fixation, infection, and pain. Hook plate fixation augmented with coracoclavicular ligament tape or loop suspensory reconstruction may help lower rates of subacromial osteolysis and improve short-term functional outcome measures postoperatively. Both patients and surgeons should be aware of the complications that can occur with the use of hook plates for AC joint injuries.