Introduction
Despite the widespread success of total knee arthroplasty (TKA), up to 25% of TKA recipients remain dissatisfied with the outcomes of the procedure (Choi and Ra 2016). Anterior knee pain that persists following TKA remains among the most commonly reported complaints associated with dissatisfaction (Halawi et al. 2019; Mathis et al. 2021). Even among satisfied TKA recipients, a third report some extent of anterior knee pain one year postoperatively (Meftah, Ranawat, and Ranawat 2011). While various etiologies have been speculated to correlate with postoperative anterior knee pain, the majority of attempts to overcome this complication have revolved around addressing a theoretical patellar source of pain. As such, patellar resurfacing gained significant traction as a potential solution for anterior knee pain following TKA (Koh et al. 2019; Raaij et al. 2021; Dong et al. 2018; Thiengwittayaporn, Srungboonmee, and Chiamtrakool 2019). While proponents of patellar resurfacing argue it reduces anterior knee pain after surgery, the procedure introduces additional technical variables such as patellar component positioning, overstuffing of the patellofemoral joint, and patellar tilt, among others. In resurfaced patella, a positive association between patellar tilt and anterior knee pain remains controversial, with reports supporting and refuting the presence of such a correlation (White et al. 2019; Joseph et al. 2021).
Robotics have gained substantial popularity over the last decade within the field of arthroplasty. The rapid adoption of robotic technology is in part driven by the perceived capacity to reduce outliers and increase replicability, improve alignment, and allow for more accurate preoperative planning and execution than conventional methods. Robotic systems have been used with different techniques to replicate methodologies applied with conventional methods, namely measured resection and gap balancing techniques. While various robotic systems and utilization methodologies have been assessed, multiple studies have noted superior accuracy and precision of femoral and tibial components positioning with robotic TKA when compared to conventional methods (Kayani et al. 2019; Mahoney, Kinsey, Sodhi, et al. 2022; Zhang, Ndou, Ng, et al. 2022). To date, the literature remains lacking of evidence assessing the impact of robotics on patella tracking, and specifically patellar tilt, in the setting of gap balancing technique.
Within that context, the aim of this study is to compare patellar tilt in robotic and conventional TKA. We specifically assess the degree of patellar tilt and frequency of outliers between the two techniques. We hypothesize improved patellar tilt with robotic TKA with fewer outliers that could be attributed to improved femoral component rotation and flexion gap balance in that group.
Methods
Study Population
Following approval by our institutional review board, all primary TKAs performed by a single surgeon (author initials withheld) between January 2018 and September 2022 were assessed. Demographic and operative data were collected including age, gender, implant brand and model, choice of patellar resurfacing, and whether robotic assistance was used to complete the operation. The Western Ontario and McMaster Universities Arthritis Index (WOMAC) patient-related outcome measure (PROM) was collected preoperatively, 3 months postoperatively, and 1 year postoperatively. Patients were excluded from analysis if postoperative radiographs did not include a diagnostic merchant view that could be used to perform patellar tilt measurements.
Surgical Technique
Patients included in the study underwent a standardized surgical exposure by the same surgeon, utilizing a midline skin incision and a medial parapatellar approach without the use of a tourniquet in any patients. A medial soft tissue release was performed following arthrotomy at various extents, individualized based on limb deformity and intraoperative gap assessment. The lateral fat pad, lateral meniscus, anterior and posterior cruciate ligaments were excised, and the tibia was subluxed exposing the entire surface.
Implant utilization varied over the study period and included implants from four different manufacturers (Zimmer Biomet, Warsaw, Indiana; Smith+Nephew, Memphis, Tennessee; ConforMIS, Billerica, MA; Depuy Synthes, Warsaw, Indiana) (Table 1). Additionally, four types of polyethylene were used, including: constrained-posterior stabilized (CPS), cruciate-retaining (CR), medial congruent (MC) and posterior-cruciate substituting (PS) (Table 2). Implants were selected based on surgeon discretion in order to provide the most appropriate implant and amount of stability for each patient.
The population was divided into two cohorts depending on whether the surgery was performed with robotic guidance based on discretion of the senior surgeon. Conventional knees were performed with a measured resection technique with post-resection soft tissue balancing. All conventional knees were planned to achieve neutral mechanical alignment. Robotic knees were performed with one of three robotic platforms (ROSA Knee System, Zimmer Biomet, Warsaw, Indiana; NAVIO Surgical System, Smith+Nephew, Memphis, Tennessee; or CORI Surgical System, Smith+Nephew, Memphis, Tennessee). Regardless of robotic platform used, a similar workflow was used. Femoral and tibial osteophytes were removed during the exposure. Registration of the robot and identification of bony landmarks were completed using a protocol that did not require any advanced imaging. Subsequently medial and lateral stress-gaps were assessed, and femoral and tibial cuts were planned accordingly to achieve balanced gaps in flexion and extension and to be within 3 degrees of neutral mechanical alignment.
Patellar management varied over the study period. All patients received a lateral facetectomy and circumferential denervation, however the patella was resurfaced at the discretion of the senior surgeon based on patient specific factors such as balancing retaining native structures versus removing diseased surfaces. When the patella was resurfaced, the cut was performed using a free-hand technique with an oscillating saw, parallel to the anterior cortex, while aiming to produce symmetric thickness throughout. Patellar resurfacing, when performed, was done with a cemented 3-button polyethylene patellar component.
Radiographic Assessment
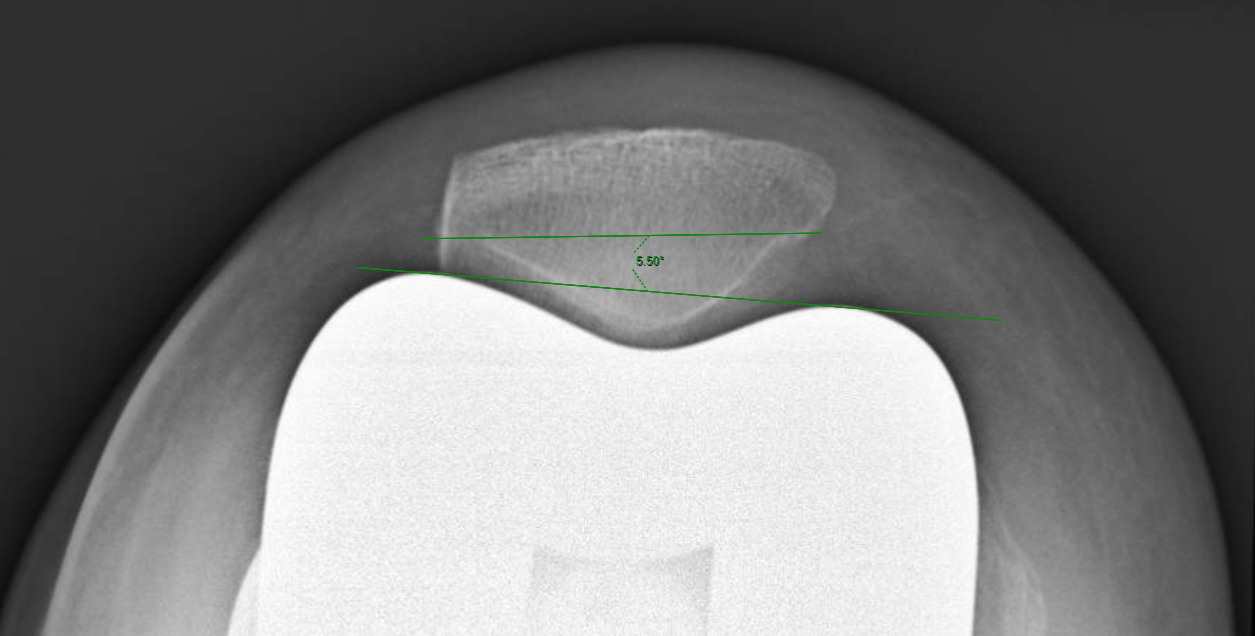
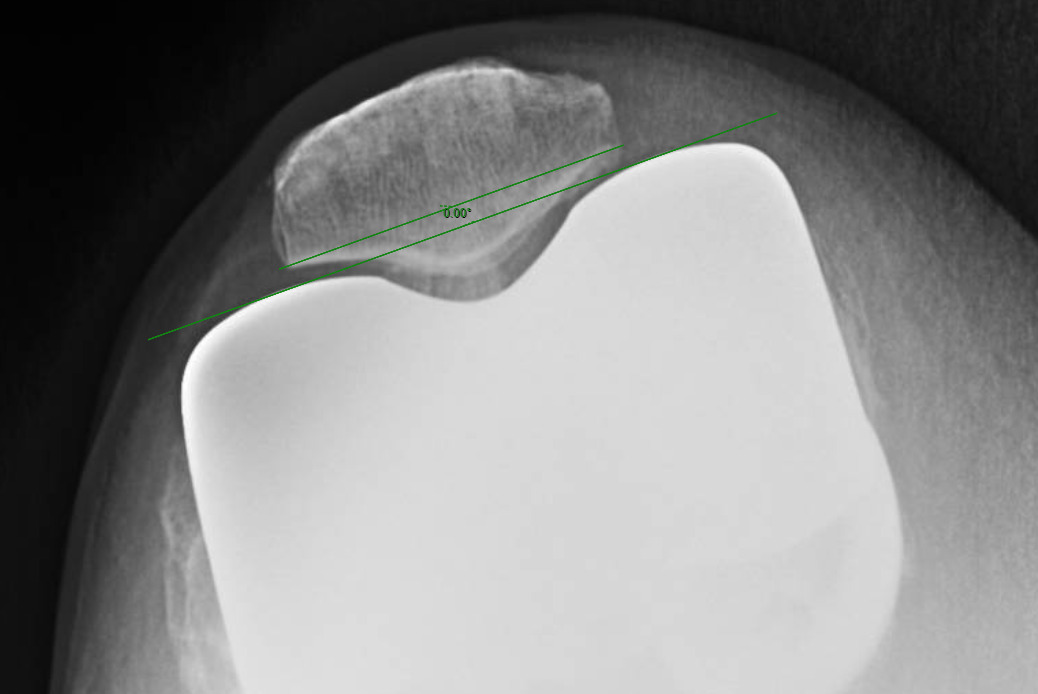
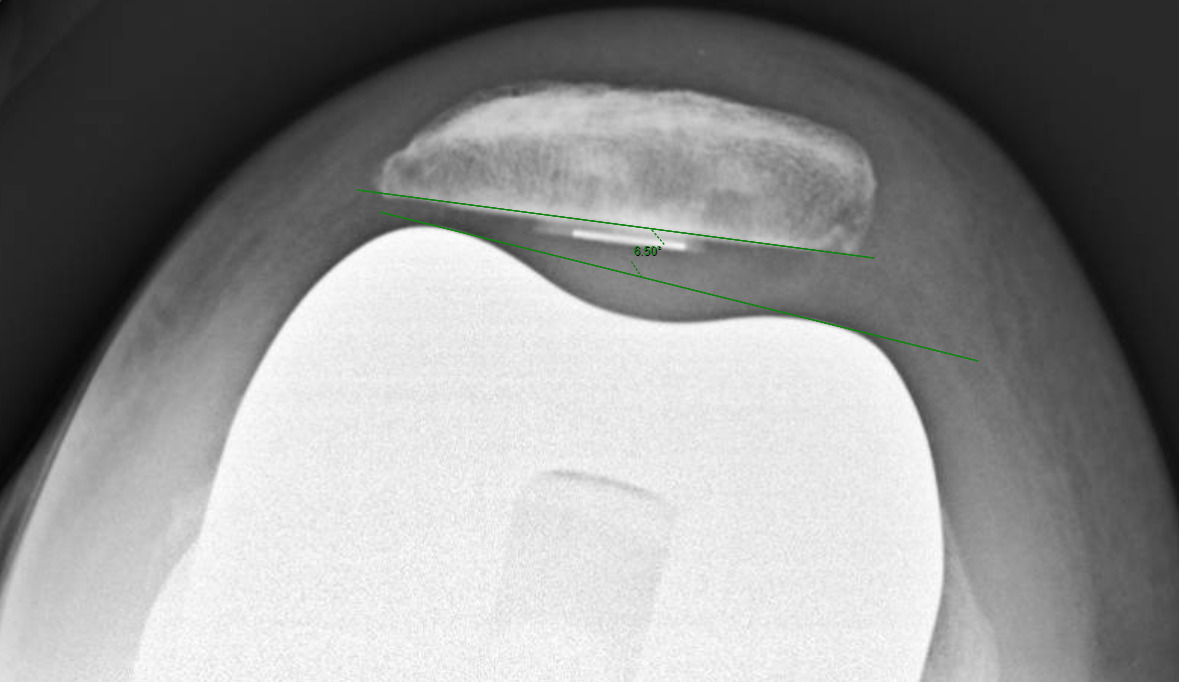
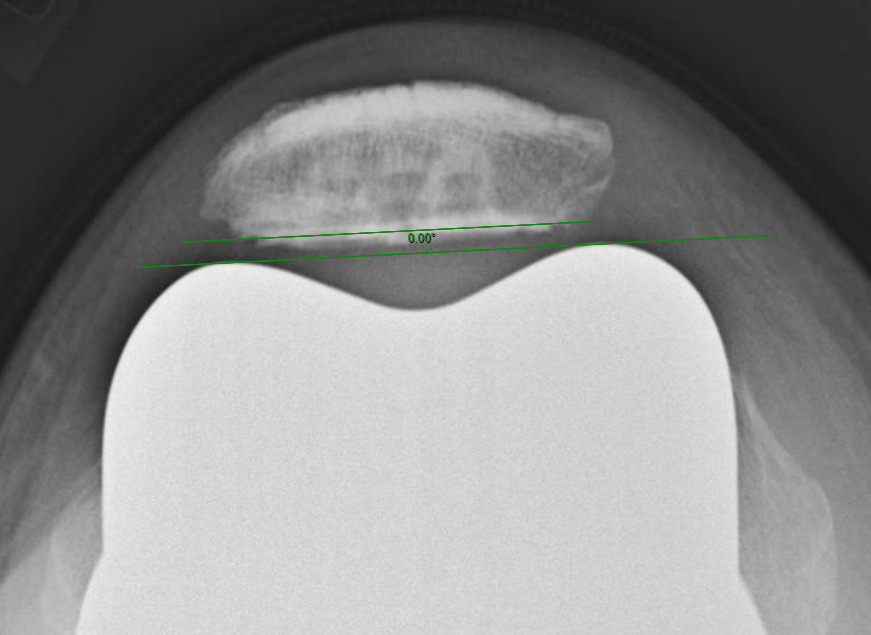
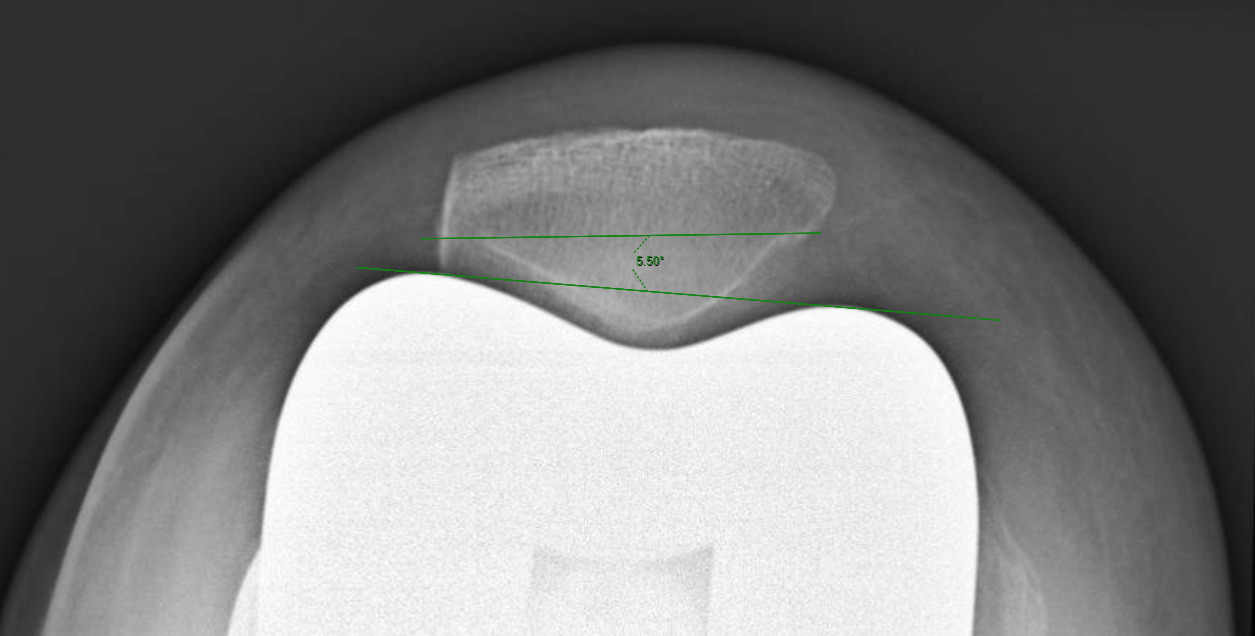
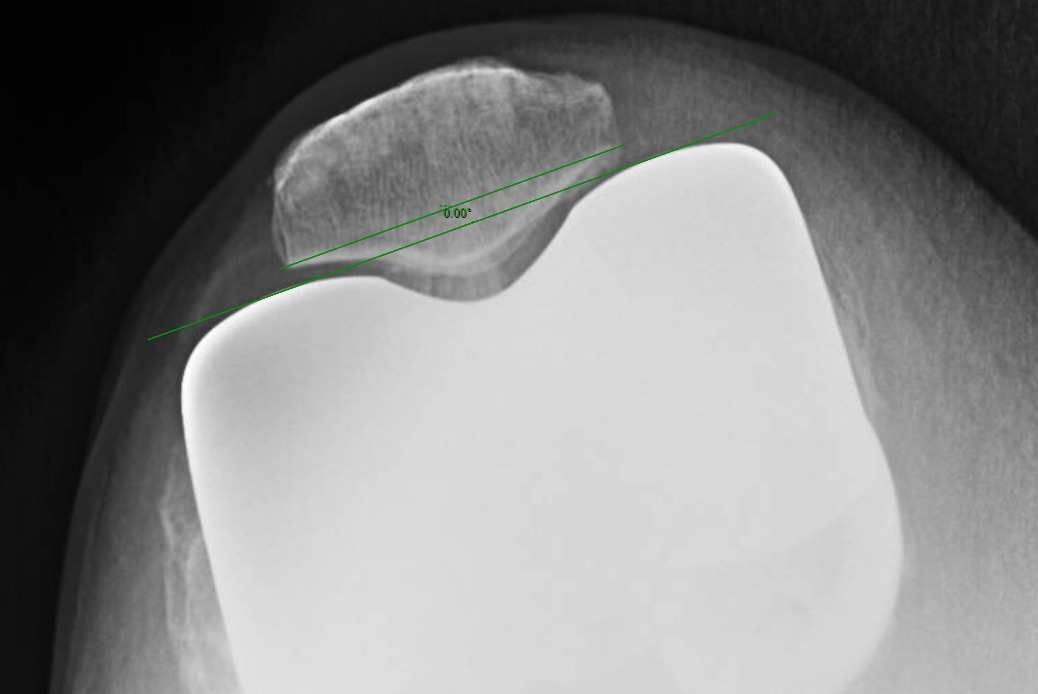
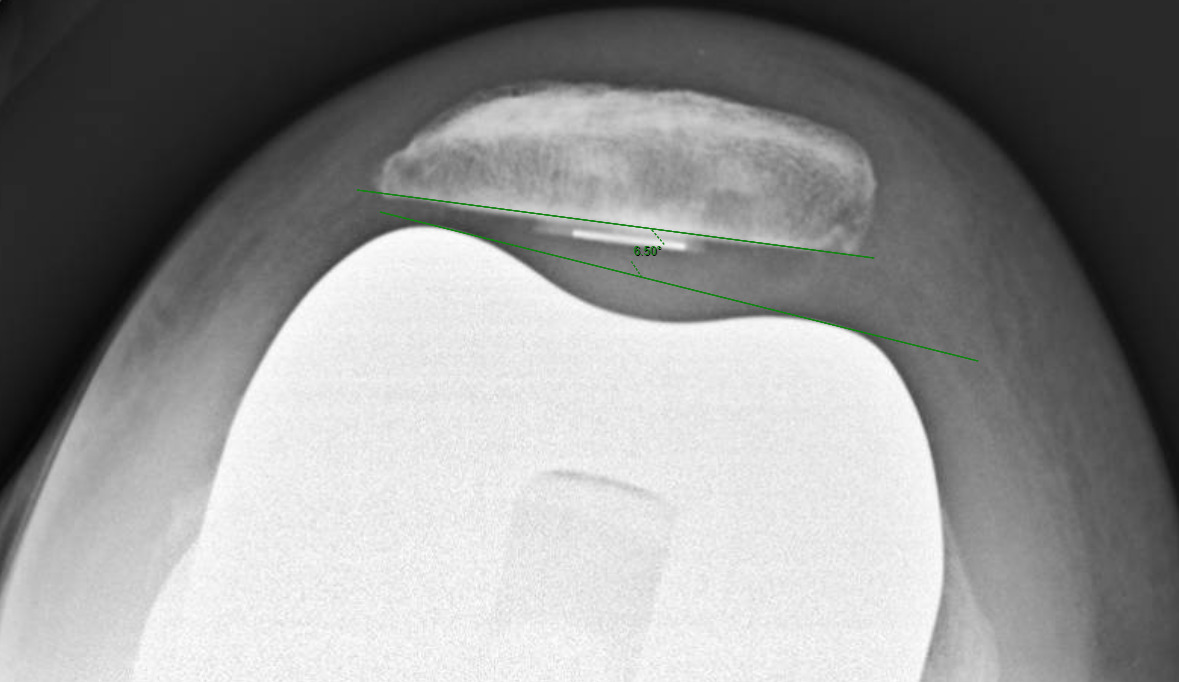
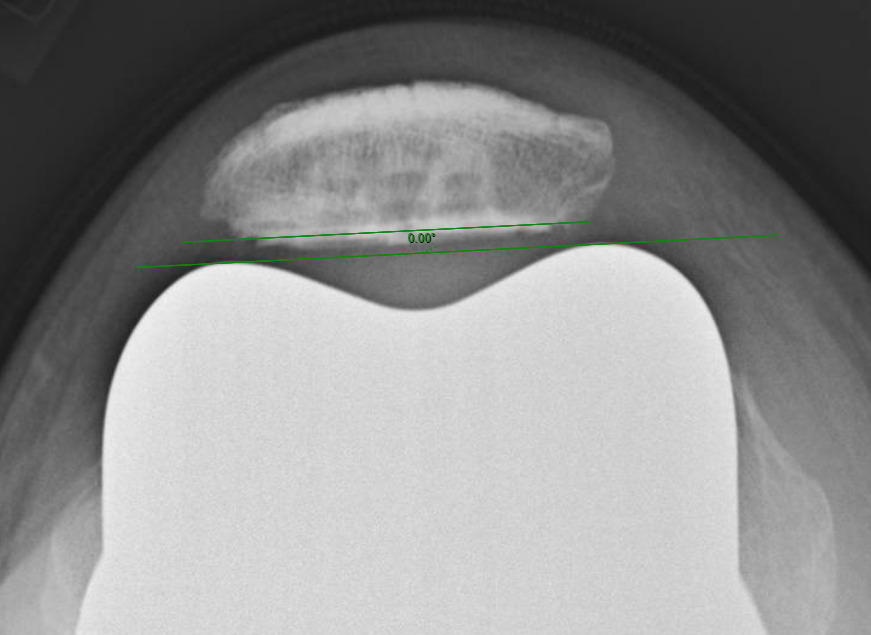
Measurements were performed by one rater following extensive training from the senior author using a standardized measurement protocol. The rater was blinded to the use of robotics when measurements were made. Assessment of postoperative merchant view radiographs on digital imaging software according to the method of Gomes et al. was conducted (Gomes, Bechtold, and Gustilo 1988). The angle between the resected surface of the patella and a line tangent to the anterior condylar axis of the femoral component was measured and recorded (Figures 1-4). The patellar tilt was recorded as positive when the tilt was lateral and was recorded as negative when the tilt was medial. The absolute value of the patellar tilt was used during data analysis as a neutral of 0° was considered the goal for patellar tilt during surgery, and both increasing lateral and medial tilt away from neutral were considered as increasingly imperfect. The percentage of outliers where the patellar tilt exceeded 3 degrees off neutral was also calculated for each group.
Statistical Analysis
Statistical analysis was carried out using (version 28.0, SPSS Inc., Chicago, IL, USA). Chi-square tests were used to examine for differences between the robotic and conventional groups for categorical variables such as gender and t-tests for continuous variables such as age, BMI, and patellar tilt. Binary logistic regression was also used so see if there was any association between patellar resurfacing and patellar tilt. WOMAC Pain, Stiffness, and Function scores were analyzed individually. Independent samples t-tests were conducted to analyze WOMAC scores between the robotic and non-robotic cohorts at each time period. All P values were for 2-sided tests, and P values < 0.05 were considered statistically significant.
Results
A total of 602 consecutive knees were performed over the study period, including 276 knees with robotic guidance and 326 knees with conventional instrumentation. Among those, 16 robotic knees (5.8%) and 15 conventional knees (4.6%) were excluded due to lack of postoperative merchant view radiographs, leaving a total of 260 knees in the robotic cohort and 311 knees in the conventional cohort.
There were no differences in baseline demographics such as age and gender between robotic and conventional groups (32). However, since the incidence of patellar resurfacing was significantly lower in the robotic knee cohort (60.8% vs 86.5%; p < 0.00001), a binary logistic regression was completed to control for this baseline difference. This regression showed no significant association between decreasing patellar tilt and a lack of patellar resurfacing (p = 0.217, Odds Ratio = 1.045, 95% CI = 0.974-1.121) (Table 4).
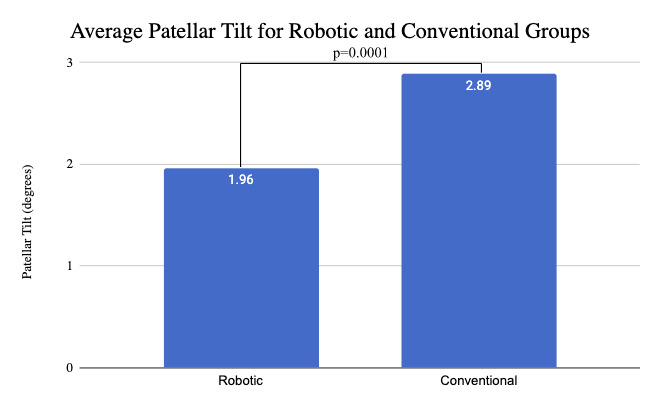
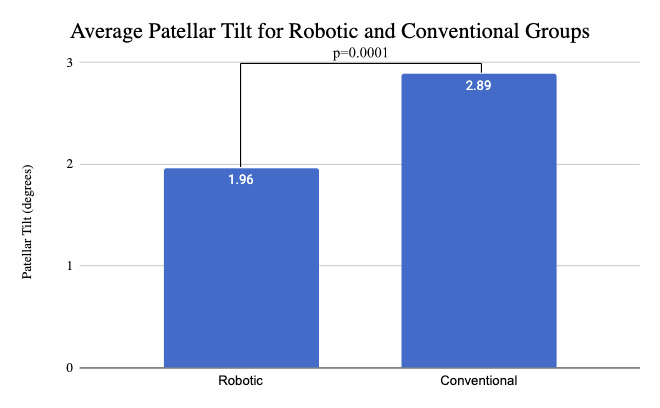
Using the absolute value of patellar tilt, the mean patellar tilt in the robotic cohort was 1.96° of lateral tilt (±2.74°, range 0° to 15°), compared to a 2.89° of tilt (±2.95°, range 0° to 14°) in the conventional cohort (p = 0.0001) (Figure 5). The percentage of outliers where the patellar tilt exceeded 3 degrees from neutral was significantly higher among conventional cohort (34% vs 20%, p = 0.00018) (Table 5).
WOMAC scores did not differ significantly between the robotic cohorts postoperatively or 3 months postoperatively (Table 6). WOMAC Pain scores were significantly better in the robotic cohort (Mean = 16.6; range = 8 to 20) than the non-robotic cohort (Mean = 15.0; range = 0 to 20) at 1 year postop; t(569) = 4.835; p < 0.001 (Table 5). WOMAC Stiffness scores did not differ between the robotic and non-robotic cohorts at 1 year postop; t(569) = 0.645; p = 0.520. WOMAC Function scores also did not differ significantly in the robotic and non-robotic cohorts at 1 year postop; t(569) = 1.390; p = 0.165.
Discussion
The current study reveals that robotic TKA leads to a statistically significant improvement in patellar tilt, with a smaller percentage of outliers, compared to conventional TKA, confirming the original hypothesis. While robotic technology plays no direct role in patellar tracking or component positioning, these findings point towards an indirect impact potentially through optimized flexion gap balancing and soft tissue tensioning and improved rotational alignment of the femoral and tibial components.
Robotic TKA aims to improve alignment, reduce variability, and potentially standardize postoperative outcomes (Decking et al. 2004). The findings from the current study indicate significantly less patellar tilt among robotic TKA cohort compared to the conventional counterpart (1.96° vs 2.89°, respectively, p < 0.0001). While multiple factors have been identified to contribute to patellar tilt following TKA, femoral component rotation has been highlighted as one of the major determinants (Anglin, Brimacombe, Hodgson, et al. 2008). Matsuda et al. assessed rotational alignment of tibial and femoral components and noted a positive correlation between patellar tilt and the sum of the internal rotation angles of the components (Matsuda et al. 2001). The positive impact of robotics on improved femoral component alignment has been extensively supported in the literature. Kayani et al prospectively compared robotic and conventional TKA and noted higher accuracy in achieving the planned position in the coronal and sagittal planes among the robotic cohort (Kayani et al. 2019). Similarly, Mahoney et al, in a prospective study comparing 143 robotic to 86 conventional TKA, reported a statistically significant improvement in deviation of femoral component rotation between planned and realized component position (1.5° vs. 1.3° for conventional and robotic, respectively, p = 0.015) (Mahoney, Kinsey, Sodhi, et al. 2022). An improved rotational alignment of the components in the robotic TKA cohort could yield improved patellar tilt, potentially providing an explanation to the results noted in our study.
Additionally, the present study noted a significantly lower percentage of outliers in patellar tilt among the robotic cohort reaching 20% compared to 34% in conventional group when outliers were defined as a difference of more than 3 degrees. (p = 0.00018). This improved consistency in patellar tracking in some respects mirrors the findings of improved consistency in sagittal and coronal alignment from Song, et al., who reported no outliers in a robotic cohort, as defined by error ≥ 3 degrees, in the mechanical axis, and coronal and sagittal inclinations, compared to a total of 24% outliers in the mechanical axis for the conventional TKA cohort (Song et al. 2013). In a more recent meta-analysis comparing accuracy of component positioning in the coronal plane between robotic and conventional TKA, Zhang et al. similarly noted substantially lower difference between planned and realized component position, with a narrower spread within the robotic arm cohort (Zhang, Ndou, Ng, et al. 2022). While the aforementioned studies assess different robotic systems and apply various definitions and values for accuracy and precision, the collective results point towards a general common pattern of improved alignment and lower rate of outliers among robotic TKA in comparison to conventional methods. As such, and as the robot plays no direct role in the patellar cut or button positioning, we speculate a consistent and precise femoral component positioning as a potential contributor to the findings of this study.
When applying gap balancing techniques, component position and rotation are mainly guided by the ligament balancing axis, irrespective of the anatomical bony alignment. This approach has been amplified in more recent years by the introduction of robotic TKA with ensuing heightened accuracy and precision of measurements and intraoperative planning. While alternative factors might be speculated to contribute to the observed results of the current study, an improved ligamentous balance in flexion could explain our reported outcomes. Flexion gap balancing has been recently noted to play a critical role in predicting patellar tilt, regardless of the femoral component rotational profile. Ko et al retrospectively compared 99 patients with internal femoral rotation and 146 with femoral component in 3°–5° external rotation, to evaluate the effect of femoral component rotation on patellar tracking using the gap balancing technique (Ko et al. 2021). The authors noted no statistical significant difference between the groups with regards to patellar tilt angle (−0.4° ± 3.6° vs. 0.1° ± 4.1°, respectively, p = 0.251). These findings led the authors to conclude that ligament balance in flexion is critical in determining patellar tracking. As such, the results presented in the current study of lower patellar tilt in the robotic TKA cohort could be attributed to improvement in flexion gap balancing and more accurate component positioning achieved through utilization of a gap balancing technique with robotic guidance. Furthermore, the authors hypothesize lower patella tilt from robotic TKA could also have beneficial clinical implications, which would be consistent with our results showing significantly improved WOMAC pain scores in the robotic cohort.
The ultimate target for robotic TKA remains to improve postoperative outcomes and survivorship of the prosthesis through optimized component alignment and reproduction of native knee kinematics. Consistent evidence of correlation between patellar tilt and postoperative outcomes following TKA remains lacking in the literature. In a retrospective analysis of 90 TKAs, White et. al . noted no correlation between tilt and postoperative pain (White et al. 2019). Interestingly, Joseph et al assessed postoperative outcomes in 878 TKAs that were divided into 633 without patellar tilt and 193 with patellar tilt. The authors reported improved global satisfaction and KSS scores in the cohort without patellar tilt, with significantly lower revision rate for any cause (p = 0.019) (Joseph et al. 2021). While the impact of patellar tilt on postoperative outcomes remains unclear in the literature, no studies have assessed this correlation among robotic TKA recipients. Given the multitude of variables that might lead to patellar tilt, and as robotic technology aids in eliminating variabilities related to component positioning and ligamentous balancing, future studies are needed to better understand the impact of patellar tilt on postoperative outcomes and anterior knee pain.
This study is not without limitations. This is a radiographic analysis of a consecutive case series of TKAs performed by a single surgeon at a single institution. As such, the generalizability of the findings reported in this study might be limited. However, this same limitation acts as a strength supporting the results, as there exists no variability in technique or other unknown variables that might have impacted the results. It is also possible that while all merchant view radiographs are taken at the same angle of knee flexion, there may have been some variability in radiographic view. Additionally, a free hand resection technique of the patella is highly surgeon dependent and could impact reproducibility. Furthermore, there was heterogeneity in the implants and robotic systems utilized which may introduce additional variability between cohorts that might not have been fully accounted for with methodology utilized. Lastly, the study was limited to radiographic analysis with no clinical outcomes or long-term follow-up reported in this study. While this methodology is common for early robotic studies, clinical outcomes and long-term follow-up were not stated aims of this study and would constitute interesting venues for future analysis. Prospective research with long-term follow-up with clinical correlation of varying patellar tilt would be beneficial to explore.
Despite these limitations, this study has several strengths as it constitutes a large cohort of consistent and standardized population and a first analysis of a prospectively collected data assessing patellar tilt in the setting of robotic TKA in comparison to conventional TKA performed with the same implant. While most other alignment analyses focused on femoral and tibial components, this is the first report to the authors’ knowledge to analyze the impact of robotic TKA on patellar tilt.
In conclusion, the findings from this radiographic analysis reveal an improved and replicable patellar tilt in robotic TKA in comparison to conventional methods. The results of this study might further support the notion of improved flexion gap balancing and general alignment with robotic TKA and consistency of results with lower incidence of outliers. These findings could explain to some extent the improved pain witnessed with robotic TKA in comparison to conventional methods. As anterior knee pain and dissatisfaction after TKA continue to pose a significant challenge and an economic burden, further assessment of correlation of the findings from this study with long term clinical outcomes remains critical.