









Introduction
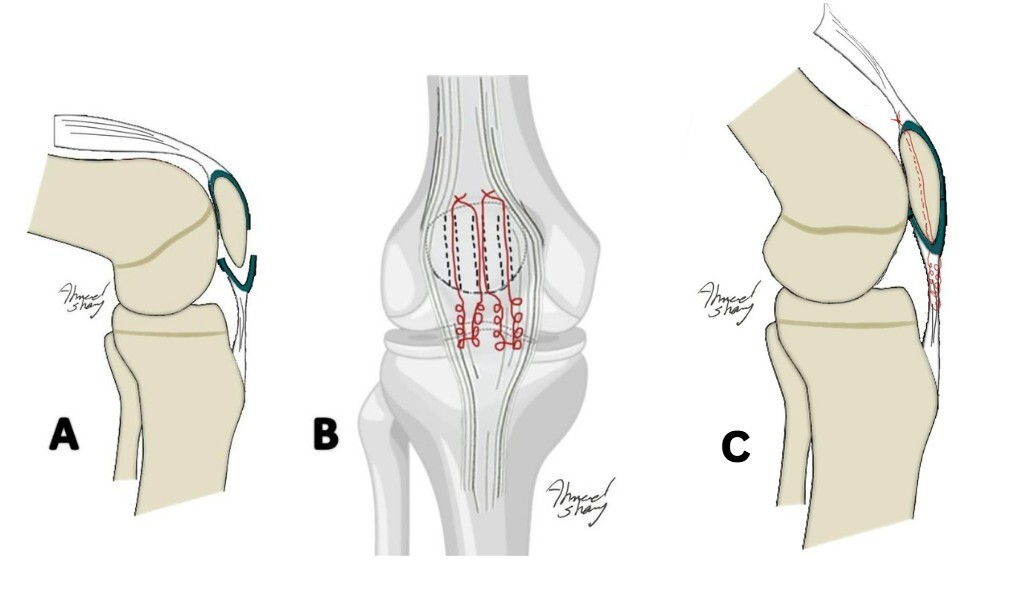
Young children are susceptible to a special kind of patellar fracture. These are called patellar sleeve fractures, and they affect the inferior pole of the patella. The patellar tendon, periosteum, and the distal articular cartilage will all avulse from the inferior surface of the patella, causing a disruption in the articular surface and the extensor mechanism (Papotto et al. 2024) (Figure 1A). Patellar sleeve fractures account for approximately 1% of all pediatric fractures and more frequently occur around 12 years of age (Ray and Hendrix 1992; Boushnak et al. 2020).Early detection and treatment of this condition are essential. Depending on the clinical and radiographic data, the diagnosis could initially be challenging and hard (Houghton and Ackroyd 1979; Grogan et al. 1990; Lin, Lin, and Wang 2011; Yeung and Ireland 2004).
These injuries commonly present with acute knee pain, limited range of motion, a joint effusion, and a palpable gap below the patella’s inferior pole. The diagnosis of patellar sleeve fractures is based in most cases on the presence of a high-riding patella, or patella alta, on the lateral plain radiograph. The Insall-Salvati ratio is used to calculate patellar height, with normal values ranging between 0.8 and 1.2. A ratio greater than 1.2 is indicative of patella alta, while a ratio below 0.8 suggests patella baja (Lin, Lin, and Wang 2011).
Further imaging modalities can be used to confirm the diagnosis if the radiographs are not clear enough to do so, and there is still a suspicion of a patellar sleeve fracture. Ultrasound is easy, cheap, and radiation-free to use; however, it depends on the operator (Hunt and Somashekar 2005). Computed tomography (CT) imaging offers high sensitivity in the detection of inferior pole patellar fractures (IPFP), with studies reporting detection rates of up to 88%. Compared to radiographs, which can only identify 44%. CT imaging provides superior visualization of bony structures, facilitating accurate diagnosis and classification of patellar sleeve fractures (Papotto et al. 2024). Furthermore, the patellar tendon-patella discontinuity can be verified, and the avulsed articular cartilage, which was difficult to visualize on routine radiographs, can be described using magnetic resonance imaging (Georgiadis and Comadoll 2021; Ditchfield, Sampson, and Taylor 2000).
According to the size and degree of displacement of the osteochondral fragments, either operative or non-operative treatment options are available for these fractures. Fractures with displacement, articular incongruity, and those with an associated extensor lag, are indicated for open reduction and internal fixation.
Different methods for operative fixation have been described, including tension band wires, absorbable intraosseous suture anchors, and transosseous nonabsorbable sutures (Kuo, Chen, and Lin 2022).
The goal of treatment is to restore the continuity and integrity of the extensor mechanism. Published methods to achieve this consist of small case reports using transosseous non-absorbable sutures or tension band wiring (Perkins, Egger, and Willimon 2022; Nowell and Niu 2023).
In this study, a patellar sleeve fracture requiring surgical repair of the osteochondral fragments is described. A schematic illustration of the transosseous sutures is presented in (Figure 1B and C). In all cases, informed consent for treatment and publication of anonymized data and images was obtained from the patients’ parents or legal guardians. Institutional approval was also secured in accordance with ethical standards.
_patellar_sleeve_fracture._b)_transosseous_sutures._c)_transosseous_sutures.jpg)
Case presentation
Case 1: clinical finding
An 11-year-old male was brought to the emergency room complaining of severe pain in his right knee. He had fallen from a height and hit his knee while kneeling. At the time of presentation, there was a noticeable hemarthrosis and a palpable gap at the inferior border of the patella. He could not fully extend his knee. The passive range of motion was sustained throughout the arc of motion, despite being painful. However, he could not perform a straight leg raise.
Diagnostic assessment
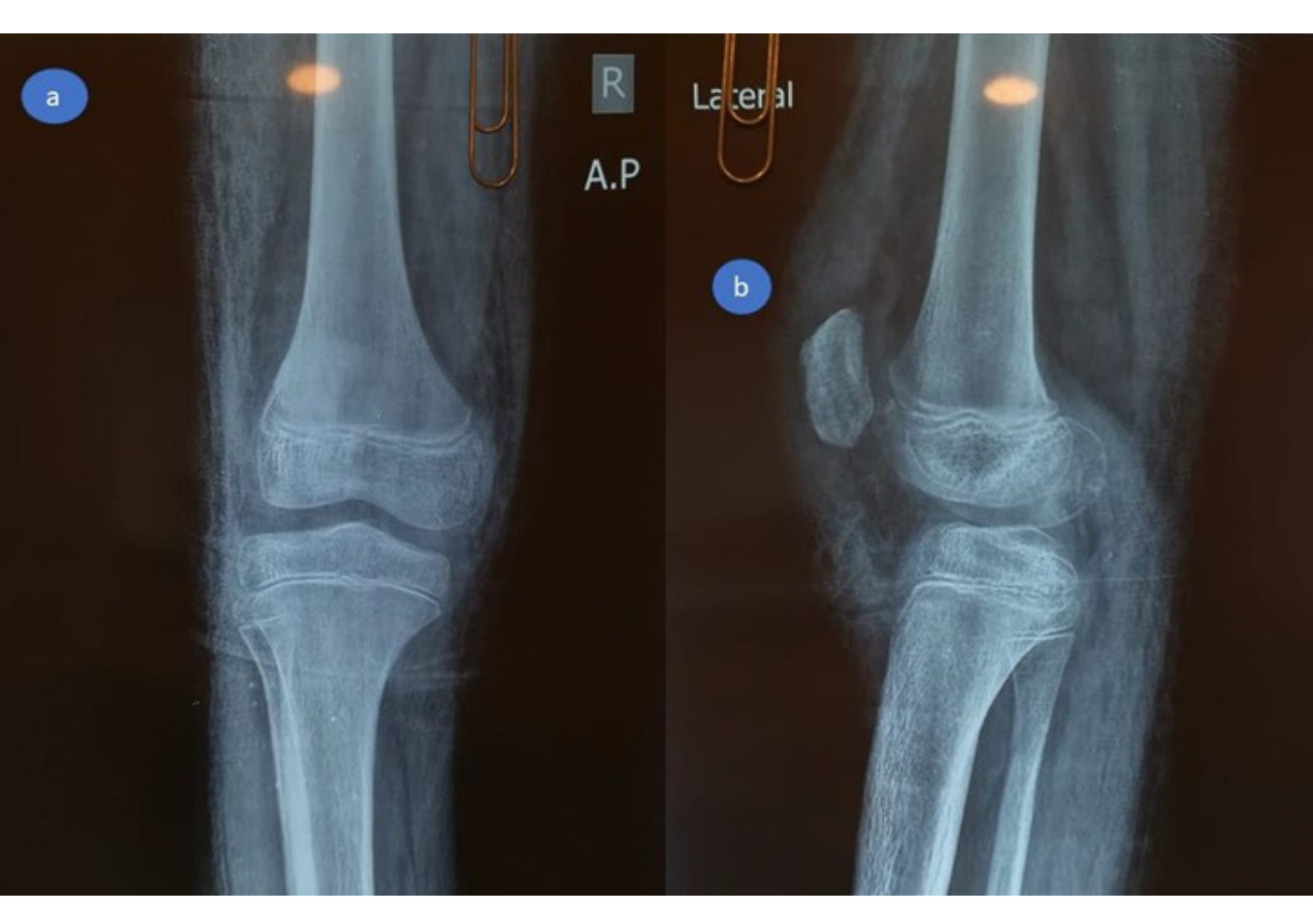
At the emergency room, radiographs were performed, which revealed a high-riding patella with a noticeable joint effusion as well as a small osteochondral fragment positioned distally to the patella. (Figure 2) As a result of the high-riding patella on the radiographs and the avulsion of the distal osteochondral side of the patella, a patellar sleeve fracture was detected. The surgery was scheduled for the next day.
_ap_view_and_(b)_lateral_view_showing_high-riding_patella_and_a_small.png)
Case 2: clinical finding
A ten-year-old boy with a history of autism presented to the emergency department with severe left knee pain and swelling after sustaining a direct trauma to the knee by a car. He presented with severe haemarthrosis and a palpable gap at the inferior border of the patella at the time of presentation. The patient had limited, painful active knee motion. The parents gave a history of autism.
Investigations
At the emergency room, standard AP and lateral radiographs were performed, which revealed patella alta as well as a small osteochondral fragment at the inferior pole of the patella. (Figure 7). As a result of these radiographic findings, a patellar sleeve fracture was diagnosed.
_lateral_view__patella_alta_and_small_displaced_fragment_at_the.jpeg)
Surgical intervention
Both patients were placed supine on a radiolucent operating table under general anesthesia, with a pneumatic tourniquet applied to the proximal thigh. The affected knee was positioned in full extension, prepped, and draped in a sterile fashion. A midline longitudinal incision was made over the patella and extended distally to expose the inferior pole. Hemarthrosis and interposed tissue were evacuated.
In both cases, the inferior pole of the patella demonstrated an avulsed osteochondral fragment involving approximately one-third of the articular cartilage and half of the periosteal surface. The patellar retinaculum was found to be torn and shredded, which complicated visualization, a finding commonly associated with sleeve fractures. Reduction was achieved under direct vision using reduction clamps to restore the patellar tendon–bone continuity and anatomical alignment of the osteochondral fragment.
Two parallel transosseous tunnels were created from the inferior to the superior patellar cortex using a 2.0-mm drill bit. Suture passage was facilitated with ACL wire passers to minimize fraying. Two No. 5 non-absorbable polyester sutures (Ethibond Excel®, Ethicon, USA) were woven in a Krackow fashion through the patellar tendon and osteochondral fragment. The four free suture limbs were shuttled proximally through the transosseous tunnels and tied securely over the superior pole of the patella, achieving stable fixation. The torn medial and lateral retinacula were repaired with absorbable sutures. Anatomical reduction and patellar height were confirmed both visually and fluoroscopically, using the contralateral knee as a reference. The wounds were closed in layers, and a long leg cylinder cast made of fiberglass was applied in full extension to protect the repair. (Figure 4-6)
_about_one-third_of_the_articular_cartil.jpeg)
_transosseous_sutures._(b)repair_of_the_patellar_ret.jpeg)
Postoperative Protocol
The cast was maintained for six weeks. Following cast removal, a structured rehabilitation program was initiated. Both patients began with isometric quadriceps exercises and a gradual range of motion (ROM) training. Knee flexion was progressed by approximately 45° each week, reaching 0–90° within the first month after cast removal. Progressive strengthening was emphasized, with restoration of quadriceps control as a primary goal. Full weight-bearing was allowed once the cast was removed.
Follow-up and outcome
Postoperative radiographs demonstrated satisfactory reduction and fixation (Figures 7,8).
_ap_view_and_(b)_lateral_view.jpeg)
_ap_view_and_(b)_lateral_view.jpeg)
By three to four months, both patients had achieved full knee ROM, restoration of quadriceps strength, and radiographic evidence of complete fragment healing (Figures 9, 10). Return to normal daily activity occurred between the third and fourth months, with clearance for sports and play at six months.
_ap_view_and_(b)_lateral_view.png)
_ap_view_and_(b)_lateral_view.jpg)
At final follow-up—12 months for Case 1 and 18 months for Case 2—both children were asymptomatic, with full ROM, normal quadriceps power, and no growth-related complications. Radiographs confirmed a well-centered patella with complete bony healing (Figures 11, 12).
_ap_view_and_(b)_lateral_view.png)
_ap_view_and_(b)_lateral_view.jpg)
Discussion
Treatment options for patellar sleeve fractures range from conservative to non-conservative, depending on the degree of displacement. An immobilization with a cylindrical plaster of Paris cast can be used in conservative therapy when the fracture is only slightly displaced. If not, it is imperative to do surgical intervention (Lin, Lin, and Wang 2011).
Various open reduction techniques are reported to achieve anatomic reduction of the articular surface, such as intraosseous suture anchors, tension band wire, and transosseous sutures. When stiff fixation cannot be performed because of the tiny size of the osteochondral fragment, intraosseous and transosseous anchor sutures may be employed. One potential benefit of the suture-only method is the mitigation of prominent hardware (Kaar, Murray, and Cashman 1993).
Patient-reported outcomes following these different techniques have been variable. Studies evaluating tension band wiring have demonstrated satisfactory union and restoration of knee stability, but some patients reported anterior knee pain or discomfort related to hardware prominence, occasionally requiring implant removal. Intraosseous and transosseous anchor sutures generally yield favorable functional outcomes, with patients describing early pain relief, improved confidence in knee function, and fewer complaints related to soft tissue irritation.18
Although some patients report prolonged stiffness or delayed return to sports, compared with more rigid fixation methods. Overall, most reports suggest that regardless of the fixation technique, careful rehabilitation and avoidance of hardware complications play a critical role in optimizing patient-reported functional recovery and return to pre-injury activity levels (Perkins, Egger, and Willimon 2022).
Since patellar vascularization usually originates from the front side of the distal pole, ischemic necrosis of the patella can happen. Hence, necrosis of the distal pole is a feared consequence (Kaar, Murray, and Cashman 1993)
In these two cases, the inferior pole of the patella was not large enough to be securely fixed with screws (tiny size not more than 1*1 cm2). Transosseous tunnel sutures were utilized to fix the inferior pole to the main proximal fragment.
The use of patellotibial cerclage was not pursued in this instance due to the possibility of patella baja and early closure of the tibial tuberosity apophysis with premature growth arrest, both of which could lead to sagittal plane deformities similar to genu recurvatum. It’s also important to take into account irritation and the growth disorders that this cerclage can cause at the tibial apophysis (Lin, Lin, and Wang 2011).
An important distinction in our approach lies in the use of a modified transosseous suture technique without additional hardware or cerclage augmentation. This method not only provided stable fixation but also minimized the risk of growth plate disturbance, especially at the tibial tuberosity, where patellotibial cerclage may predispose to premature apophyseal closure and genu recurvatum. Moreover, by avoiding tension band wiring and metallic implants, we reduced the potential for symptomatic hardware, the need for future removal surgeries, and allowed for a simplified surgical procedure.
Intraoperatively, our technique emphasized preserving the integrity of the distal osteochondral fragment, with careful suture passage through the patellar tendon and inferior pole, avoiding further fragmentation.
An important limitation of our report is the absence of long-term follow-up into skeletal maturity. Although no growth disturbance was observed at one-year and 18-month follow-up, the patellar ossification center may remain open until adolescence, and transosseous tunnels theoretically pose a risk to the developing patellar physis. While we attempted to minimize this risk by careful tunnel placement and limiting the number of drill holes, longer follow-up into skeletal maturity would be necessary to definitively exclude growth-related complications. This potential risk should be considered when choosing fixation methods in skeletally immature patients.
In our setting, both patients were managed postoperatively in a long leg cast. Although hinged knee braces or knee immobilizers offer the advantage of gradual controlled mobilization and earlier range of motion, they were not readily available in our hospital, and cost was a limiting factor for families. Immobilization in a cast therefore, represented a pragmatic choice, ensuring adequate protection of the repair.
Restricted knee flexion following cast removal due to muscle atrophy is a recognized problem, even though casting increases fixation security. Fortunately, the two patients responded very well to physical therapy, where full extension and near-full flexion were accomplished rapidly, within one month after removing the cast.
Notably, the second case in our series involved a child with autism spectrum disorder, which presented unique challenges in assessment and postoperative compliance. This highlights the versatility and reliability of our technique even in patients with communication or behavioral difficulties.
Tips and Tricks
Preserve distal bony fragments: Avoid sacrificing small distal osteochondral pieces, as they provide additional stability and healing potential. Bone-to-bone healing offers superior biological integration and strength compared to tendon-to-bone healing.
Use strong, nonabsorbable sutures: No. 5 Ethibond provides durable fixation while minimizing the risk of suture breakage; however, FiberWire offers even greater tensile strength and is associated with a lower risk of infection.
Tunnel placement: Drill tunnels slightly divergent to prevent convergence and allow even distribution of tension across the patella.
Secure knots proximally: Tying sutures over the superior pole distributes load across intact bone and reduces cut-out risk.
Intraoperative imaging: Fluoroscopy helps confirm anatomical reduction and patellar height; using the contralateral knee as a reference provides an additional guide for achieving accurate alignment and restoration of patellar height.
Post-op immobilization: Initial cast or brace protection is critical to avoid early tension overload on the repair.
Pitfalls and How the Technique May Fail
Improper tunnel trajectory: Converging tunnels can weaken bone and lead to tunnel blowout or loss of fixation.
Insufficient reduction: Failure to fully seat the osteochondral fragment may result in step-off, altered patellar tracking, or persistent anterior knee pain.
Suture cut-through: Aggressive tensioning may cause sutures to cut through osteochondral tissue, particularly in small or comminuted fragments.
Quadriceps weakness/stiffness: Extended immobilization can lead to delayed rehabilitation, quadriceps atrophy, and knee stiffness.
Noncompliance with immobilization: In children, early activity or cast removal may compromise healing and cause fixation failure.
Conclusion
Patellar sleeve fracture is an uncommon condition that affects young individuals as a result of either a direct injury or a sudden contraction of the quadriceps on a flexed knee. Identification of this condition is essential, especially in the emergency department by emergency physicians. This can be accomplished by identifying its distinctive feature, patella alta, and since the majority of these instances present without any bone fragments that can be identified by X-rays, Hemarthrosis is crucial to making the diagnosis. For displaced fractures, early surgical intervention is required. Fixation of osteochondral fragments with transosseous tunnel sutures is an option that can be utilized safely and effectively.
Acknowledgement
None.
Ethics approval and consent to participate
Informed consent was obtained from the patients or caregivers.
Consent for publication
Written informed consent was obtained from the caregivers for publication of this case report and any accompanying images.
Availability of data and materials
The data is available in the manuscript.
Competing interests
The authors declare that they have no competing interests.
Funding
No funding was received for this research.