INTRODUCTION
Meniscal injuries represent the most common indication for arthroscopic knee surgery (Thompson 2016). Due to the high frequency of meniscal procedures performed, quantifying subjective patient reported outcomes is necessary to validate the benefit to patients undergoing meniscal procedures based on postoperative improvement. Increased use of patient-reported outcome measures (PROMs) reflects this desire for numerical data (Mosher, Ewing, Collins, et al. 2020), as numerous PROMs are utilized to define outcomes following meniscal surgery, each offering different advantages (Harris et al. 2017). Commonly reported PROMs include the Knee Injury and Osteoarthritis Outcome Score (KOOS), International Knee Documentation Committee (IKDC), Lysholm Knee Questionnaire, and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (Siljander et al. 2018). Due to the heterogeneity inherent within the currently available PROMs, determining the clinical significance associated with changes in scores following surgery remains challenging (Mabrouk, Nwachukwu, Pareek, et al. 2023).
To address this challenge, additional outcome tools have been introduced to aid in the clinical interpretation of PROMs. Three of the commonly used tools to assess clinically significant outcomes (CSOs) are the minimal clinically important difference (MCID), substantial clinical benefit (SCB) and patient acceptable symptomatic state (PASS) (Migliorini et al. 2024; Mowers et al. 2025; Childers, Lack, Mowers, et al. 2025). MCID aims to detect the smallest change in postoperative outcomes that reaches clinical significance; PASS is used to determine the minimal outcome required for patient satisfaction; while SCB seeks to quantify substantial improvement from preoperative status (Lubowitz, Brand, and Rossi 2019). While CSOs are intended to increase the standardization of PROM interpretation, recent studies have noted variability in the literature when calculating these measures (A. C. Lee et al. 2024; Kolin, Moverman, Pagani, et al. 2022; Deckey, Verhey, Christopher, et al. 2023). Namely, CSO can be calculated using a variety of different methods, grouped into either an anchor-based versus distribution-based approach (Franceschini et al. 2023). When using an anchor-based methodology, an anchor question is chosen as an adjunct to the PROM, intended to define level of improvement following surgery (Mabrouk, Nwachukwu, Pareek, et al. 2023). These anchors are then used to create a receiver operating characteristics (ROC) curve to calculate threshold values that guide determination of clinically significant changes (Maldonado et al. 2023). Distribution-based methods utilize a strong statistical basis; often using standard error of the mean (SEM), one half of a standard deviation (0.5 SD), or the effect size to determine a threshold value (Franceschini et al. 2023).
Prior studies reporting on a variety of orthopaedic procedures, including rotator cuff repair and joint arthroplasty (Migliorini et al. 2024; Kolin, Moverman, Pagani, et al. 2022; Deckey, Verhey, Christopher, et al. 2023) have reported substantial variety in the reporting of PROMs and calculation of CSOs. The purpose of this review was to systematically review the reporting of CSOs thresholds and methods for calculating thresholds following meniscal debridement, repair and allograft transplantation. The authors hypothesized a high degree of heterogeneity in the reported PROMs following meniscal procedures, with the majority of CSO calculated using anchor or distribution-based methods.
METHODS
Search Strategy and Eligibility Criteria
A systematic review of the existing literature following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Page, McKenzie, Bossuyt, et al. 2021) was performed using the PubMed, Embase, and SCOPUS online databases examining articles published from January 1, 2010 to April 25, 2024. Inclusion criteria consisted of Level I-IV studies published in English language reporting on patients undergoing meniscal procedures (debridement, repair and/or meniscal allograft transplantation [MAT]) with minimum 12-month follow-up and MCID, PASS, or SCB were included. Exclusion criteria included abstracts, case reports, biomechanical or technical reports, articles not written in English language or without English translation, animal studies, cadaveric studies, review articles and editorial articles.
The following Medical Subject Headings (MeSH) was used: (((“Meniscus” or “meniscal”) or OR “meniscectomy”) or (“Knee” AND (“Arthroscopy” OR “Arthroscopic”))) AND (“MCID” OR “minimally clinically important difference” or “SCB” or “substantial clinical benefit” or “PASS” OR “patient acceptability symptom state” OR “patient acceptable symptom state” OR “Clinically significant outcomes”). Title and abstract screening were completed by two independent authors (*initials blinded for peer-review*); any studies meeting initial criteria were considered for full-text screening. No disagreements between the two authors were encountered. Any duplicate studies were removed during the screening process.
Data Extraction
Upon completion of full-text screening, Microsoft Excel version 16.63 (Microsoft Corp., Redmond, WA, USA) was used to conduct data extraction, which included the CSOs reported for each individual PROM threshold, as well as the method (anchor -based, distribution-based, other) used to calculate each threshold. The method and approach used to calculate each CSO was recorded for both studies that calculated their own values and studies that extracted their values from the previous literature. In studies that did not calculate their own values, the method and approach was either directly reported, able to be deduced directly via their methods section, or determined through analysis of the studies they cited. Study demographics, including publication year, mean follow-up time, and number of patients reported, were also collected.
Risk of Bias Assessment
A methodological quality assessment was performed using the Methodological Index for Non-Randomized Studies (MINORS) criteria (Slim et al. 2003) by two independent authors (*initials blinded for peer-review*). The MINORS criteria is a numerical scale consisting of 8 questions for non-comparative studies and 12 questions for comparative studies with each question scored as the following: 0 if not reported, 1 if reported but inadequate, or 2 if reported and adequate. The highest achievable score for a non-comparative, non-randomized study meeting all criteria is 16, while the highest achievable score for a comparative, non-randomized study is 24. If a score difference ≥ 2 was encountered for any study between the two authors, a third author (*initials blinded for peer review) was consulted. No score difference ≥ 2 was recorded between the two authors.
Statistical Analysis
Due to the low level of evidence and lack of homogeneity amongst the studies included, data was not pooled, necessitating a descriptive analysis. Microsoft Excel version 16.63 (Microsoft Corp., Redmond, WA, USA) was used to calculate descriptive variables such as mean, median, and range.
RESULTS
Study Demographics
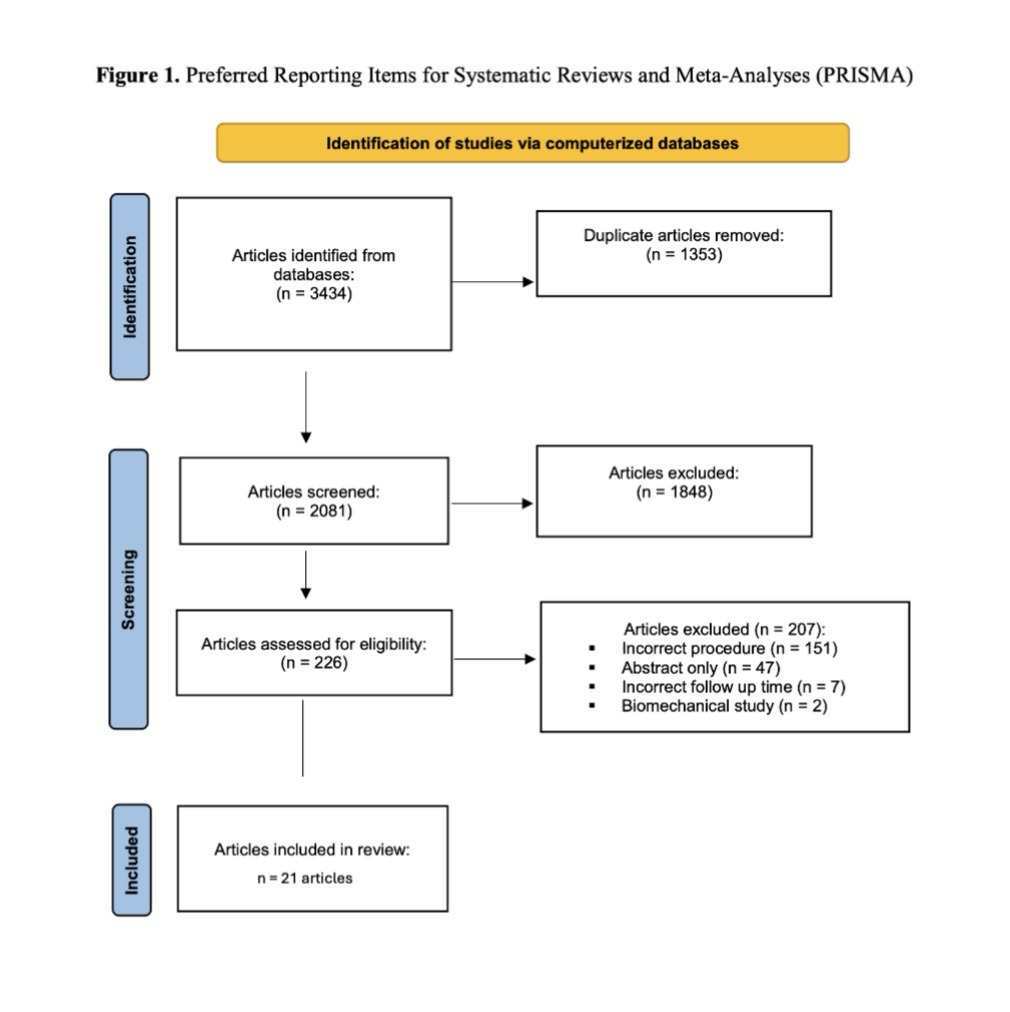
A total of 3434 studies were identified following abstract screening, of which 1353 duplicates were removed. The remaining 2081 abstracts were screened, of which 227 were eligible for full-text review. Following this, 21 studies (Aavikko et al. 2023; Beletsky, Gowd, Liu, et al. 2020; Bisson, Kluczynski, Wind, et al. 2022a; Dwyer et al. 2020; Grassi, Macchiarola, Lucidi, et al. 2020; Herber et al. 2024; Huddleston, Polce, Gilat, et al. 2022; Ingelsrud et al. 2023; Liu, Gowd, Redondo, et al. 2019; Lowenstein, Chang, Mass, et al. 2024; Maheshwer, Wong, Polce, et al. 2021; Massey, Sampognaro, Starnes, et al. 2023; Muench, Achtnich, Krivec, et al. 2022; Shekhar, Tapasvi, and Williams 2022; Therrien, Langhans, Lamba, et al. 2023; Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024; Zhang, Zhang, Jiang, et al. 2024; Jones, Gottreich, Jin, et al. 2024; Kurzweil, Krych, Anz, et al. 2021) reporting on 3110 patients undergoing meniscal procedures of the knee met inclusion criteria (Table 1, Figure 1). Level of Evidence (LOE) of the studies included Level II (2/21, 9.5%), III (9/21, 42.9%), and IV (10/21, 47.6%). Mean follow-up time, when reported, was 85.1 months (range, 12-120 months). All studies reported on CSOs postoperatively, with nine studies (9/21, 42.9%) reporting on outcomes following meniscal repair, seven studies (7/21, 33.3%) following MAT, and five studies (5/21, 23.8%) following partial meniscectomy. The mean MINORS score was 11.7 (range, 10-13) for non-comparative studies and 19.1 (range, 17-21) for comparative studies (Appendix 1).
.png)
Patient-Reported Outcome Measures
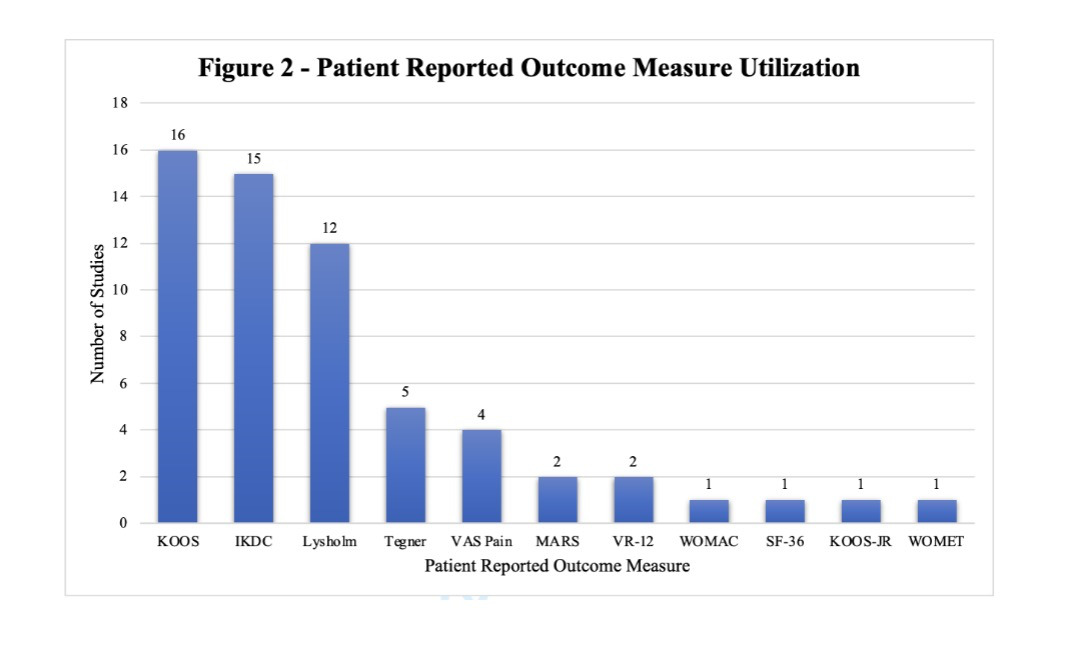
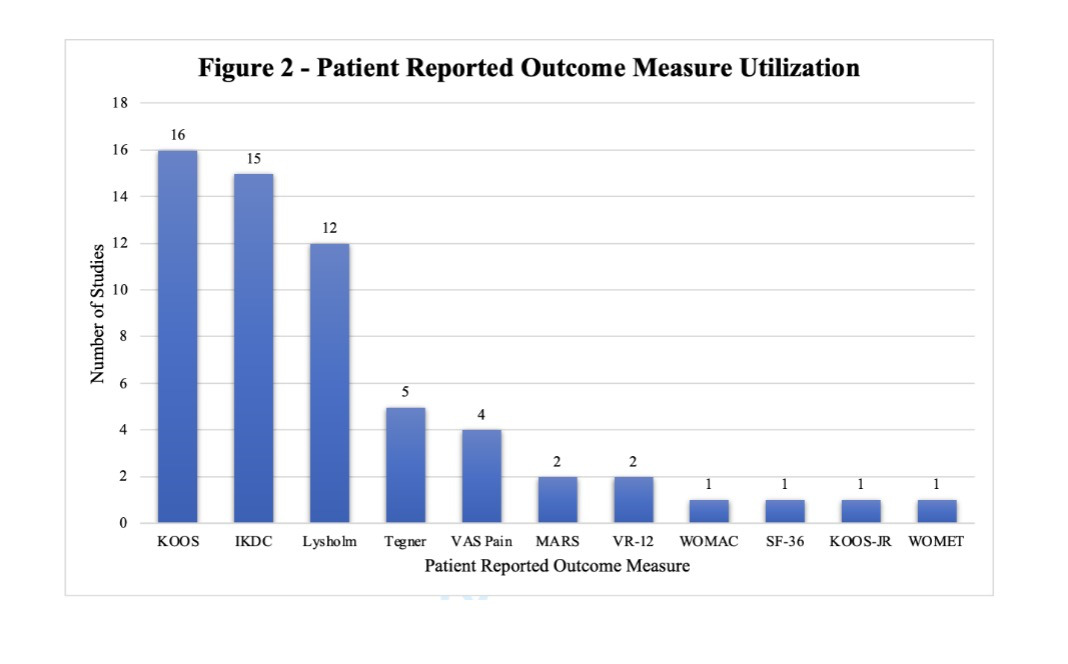
Eleven different PROMs were reported, with the most common being KOOS (16, 76.2%), followed by IKDC (15, 71.4%) (Figure 2).
Clinically Significant Outcomes
MCID and PASS were the most commonly reported CSOs, each reported in 15 studies (71.4%), while SCB was reported in five studies (23.8%). One study (Ingelsrud et al. 2023) (4.8%) reported minimal important change (MIC) and treatment failure (TF) thresholds.
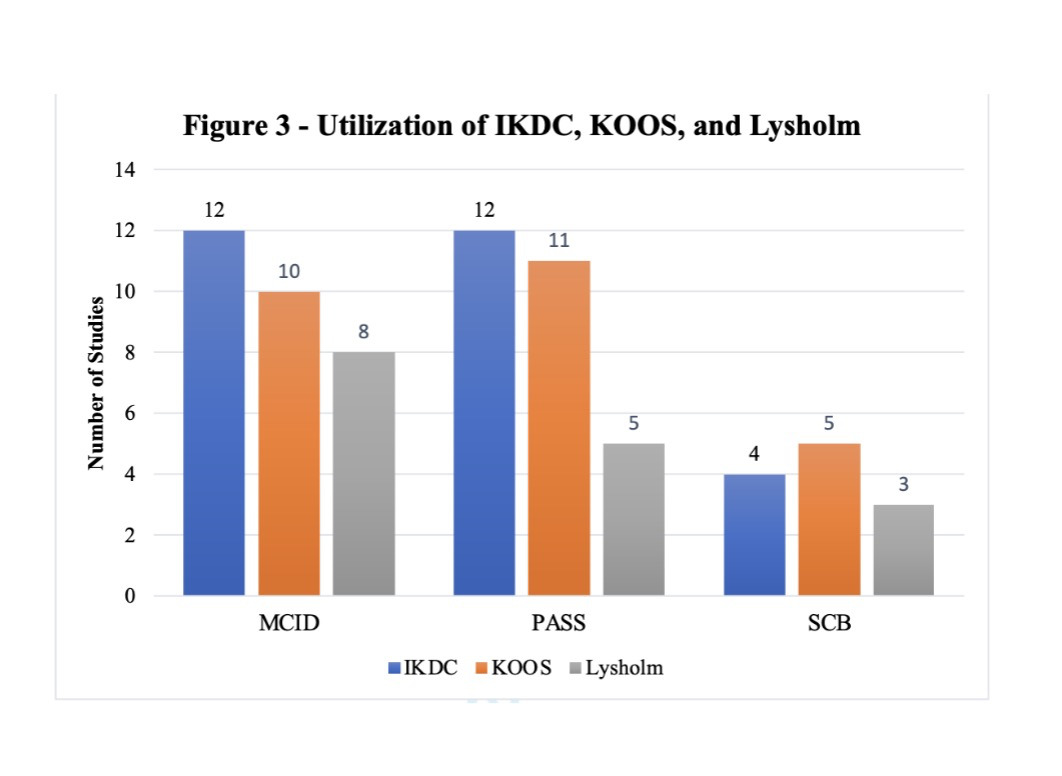
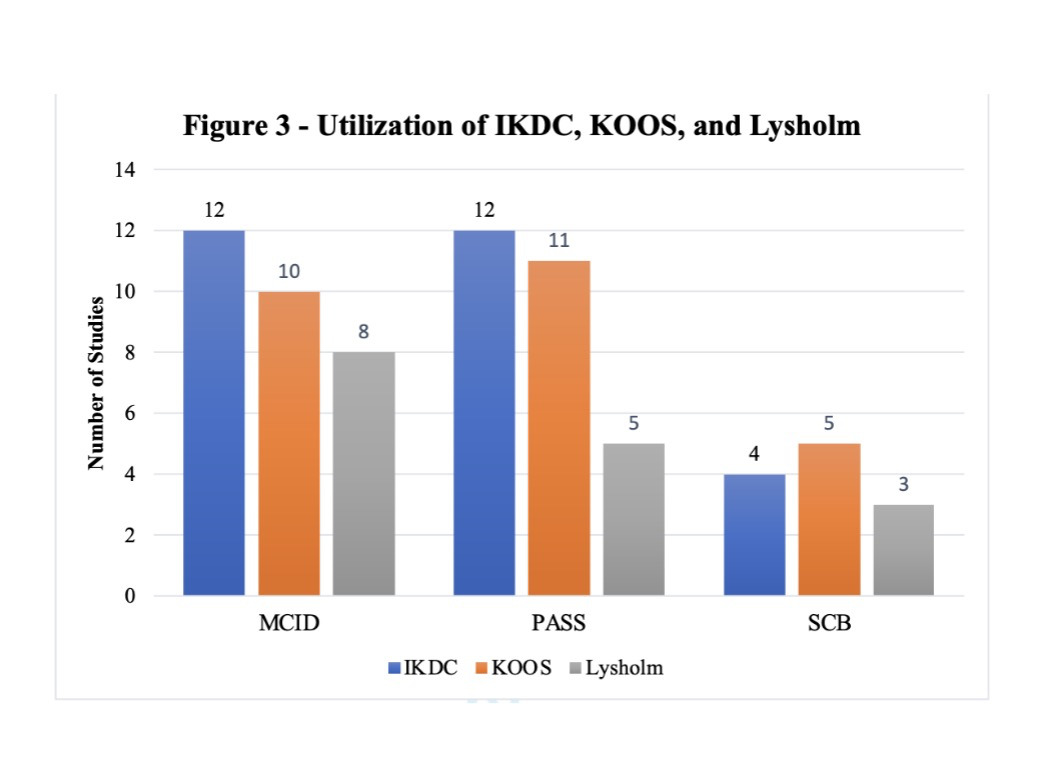
In studies reporting MCID, IKDC was the most commonly utilized PROM, with 12 studies (12/15, 80.0%) reporting thresholds for IKDC, followed by KOOS (10/15, 66.7%) and Lysholm score (8/15, 53.3%) (Figure 3). In studies reporting PASS, 12 studies utilized IKDC (12/15, 80.0%), while 11 (11/15, 73.3%) reported on KOOS, and 5 (5/15, 33.3%) used Lysholm. KOOS was the most frequently utilized PROM for SCB, reported in five studies (5/5, 100%), followed by IKDC (4/5, 80%) and Lysholm (3/5, 60%). MIC and TF were reported utilizing KOOS in a single study (Ingelsrud et al. 2023).
Methods of Calculation
Nine studies (9/15, 60.0%) calculated original MCID thresholds, while six studies (6/15, 40.0%) referenced previously published values. All nine studies performing original calculations utilized one-half of the standard deviation of the mean change of the PROM of interest (9/15, 60.0%). Of the 15 studies reporting PASS, nine (9/15, 60.0%) performed original calculations, with the most common method being ROC analysis maximizing the Youden index (6/15, 40.0%). Adjusted predictive modeling was performed in two studies (2/15, 13.3%), while ROC curve analysis was reported in one study (1/15, 6.7%). The remaining six studies (6/15, 40.0%) reporting PASS referenced previously cited literature to determine threshold values. Of the five studies reporting SCB, four (4/5, 80%) performed original calculations, all of which utilized the ROC-Youden Index method. One study (1/5, 20%) reporting SCB referenced previously cited literature for threshold values. The lone study reporting MIC and TF used adjusted predictive modeling for calculation.
Frequently Cited Thresholds
Of the 21 included studies, 17 referenced previously published literature, either for the purpose of using established CSO thresholds, or to credit their method of calculation. There were 12 unique studies referenced, with two (Liu, Gowd, Redondo, et al. 2019; Maheshwer, Wong, Polce, et al. 2021) of these being cited by at least two other studies for the purpose of referencing threshold values. Instances of citation, reference threshold values, and methods of calculation can be found in Table 2.
Anchor Questions
Of the 21 included studies, 10 (10/21, 47.6%) used an anchor question to assess patient outcomes. Studies reporting PASS most commonly utilized an anchor question, (n=10/15, 60.0%). Four (4/5, 80%) studies reporting SCB used an anchor question, compared to only three (3/15, 20.0%) studies reporting MCID. Binary (yes/no) questions were the most common, with all 10 of the studies reporting an anchor question using this type. Two studies (Beletsky, Gowd, Liu, et al. 2020; Maheshwer, Wong, Polce, et al. 2021) reported using two anchor questions: one binary and one Likert scale with 15-point values. There were six unique anchor questions implemented, the most common of which being: “Taking into account all activities you have done during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?”, utilized in four studies. Two studies (Beletsky, Gowd, Liu, et al. 2020; Maheshwer, Wong, Polce, et al. 2021) reported a Likert scale question that asked their patients: “Since your surgery, has there been any change in the pain in your knee?”, and provided 15 total options, ranging from -7 to +7.
Stratification by Procedure Type
Meniscal Repair
Of the nine studies reporting outcomes in patients undergoing meniscal repair, six (66.7%) reported MCID (Herber et al. 2024; Maheshwer, Wong, Polce, et al. 2021; Massey, Sampognaro, Starnes, et al. 2023; Shekhar, Tapasvi, and Williams 2022; Zhang, Zhang, Jiang, et al. 2024; Kurzweil, Krych, Anz, et al. 2021) and six (66.7%) reported PASS (Herber et al. 2024; Ingelsrud et al. 2023; Maheshwer, Wong, Polce, et al. 2021; Massey, Sampognaro, Starnes, et al. 2023; Muench, Achtnich, Krivec, et al. 2022; Therrien, Langhans, Lamba, et al. 2023). Of the six studies reporting MCID, three (Maheshwer, Wong, Polce, et al. 2021; Massey, Sampognaro, Starnes, et al. 2023; Zhang, Zhang, Jiang, et al. 2024) (50.0%) utilized one-half of the standard deviation of the mean change of the PROM of interest and three (Herber et al. 2024; Shekhar, Tapasvi, and Williams 2022; Kurzweil, Krych, Anz, et al. 2021) (50.0%) referenced previously reported thresholds. Studies reporting PASS most frequently used previously determined thresholds (Herber et al. 2024; Massey, Sampognaro, Starnes, et al. 2023; Muench, Achtnich, Krivec, et al. 2022; Therrien, Langhans, Lamba, et al. 2023) (4/6, 66.7%), followed by ROC-Youden index (Maheshwer, Wong, Polce, et al. 2021) (1/6, 16.7%) and adjusted predictive modeling (Ingelsrud et al. 2023) (1/6, 16.7%).
Meniscal Allograft Transplant
The MCID (Aavikko et al. 2023; Huddleston, Polce, Gilat, et al. 2022; Liu, Gowd, Redondo, et al. 2019; Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024) and PASS (Grassi, Macchiarola, Lucidi, et al. 2020; Huddleston, Polce, Gilat, et al. 2022; Liu, Gowd, Redondo, et al. 2019; Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024) were each reported in six of the seven (85.7%) studies reporting on MAT, while SCB (Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024) was reported in three (42.9%) studies. Of the six studies reporting MCID, four (Liu, Gowd, Redondo, et al. 2019; Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024) (66.7%) utilized one-half of the standard deviation of the mean change, while two (Aavikko et al. 2023; Huddleston, Polce, Gilat, et al. 2022) (33.3%) referenced previously determined thresholds. PASS was calculated using ROC-Youden index in four (Liu, Gowd, Redondo, et al. 2019; Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024) of the six (66.7%) studies, while previously referenced thresholds were in the remaining two studies (Grassi, Macchiarola, Lucidi, et al. 2020; Huddleston, Polce, Gilat, et al. 2022) (33.3%). All three (Wagner, Kaiser, Knapik, et al. 2023; Wagner, Kaiser, Quigley, et al. 2024; Wagner, Horner, Gilat, et al. 2024) studies reporting SCB used the ROC-Youden index.
Partial Meniscectomy
Of the five studies reporting outcomes following partial meniscectomy, three (60.0%) reported MCID (Beletsky, Gowd, Liu, et al. 2020; Bisson, Kluczynski, Wind, et al. 2022a; Lowenstein, Chang, Mass, et al. 2024; Bisson, Kluczynski, Wind, et al. 2022b), three (60.0%) reported PASS (Beletsky, Gowd, Liu, et al. 2020; Dwyer et al. 2020; Jones, Gottreich, Jin, et al. 2024), and two (40.0%) reported SCB (Beletsky, Gowd, Liu, et al. 2020; Lowenstein, Chang, Mass, et al. 2024). MCID was calculated in two (Beletsky, Gowd, Liu, et al. 2020; Bisson, Kluczynski, Wind, et al. 2022a) studies (2/3, 66.7%) using one-half of the standard deviation of the mean change, with one (Lowenstein, Chang, Mass, et al. 2024) study (1/3, 33.3%) using previously determined thresholds. PASS was determined in one study each using ROC-Youden index (Beletsky, Gowd, Liu, et al. 2020), adjusted predictive modeling (Jones, Gottreich, Jin, et al. 2024), and ROC curve analysis (Dwyer et al. 2020). Of the two studies reporting SCB, thresholds were calculated using the ROC-Youden index (Beletsky, Gowd, Liu, et al. 2020) and previously determined thresholds (Lowenstein, Chang, Mass, et al. 2024).
DISCUSSION
The primary findings from this study include the substantial variability present in the reporting of CSOs and methods for calculating CSO threshold following meniscal procedures. Anchor-based and distribution-based methodology for calculating CSOs offer alternative methods of obtaining CSO thresholds with neither exclusively preferred by currently published studies. MCID and PASS were frequently reported when compared to SCB. IKDC, KOOS, and Lysholm were commonly utilized PROMs, demonstrating a potential preference following meniscal procedures.
When two studies report CSOs on similar patient cohorts, a large degree of variation in findings may contribute to the inconsistency of CSO reporting. Two studies in this review reported on outcomes following partial meniscectomy, both using distribution-based calculation methods to determine the MCID for KOOS subscales. Beletsky et al (Beletsky, Gowd, Liu, et al. 2020). reported on patients following isolated partial meniscectomy. Using one-half of the standard deviation of the mean change, the authors found MCID thresholds for each KOOS subscale. Similarly, Bisson et al (Bisson, Kluczynski, Wind, et al. 2022a). investigated patients undergoing partial meniscectomy in which 71 knees had unstable chondral lesions at the time of surgery, while no chondral lesions were reported in 47 patients. Despite using the calculation method employed by Beletsky et al., the authors reported lower MCID values for nearly all KOOS subscales for both cohorts. When comparing data from Beletsky et al. to Bisson et al. in which no chondral lesion were encountered, mean age (48.9 vs. 50.2 years, respectively) and BMI (25.9 vs 27.3, respectively) were similar, yet MCID thresholds differed substantially, most notably in the KOOS-QOL subscale (15.6 vs. 11.0, respectively). This level of variance among two cohorts of similar demographic makeup suggests that distribution-based methods may lead to the incongruence of CSO threshold calculation, contributing to the inconsistency of reporting in the literature.
Of the 15 studies reporting PASS thresholds, 10 utilized an anchor question. Anchor-based methodology is considered to better reflect change in clinical status compared to distribution-based methods and is generally preferred, when feasible (A. C. Lee et al. 2024). While more cumbersome to administer than distribution-based methods, anchor-based methods have been reported to yield results more reflective of the level of the patient (Copay et al. 2007). Anchor-based methods rely on the use of a specifically chosen question as an adjunct to PROM data. These questions can exist either as a binary query or are rated on a Likert scale, presenting patients with a multitude of options across the spectrum of outcomes. Notably, all nine studies in this review that utilized an anchor question opted for binary answer choices; while only two studies (Beletsky, Gowd, Liu, et al. 2020; Maheshwer, Wong, Polce, et al. 2021) chose to supplement this with a follow-up question graded on a Likert scale. Use of binary questions has been reported to inflate the MCID, placing patients into categories not fully representative of their level of function and satisfaction (Revicki et al. 2008). As such, anchor questions should be chosen based on the population of interest, which can be done by creating domain-specific questions. Specifically, Ward et al (Ward, Guthrie, and Alba 2015). demonstrated that domain-specific questions increase construct validity in the determination of clinical significance. With little exception, studies included in this review used global, nonspecific anchor questions to support CSO calculations, increasing the opportunity for variance in CSO reporting due to the heterogeneity in the reference populations.
Two studies (Liu, Gowd, Redondo, et al. 2019; Maheshwer, Wong, Polce, et al. 2021) reported CSO threshold values which were subsequently cited by other included studies. Liu et al (Liu, Gowd, Redondo, et al. 2019)., cited by two included studies (Grassi, Macchiarola, Lucidi, et al. 2020; Huddleston, Polce, Gilat, et al. 2022), reported MCID and PASS thresholds using half of the standard deviation of the mean change and the ROC-Youden Index, respectively. Meanwhile, Maheshwer et al (Maheshwer, Wong, Polce, et al. 2021). was cited by three (Herber et al. 2024; Massey, Sampognaro, Starnes, et al. 2023; Muench, Achtnich, Krivec, et al. 2022) other included studies. The authors reported MCID and PASS thresholds following arthroscopic meniscal repair at a follow-up of two years. Distribution-based methods were used for the calculation of both MCID and PASS for IKDC, while the ROC-Youden Index and two anchor questions were used for KOOS values. The use of previously established thresholds may have the potential to bring standardization to the reporting of CSOs. Namely, highly cited studies, specific to procedure and population, may serve as landmarks for future publications to reference as opposed to original calculation methods. This has the potential to reduce the workload of authors seeking to publish CSO while standardizing the reporting of CSO thresholds. However, this practice is not without disadvantages. When using established threshold values, it is important to consider both procedure and population of interest, as it has been reported that there is a significant, potentially detrimental practice in orthopedic literature of reusing CSO values across different procedure types, geographic locations, and timeframes (Wellington, Davey, Cote, et al. 2023). One study (Aavikko et al. 2023) reporting on outcomes following MAT co-opted MCID threshold values from Berliner et al (Berliner et al. 2017)., a publication in which the authors established thresholds based on a cohort of patients undergoing total knee arthroplasty. The cross-procedural use of CSO cutoffs may contribute to inaccurate and inconsistent reporting of clinical significance. As such, it is plausible that standardized CSO values may show appreciable clinical benefit only if they are highly specific to the procedure and the patient population being evaluated.
When comparing utilization of CSOs, MCID and PASS were both reported in 15 out of 21 studies (71.4%), while SCB was reported in only five studies, with no study reporting SCB in isolation. This is consistent with previous studies reporting CSOs following knee arthroplasty, in which SCB is infrequently reported (Migliorini et al. 2024). As SCB is based on the achievement of substantial benefit to the patient, beyond just the minimum clinically recognized improvement (Glassman et al. 2008), the benefit of SCB over other CSOs lies in its ability to determine cutoffs for meaningful outcomes. However, a lack of consensus in reporting protocol has led to inconsistent implementation of SCB in the current literature.
When stratified based on procedure type (debridement, repair, transplant), comparable rates of MCID and PASS reporting were appreciated. This suggests that trends in CSO reporting may not be procedure-specific, but rather representative of studies reporting CSO following the management of meniscal injuries as a whole. However, heterogeneity existed when comparing methods of CSO calculation between procedures. Studies reporting on PASS for meniscal repairs preferentially used previously determined thresholds (66.7%), compared with only 33.3% of studies following MAT and none for partial meniscectomy. One possible explanation for this is that meniscal repairs tend to have longer lasting benefits (Stein et al. 2010) making it easier for authors to use established PASS thresholds. In a partial meniscectomy, results are more short-lived (W. Q. Lee, Gan, and Lie 2019) and a greater interpopulation variability may lead authors to shy away from utilizing previously established thresholds. Authors should consider the previously discussed advantages and disadvantages when selecting method for CSO calculation. Efforts to standardize the calculation and reporting of CSOs, as well as increased use of anchor-based calculation methodology, may serve to emphasize the clinical importance and ease of use when evaluating outcomes following specific procedures. Namely, authors should drive to calculate unique CSO’s for their own specific patient populations and procedures and avoid adopting generalized values provided by previous researchers and use specific language when describing their calculation methodology and justification. This will allow for more standardized comparisons between varying groups. Ultimately, the orthopaedic community can do a better job in capturing CSOs for one of the most common procedures we perform.
Limitations
This study was not without limitations, as the findings of this review must be interpreted in the context of its limitations. Due to the small sample size, secondary to the strict inclusion/exclusion criteria utilized, the overall level of evidence of the included studies was low, while data pooling and meta-analysis were not performed. Subgroup analysis of meniscal allograft transplant studies was limited due to the majority of these studies coming from the same institution, leading to a potential bias. The extent of meniscal debridement, type of meniscal repair, and the performance of concomitant procedure during MAT were not uniform and thus, the impact of meniscal tear severity and potential concurrent pathologies could not be evaluated, potentially leading to further bias in the interpretation of the results.
Substantial variability exists in the reporting and calculation of MCID, SCB, and PASS for various PROMs following meniscal debridement, repair and allograft transplantation. This heterogeneity may hinder the interpretive utility of such measures. As such, authors should strive to derive CSO values specific to their patient population at hand using anchor-based methods if possible.
Abbreviations
PROMs, patient-reported outcome measures; KOOS, Knee Injury and Osteoarthritis Outcome Score; IKDC, International Knee Documentation Committee; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; CSOs, clinically significant outcomes; MCID, minimal clinically important difference; SCB, substantial clinical benefit; PASS, patient acceptable symptomatic state; ROC, receiver operating characteristic; SEM, standard error of the mean; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; MAT, meniscal allograft transplant; MeSH, medical subject headings; MINORS, Methodological Index for Non-Randomized Studies; LOE, level of evidence; MIC, minimal important change; TF, treatment failure; SD, standard deviation; VAS, Visual Analog Scale; VR-12, Veterans Rand; MARS, Marx Activity Rating Scale; SF-36, 36-item Short Form Health Survey; KOOS JR, Knee Injury Osteoarthritis Outcomes Survey Joint Replacement; WOMET, Western Ontario Meniscal Evaluation Tool; KOOS-QL, Knee Injury and Osteoarthritis Outcome Score – Quality of Life.