Introduction
Arthroscopic repair of rotator cuff tears (RCTs) has become the gold standard of treatment for rotator cuff injuries. From 2004 to 2009 alone, the percentage of RCTs repaired arthroscopically increased from 48.8% to 74.3%, while the percentage repaired via open techniques decreased from 51.2% to 25.7% (Zhang et al. 2013). Widespread adoption of the arthroscopic approach has driven the demand for new surgical devices to aid surgeons in navigating the narrow subacromial space and tight shoulder margins (Dey Hazra et al. 2021). Antegrade suture passing devices were developed to assist surgeons in grasping the tendon tissue and passing the suture in one step, thus reducing operative time and improving movement efficiency within the narrow working space. However, the ability of the suture passer to penetrate the appropriate tissue depends on several factors, including RCT morphology, size, anatomical location, and tissue thickness (Chung et al. 2019). Because the complexity of RCTs varies significantly from shoulder to shoulder, intrinsic rotator cuff pathologies, such as delamination and deep surface tendon retraction, present a challenge for repairing these tears with a single, conventional method.
Review of RCT pathogenesis
Unique biomechanical and biological properties of the rotator cuff predispose the tendon to distinct injuries. RCTs can occur on the articular (deep) surface, the bursal (superficial) surface, or within the tendon intrasubstance (Ellman 1990; Walz et al. 2007). A specific type of tear that can present challenges with antegrade suture passers is known as the “delaminated tear” (J.-H. Kim and Lee 2023; Sonnabend et al. 2001). As defined by Kwon et al., delamination in full-thickness tears involves a discernable gap between the bursal and articular edges of the tendon, and in partial-thickness tears, retraction at either the bursal or articular surface with a discernable horizontal gap (Kwon et al. 2019). The rotator cuff tendon’s multilayered histological anatomy may predispose it to delaminated tears (J. H. Kim and Jung 2019).
In some instances, even without visible delamination, the deep fibers of the rotator cuff can retract to varying levels of severity, with the articular surface fibers often retracting more than the bursal surface fibers (Lee and Lee 2002). Larger tear size often correlates with greater degrees of retraction (Kandemir et al. 2010). Structural differences confirmed by biomechanical displacement-controlled studies demonstrate that the articular layer is more vulnerable to tensile load, while the bursal layer provides greater deformation and, consequently, tensile strength. This creates a shearing force during glenohumeral abduction between the layers, predisposing the rotator cuff to full delamination and the potential for deep layer retraction (Nakajima et al. 1994). The location can vary, but delamination more frequently occurs posteriorly rather than anteriorly (Clark and Harryman 1992; Han et al. 2013a; Tanaka et al. 2018). Further, Tanaka et al. found the presence of delamination to increase as the size of RCT increased from small tears (< 10mm) to large tears (≥ 30mm but < 50mm) (Tanaka et al. 2018).
Biomechanical forces distributed between several points, including the suture-tendon interface, impact the strength of arthroscopic RCT repair (Wlk et al. 2015). The ability of suture passers to optimally place sutures in the tendon is limited by the depth of the device jaws and the level of retraction of the deep layer of the rotator cuff. The suture passing device used in this study has a bite depth of 16mm, with most suture passing devices ranging between 16-22mm. This bite depth is sufficient for most rotator cuff morphology, but in RCTs with articular surface retraction, the suture passer jaws may not be deep enough to fully grasp both bursal and articular layers of the tendon, even when the jaws of the device are buried entirely into the lateral margin of the rotator cuff. We believe capturing and repairing the deeper articular layers when passing the suture through the tissue is significant as it allows the tendon to heal in an anatomical position by improving the tensile strength of the repair.
The purpose of this study was to investigate the rate at which antegrade suture passers successfully passed through both the articular and bursal layers of the rotator cuff in partial- and full-thickness tears at the anterior, middle, and posterior portions of the tendon during arthroscopic repair of rotator cuff tears. We hypothesized that RCTs < 20mm would demonstrate higher success rates than RCTs ≥ 20mm when repaired arthroscopically using a suture passer with a bite depth length of 16mm. Additionally, we hypothesized that sutures placed in the middle and anterior position with the suture passer would demonstrate higher rates of passing than those placed in the posterior position, and partial-thickness tears would demonstrate a higher rate of passing than full-thickness tears.
Materials and Methods
Study Design
From February 2023 to February 2024, a consecutive series of patients underwent arthroscopic repair for rotator cuff tears by a shoulder and elbow fellowship-trained surgeon at an outpatient surgery center. Institutional review board approval was obtained for the study protocol and chart review of patient data. Patients with partial or full-thickness rotator cuff tears who failed conservative treatment were identified as candidates for surgery and eligible for inclusion in the study. Patients with additional shoulder pathologies or revision surgery were excluded from the study.
Surgical Technique
All RCTs were repaired arthroscopically. The rotator cuff was visualized through a posterior-lateral viewing portal anterior to the posterolateral corner of the acromion. In the setting of partial-thickness tears of the rotator cuff, tendons were repaired using a full tendon “take-down” approach, rather than transtendinous repair. In all cases, the surgeon first mobilized the torn tendon and reduced it to the lateral side of the greater tuberosity, ensuring no significant tension on the repair. Depending on the morphology and size of the tear, between 1-4 medial row anchors were placed utilizing a double-row repair technique, attempting to maximize contact and pressure between the tendon-tuberosity interface while avoiding anchor overcrowding. The Expressew III Flexible Suture Passer (DePuy MiTek, Raynham, MA) was used to pass sutures through the rotator cuff tendon. A retrograde suture passer (SutureLAsso SD 90°, Arthrex, Naples, FL) was used to pass the suture only after the antegrade passer was not successful in passing the suture with optimal placement. After passing into the appropriate layer, the sutures were tied and brought into two lateral row anchors to complete the repair.
Device Performance Metrics
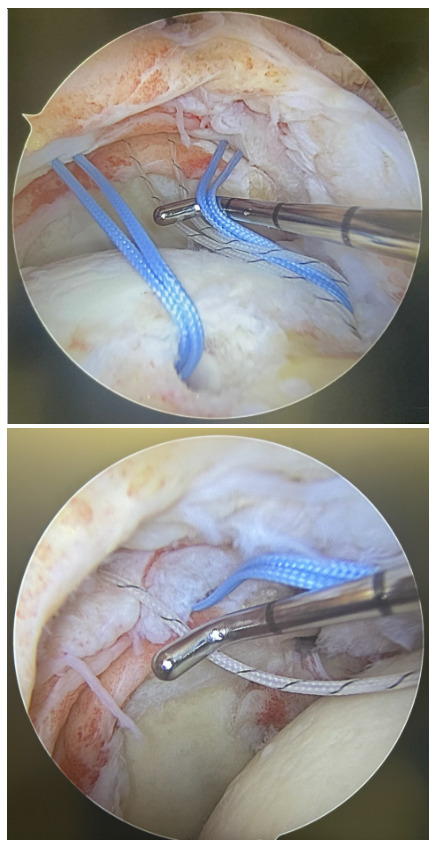
To evaluate the efficacy of the suture passer, explicit criteria were developed a priori to characterize the ability of the device to penetrate the desired tissue. All attempts were documented sequentially during surgery in real time. First, the surgeon attempted to place each suture using the antegrade suture passer through the rotator cuff by burying the device to the lateral border of the tendon and deploying the trigger to pass the suture. After passing each suture, the surgeon would then assess the placement of the suture to determine if it captured the appropriate layers of the rotator cuff. Optimal tendon penetration was defined as penetrating all layers of the rotator cuff tendon, including the articular and deeper bursal layers. If the device successfully passed the suture through the articular and bursal layers of the tendon, the attempt was recorded as a “success”. If the suture did not fully pass through the desired articular layer, only passing through the tendon and sparing the deeper capsular layers, the attempt was recorded as a “miss” (Figure 4). Whenever a “miss” was recorded, the suture was removed, and the surgeon then used the retrograde passer (Suture Lasso SD 90°, Arthrex, Naples, FL) to correctly place the suture through the desired tissue. If attempts to place subsequent sutures through the same rotator cuff using the antegrade suture passer were unfeasible due to tear morphology or limited access, the attempt was forgone, and the retrograde passer was used to manually place the suture. These attempts were recorded as “misses” to ensure systematic reporting.

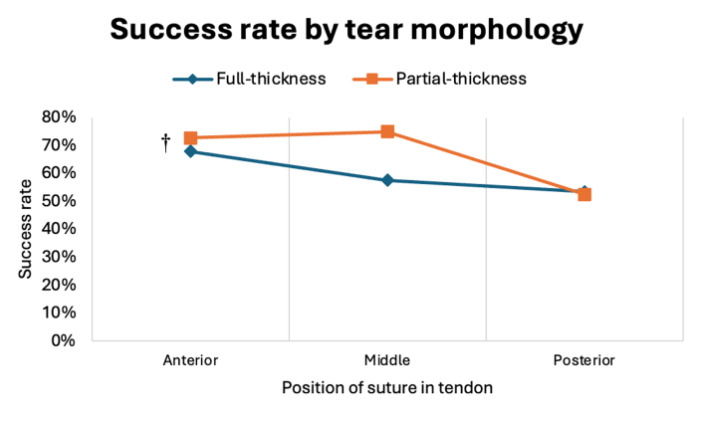
_than_partial-thickness_tears_(6.png)


For each rotator cuff repair, the antegrade suture passer success rate was calculated based off the number of successful passes through the tendon divided by the total number of attempts. Success rates were also calculated for the anterior, middle, and posterior portions of the rotator cuff as well as the overall rate of incorrectly placed (“missed”) in the rotator cuff. Success rates were compared across demographic factors (age and sex), tear morphology (partial-thickness vs. full-thickness), and tear size (< 20mm vs. ≥ 20mm). This cutoff was selected as it approximates the average rotator cuff tear size reported in the literature, allowing for balanced cohort sizes and meaningful comparison. Tear size was measured in the anteroposterior (AP) dimension using magnetic resonance imaging (MRI). The tear size was confirmed under arthroscopic examination.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics 29.0.1.1 (SPSS Inc., Armonk, NY, United States). Descriptive statistics were used to report demographic characteristics of the study population. Success rates were compared using the Kruskal-Wallis Test and Mann-Whitney U Test, with significance set at p<0.05 and a 95% CI. Significance reported for the Kruskal-Wallis Test was adjusted by the Bonferroni correction for multiple comparisons.
Results
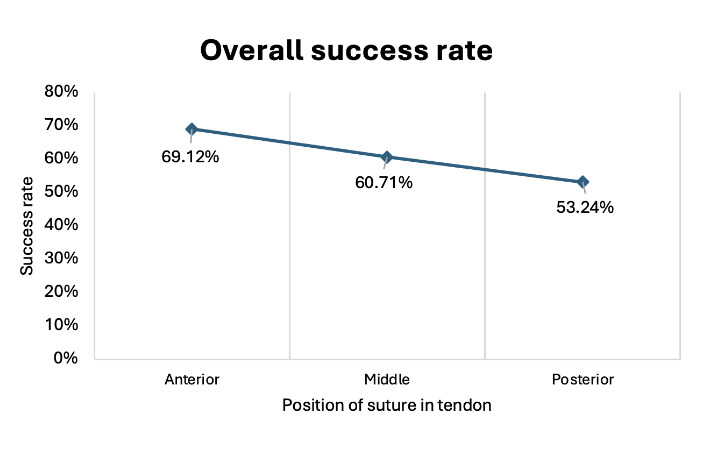
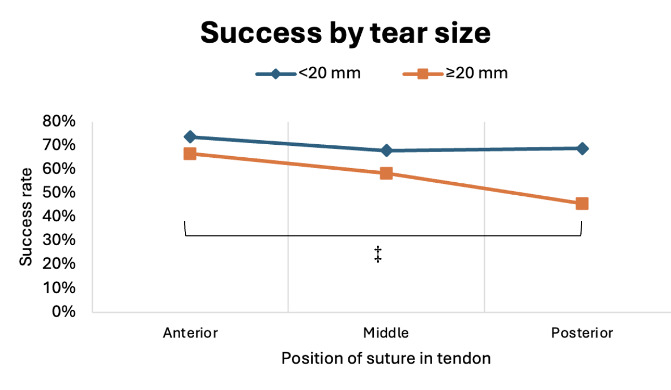
A total of 102 rotator cuff repair surgeries were performed on 60 males and 42 females. The mean age at operation was 61.04 ± 8.3 years (40 to 75 years). Of the 102 tears, 71.6% were full-thickness tears and 28.4% were partial-thickness tears with a mean width of tear at 20.0 ± 6.8mm (10 to 55mm). The mean tear width of men was 21.2mm and the mean tear width of women was 18.3mm (p=.029). The overall success rate of the antegrade suture passer was 60.56% (n = 102), with women (70.0%, n = 42) displaying a significantly higher success rate than men (53.9%, n = 60) (p=.042) (Figure 1). Full-thickness tears had a lower success rate (58.86%, n = 73) than the partial-thickness tears (64.83%, n = 29), however no significant difference was determined (p=.517) (Figure 2). Although there was no significant difference in success rate found between overall suture position (p=.060) or in rotator cuff tears < 20mm (p=.955), sutures passed through tears ≥ 20 mm displayed a significantly lower success rate in posterior positions (45.6%, n = 60) as compared to both middle (58.3%, n = 21) and anterior (66.5%, n=60) positions (p=.033) (Figure 3). The overall failure rate (38.6%, n=102), or percent passed through the rotator cuff missing the desired articular layer, was significantly higher for tears ≥ 20mm (44.3%, n = 60) than for tears ≤ 20mm (30.4%, n = 42) (p=.029).
Discussion
The results of this study demonstrated that an antegrade suture passer had a lower success rate in passing the suture through both deep and superficial rotator cuff tendon tissue than expected (60.56%, n = 102) (Table 1). Additionally, missed passes were particularly more prevalent in the posterior portion of the tendon in RCTs ≥ 20mm. Overall, the data did not support our hypothesis that RCTs ≥ 20mm would display lower success rates than RCTs < 20mm. However, the results do confirm our hypothesis regarding lower passing success in the posterior aspect of the tendon, with tears ≥ 20 mm displaying a significantly lower success rate (p=.023) (Table 2). Additionally, in every subgroup except tears < 20mm, the suture passer was least successful in the posterior portion of the tendon. Although no statistical significance was found between the three positions overall (p=.060), passing through the posterior aspect of the tendon demonstrated the least success within tears ≥ 20 mm, further supporting our hypothesis (Table 1). We found no statistical difference between partial-thickness and full-thickness RCTs, failing to support our hypothesis that partial-thickness repairs would demonstrate a higher success rate.
Several biomechanical and retrospective studies correlated differences in suture passer characteristics and tendon morphology with the strength of the suture-tendon interface and needle-tip breakage. Ponce et al. found that sheep tendon grafts repaired with suture passers with larger bite sizes (10mm) displayed higher resistance before failure than tendons repaired with smaller bite sizes (5mm) (P<.001) (Ponce et al. 2013). Chung et al. and Kim et al. reported that the needle failure of antegrade suture passers was more prominent in thicker tendons (7-9mm) with intrasubstance delamination (Chung et al. 2019; M. S. Kim et al. 2015). Unique to this study, we analyzed the performance of suture passing devices in repairing RCTs of various sizes and morphology at the anterior, middle, and posterior portion of the tendon, providing a valuable dimension for the repair of delaminated and retracted tendons.
Suture passer jaw depth may limit proper tissue bite capabilities in large, delaminated or deep surface retracted tears of the rotator cuff, especially in the posterior position of the tendon. From jaw-angle to the edge of the arm, the antegrade passer utilized in this study measures 16mm in length. This length is within the typical range (16-22mm) of most suture passers commonly used to repair RCTs arthroscopically. When repairing non-delaminated tears, burying the jaw of the suture passer into the lateral edge of the rotator cuff tendon is normally sufficient in ensuring an appropriate bite depth and suture penetration through the tendon. However, in delaminated and retracted deep layer tears, the inferior arm of the suture passer may not completely capture the deep articular layers of the tendon associated with the capsule. This observation has not previously been reported in the literature, and inadequate passage was found in a surprising number of tears. Overall, we found optimal suture placement to occur in 60.56% (n=102) of the shoulders (Table 1).
Additional morphological differences of the tear, such as tear predilection for the posterior position of the tendon or larger tears (>20 mm) may also limit the suture passer’s ability to capture the articular layers. Consistent with our findings that the suture passer was less successful in capturing the posterior portion (45.61%) relative to the anterior (66.53%) and middle (58.33%) (P=.037), current literature suggests that RCT delamination occurs most frequently in the posterior portion of larger tendon tears (Table 1). Tanaka et al. found that the delamination prevalence increased as the size of the tear increased within the posterior portion of the tendon, from small (37.5%), to medium (67.5%), to large (81.3%), to massive tears (93.3%), compared to the anterior and anterior-posterior portion (p=.001) (Tanaka et al. 2018). Matsuki et al. also reported a higher frequency of delamination occurring at the posterior rather than anterior part of the tendon (Matsuki et al. 2006). This coincides with our findings that tears < 20mm had a 68.76% success rate whereas tears ≥ 20mm had a 45.61% success rate within the posterior portion (p=.023) (Table 2). Histological and anatomical studies from Clark and Harryman et al. revealed congregations of musculotendinous connections with the joint capsule and ligament at the anterior part of the greater tuberosity (Clark and Harryman 1992; J.-H. Kim and Lee 2023). This inherent difference could lead to an increased prevalence of delamination, and subsequent failure of the antegrade suture passer, in the posterior portion of larger RCTs.
We hypothesized that a secondary reason the posterior portion of the tendon displayed lower antegrade passer success rates might be related to the intra-operative viewing portal. Han et al. examined the ability of surgeons to identify posterior delamination from the posterior, posterolateral, and lateral viewing portal in 130 patients and found that 11% were visualized through the posterior portal, 70% through the posterolateral, and 100% through the lateral view (Han et al. 2013b). Although all procedures were performed through the posterolateral view, the study suggests that up to 30% of the cases of posterior delamination could be missed from this view, compared to 0% in the lateral view which allows for visualization of the entire surface of the rotator cuff.
Inconsistent with our hypothesis, we did not find a significant difference between full-thickness RCTs (58.86%) and partial-thickness RCTs (64.83%) (p=.517) (Table 1). In a study analyzing antegrade suture passer performance with varying tendon thickness, Kim et al. observed difficulties in tendon penetration of the bursal side in partial-thickness tears (M. S. Kim et al. 2015). Multiple studies report that partial-thickness tears are 2-3 times more likely to occur on the articular surface than the bursal surface, often resulting in deep-layer tendon retraction (Matava, Purcell, and Rudzki 2005). We believed that this may make visualization and repair of the tear using a suture passer more difficult. However, in the case of our study, the frequency of deep layer retraction in partial-thickness tears did not result in a significant difference from full-thickness tears.
Analysis demonstrated a significantly lower success rate of the antegrade suture passer in male patients (53.9%, n=60) compared with female patients (70.0%, n=42, p=.042) (Table 1). Mean tear width also differed between groups, with larger tears in males (21.2mm) than in females (18.3mm) (p=.29). These findings align with prior reports that female patients tend to present with smaller rotator cuff tears than male patients (Sabo, LeBlanc, and Hildebrand 2021). Because tears >20 mm were associated with lower success rates in this study, the observed difference in device performance likely reflects variation in tear size rather than sex. Notably, previous studies have found no significant differences in patient-reported outcomes between sexes following rotator cuff repair (Sabo, LeBlanc, and Hildebrand 2021). Taken together, these results suggest that the apparent sex-related disparity is more accurately attributed to differences in tear morphology.
Several important clinical considerations can be drawn from the results of this study. Considering that the device had a 39.44% rate of unsuccessfully capturing both deep and superficial layers of the rotator cuff tendon, we recommend careful assessment of suture placement through the tendon in all attempts using an antegrade suture passer in the arthroscopic repair of RCTs. In addition to an increased awareness of this intraoperative scenario, surgeons should take precautions especially when repairing RCTs with an antegrade suture passer in tears ≥20 mm in the posterior part of the tendon with signs of delamination or deep layer retraction. We believe that repairing the deep layer will help lower postoperative retears, limit revisions, and improve patient outcomes.
Limitations
This study must be understood under the context of its limitations. First, a single surgeon assessing the accuracy of the suture placement within the tendon is vulnerable to observer bias. Device performance is influenced not only by design but also by surgeon technique, training, and experience, which can limit the generalizability of success rates across the broader orthopaedic community. Accordingly, the present study does not seek to establish the absolute efficacy of the antegrade suture passer, but rather to describe patterns of performance in relation to tear morphology, location, and size, as observed in a single-surgeon practice. This approach allows for characterization of technical challenges that may arise in specific contexts, while recognizing that outcomes should be interpreted relative to the operating surgeon.
Second, we did not record post-operative patient outcomes. Future studies are needed to investigate how repairing the deep articular layer correlates with range of motion, post-operative pain, and post-operative retear rates. Further research is necessary to correlate these intraoperative findings with long-term outcomes, such as retear rates and functional recovery.
Third, the antegrade and retrograde suture passers were selected based on what is routinely used in our surgical practice, which happened to be from different manufacturers. Importantly, only the performance of the antegrade suture passer was analyzed, while the retrograde passer was not included in the outcomes and therefore was not directly compared. Additionally, we recognize that device-specific design differences may influence performance, and that evaluating only one manufacturer for each type of suture passer may introduce potential bias. Future investigations that include multiple antegrade devices from different manufacturers, ideally assessed in a blinded fashion, would strengthen the robustness and generalizability of these findings. Such studies would allow for broader conclusions regarding device performance across different surgical contexts.
Conclusion
The antegrade suture passer demonstrated an overall moderate success rate, with reduced efficacy in larger tears and in the posterior part of the tendon where delamination and deep retraction are more prevalent. Surgeons should exercise caution when using this device in complex tear morphologies with delamination of the tendon layers and in tears ≥ 20mm involving the posterior aspect of the tendon.