






INTRODUCTION
Extra-articular coronal plane deformity is found in up to 12 % of primary total knee arthroplasties (TKA) and is a well-recognized risk factor for malalignment, soft tissue imbalance, and early implant failure (Loures et al. 2019). Wolff et al. indicated that deformities ≥ 15° in the tibia or ≥ 20° in the femur overwhelm the capability of usual intra-articular bone cuts to achieve neutral alignment without sacrificing collateral ligament insertions (Wolff, Hungerford, and Pepe 1991). Follow-up clinical series established that greater intra-articular resection compromises the joint line, requiring release of the collateral ligaments and, at worst, constrained polyethylene liners—all of which have been associated with poorer mid-term functional scores (Wang and Wang 2002; Laskin 2002).
To circumvent these compromises, the surgeon can perform a two-stage osteotomy with delayed TKA or a single-stage extra-articular osteotomy with arthroplasty. The latter, enabled by long stems that span the osteotomy, can recreate the mechanical alignment while leaving ligament tension and joint line height intact, reducing the possibility of instability and polyethylene wear (Catonné, Sariali, Khiami, et al. 2019; Sculco et al. 2019). Studies comparing simultaneous osteotomy and staged approaches report comparable implant survivorship but fewer early complications with simultaneous procedures (Oh et al. 2019; Park et al. 2018).
Despite these promising findings, the best management for “borderline” deformities of 10–15° is controversial. We report a case of a 60-year-old female patient with a 12° proximal tibia varus malunion treated with single-stage metaphyseal osteotomy and TKA, describing how stem-only fixation is capable of inducing union rapidly along with superb early function without the dangers of extensive intra-articular resection.
CASE PRESENTATION
Pre-operative Assessment
A 60-year-old woman with a BMI of 29 kg/m² presented with worsening right knee pain, intermittent knee buckling, and difficulty descending stairs. Fifteen years earlier, she had undergone a tibial tubercle osteotomy (TTO) at an outside facility to address recurrent patellar dislocation. Four weeks after the TTO, she experienced a fall from standing that caused immediate pain in the upper part of her leg. Initial radiographs taken at the outside facility were interpreted as showing no fracture. However, persistent discomfort led to repeat imaging ten weeks later, which revealed a proximal-third tibial shaft fracture that was already healing in varus alignment. Since the fracture showed bridging callus, no surgical intervention was offered at that time. Over the years, degenerative changes likely developed due to her varus malunion.
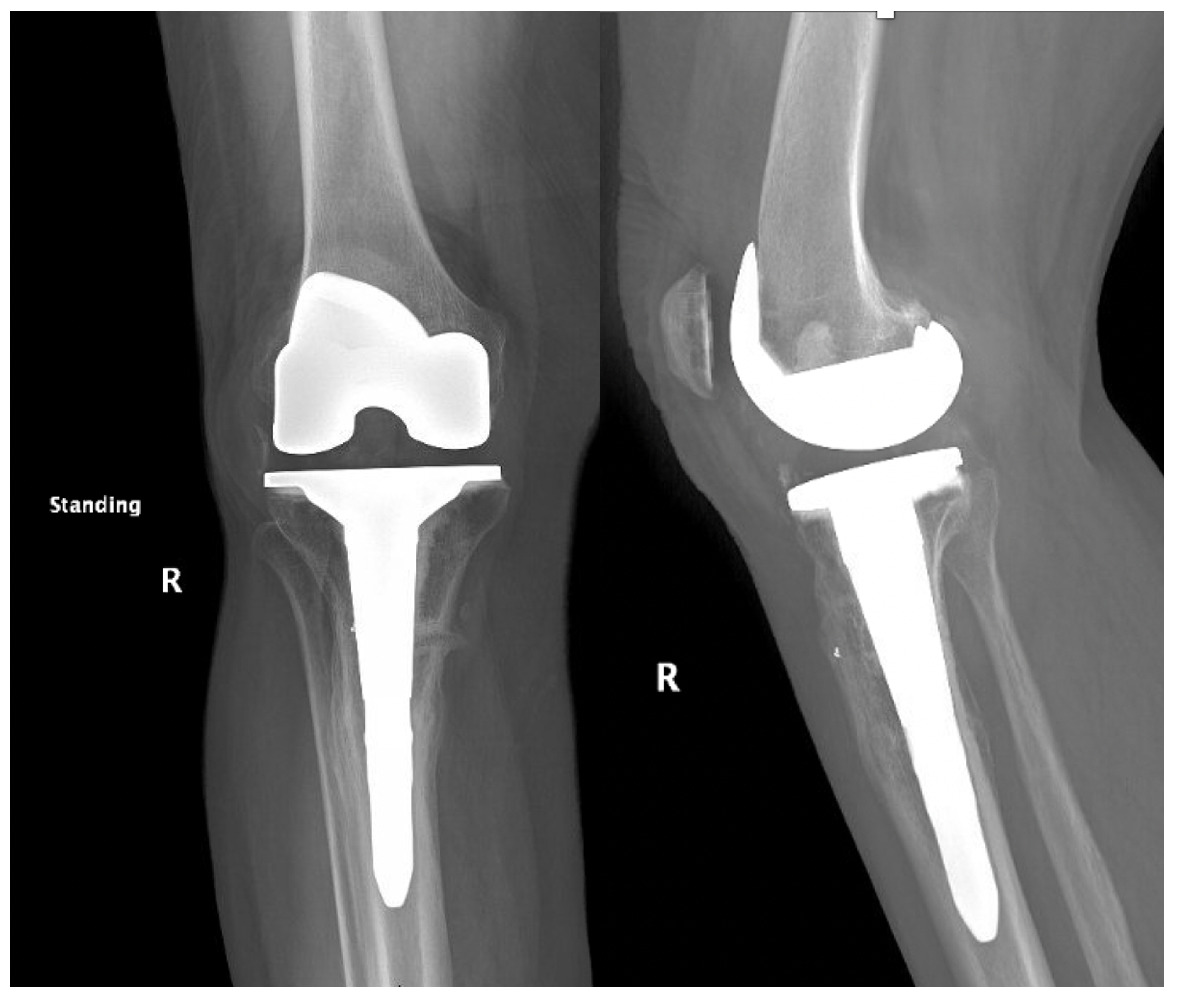
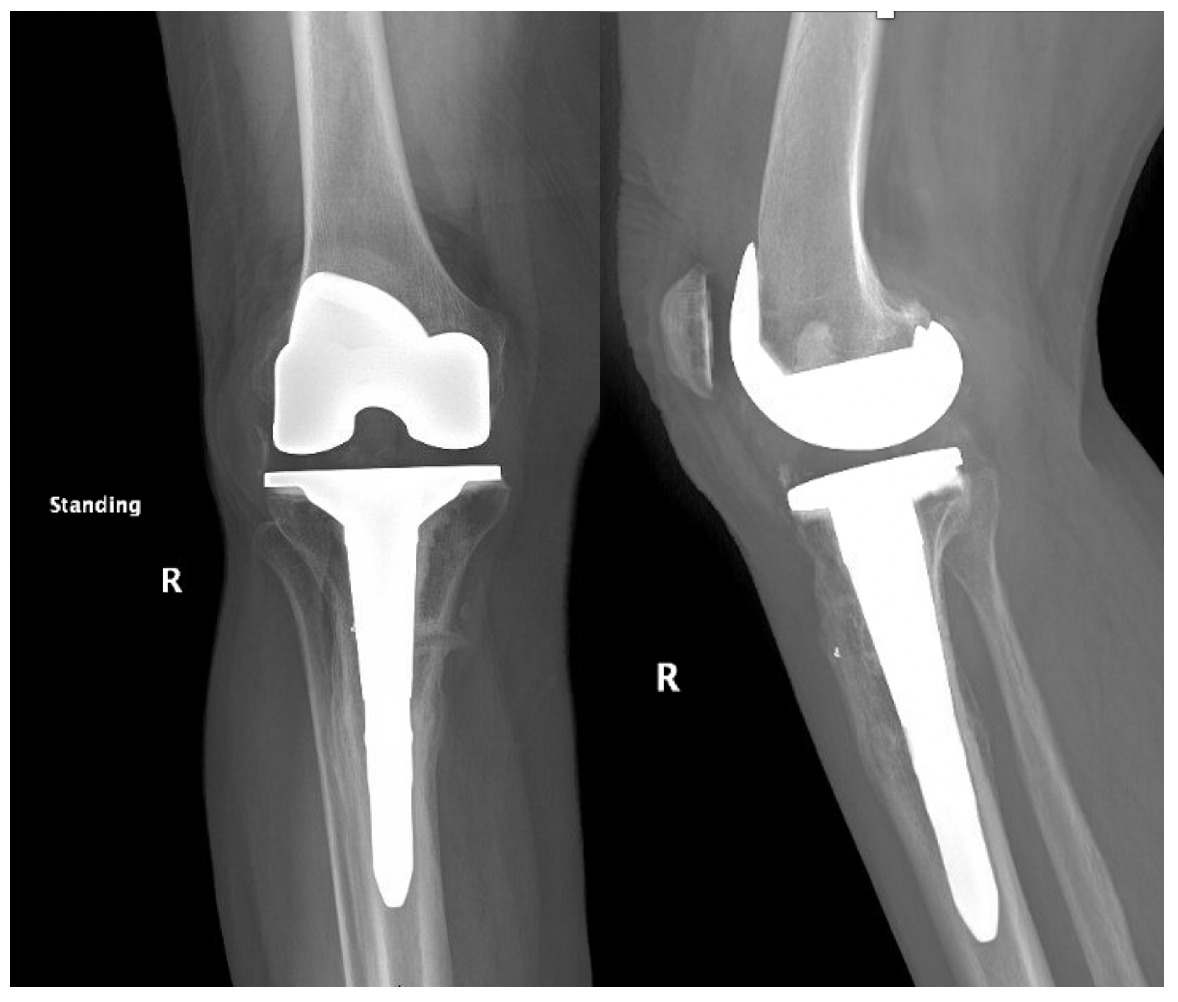
Pre-operative radiographs demonstrated Kellgren-Lawrence grade 4 tricompartmental osteoarthritis, 12° of tibial varus, a 22 mm deviation of the mechanical axis toward the medial side of the knee center, and an apex of angulation located 6 cm below the joint line (Figures 1 and 2). A follow-up computed tomography scan confirmed the absence of rotational malunion.

_radiograph_showing_12_tibia.png)
Physical examination disclosed active knee motion from 0° to 110°, a varus thrust during gait, and patellar subluxation near full extension. The collateral and cruciate ligaments were intact, and neurovascular integrity was preserved. Preoperative patient-reported outcomes included a Knee Society Score of 54 (pain 24, function 30) and a Knee Injury and Osteoarthritis Outcome Score for Joint Replacement (KOOS JR) of 49.
Surgical Technique
After induction of regional anesthesia, the patient was positioned supine on a radiolucent table with a tourniquet applied but left deflated. A midline skin incision was carried through the previous scar, and a standard medial parapatellar arthrotomy was performed. Dense fibrous tissue from the prior tibial tubercle osteotomy (TTO) was sharply excised to facilitate exposure.
The two TTO cortical screws were removed. Attention then turned to the extra-articular deformity. Under biplanar fluoroscopic control an oblique medial open-wedge osteotomy was created six centimeters distal to the tibial plateau at the apex of the varus malunion (Figure 3). A laminar spreader was gently inserted and opened until a neutral mechanical hip–knee–ankle axis was achieved, as confirmed with an extramedullary alignment rod extending from the center of the femoral head to the center of the ankle mortise.

A surgical assistant steadied the correction by holding laminar spreader and distal leg during tibial preparation. The tibial canal was sequentially reamed to accommodate a 15-mm diameter, 150-mm press-fit stem. Standard measured-resection technique was used on the femur with an intramedullary guide set to 6˚ of valgus. Femoral rotation was set to 4˚ of external rotation relative to the posterior condylar axis and parallel to the trans epicondylar axis—an amount chosen to optimize patellar tracking without over-stuffing the lateral compartment. The tibial proximal cut was made perpendicular to the mechanical axis with a targeted posterior slope of 3˚. Initial tibial component rotation was referenced to the medial one-third of the tibial tubercle and patellar tendon trajectory.
Trial components were inserted and demonstrated balanced flexion and extension gaps and central patellar tracking without the need for lateral release. The tibia was subsequently punched after confirming appropriate rotation for adequate patellar tracking. Final implantation proceeded with pressurized cement for the posterior-stabilized femoral component and the tibial baseplate under tourniquet insufflation. The diaphyseal press-fit stem was again confirmed to span the osteotomy by more than two cortical diameters under fluoroscopic guidance (Figure 4). Autogenous cancellous graft harvested from the femoral chamfer cuts was tightly packed into the osteotomy gap and along the medial cortex. The patella was resurfaced with a medialized polyethylene button.

After copious irrigation, the arthrotomy and extensor mechanism were closed in layered fashion over a closed-suction drain. A sterile dressing and a hinged knee brace locked in full extension were applied. The patient was allowed full weight bearing as tolerated with the brace, and physiotherapy was initiated on post-operative day one. Chemoprophylaxis against venous thrombo-embolism consisted of re-initiation of her home medication of apixaban 2.5 mg twice daily.
Post-operative Course
The total estimated blood loss was 300 mL, and no transfusion was required. The patient tolerated oral intake on the evening of surgery, completed her first physiotherapy session the following morning, and ambulated fifty feet with a rolling walker while wearing the hinged knee brace locked in extension. Following ambulation, full length lower extremity films were re-obtained, demonstrating neutral mechanical hip–knee–ankle axis (Figure 5). She was discharged home on post-operative day two with acceptable pain control and an incision that was clean, dry, and intact.

Quantitative range-of-motion and outcome-score data are summarized in Table 1. At the two-week clinic visit the incision was fully healed and sutures were removed. The patient continued full weight bearing in the brace. By six weeks the osteotomy displayed bridging callus across the osteotomy site (Figure 6), the brace was discontinued, and she achieved an unrestricted gait pattern without assistive devices. Four months after surgery, the patient had resumed activities such as tennis and reported no pain or swelling. Radiographs at that time demonstrated complete cortical union without any interval changes in alignment (Figure 7). At the nine-month assessment she reported hiking up to five miles and skiing on groomed slopes without limitation. Imaging showed continued consolidation of the osteotomy and stable components (Figure 8).


DISCUSSION
Historically, managing extra-articular coronal deformities during TKA has relied on established angular thresholds to determine whether correction should be intra-articular or extra-articular. Historically, tibial deformities exceeding 15° or femoral deformities greater than 20° could not be corrected intra-articularly without risking damage to the collateral ligament attachments (Wolff, Hungerford, and Pepe 1991). Subsequent research has confirmed that aggressive intra-articular resections may elevate the joint line, destabilize the medial collateral ligament, and increase the need for constrained bearings—factors associated with lower Knee Society Scores and higher revision rates when the postoperative mechanical axis deviates by more than 3° from neutral (Wang and Wang 2002; Laskin 2002; Park et al. 2018; Oh et al. 2018).
Our patient presented with a borderline deformity: 12° of metaphyseal varus located 6 cm below the joint line. Planning for intra-articular correction suggested an additional 11 mm of medial tibial resection, which would have jeopardized the medial collateral ligament’s attachment and raised the joint line by 4 mm. Given the patient’s high activity goals, the limited options for adjusting joint line elevation (with augment sizes available only in 5 mm, 10 mm, etc.), and the established link between joint line elevation and mid-flexion instability (Laskin 2002), we opted for a single-stage metaphyseal osteotomy stabilized by a long press-fit stem.
Meta-analyses comparing staged high-tibial osteotomy followed by delayed TKA, simultaneous osteotomy and TKA, and aggressive intra-articular bone resection show similar ten-year implant survivorship. However, staged procedures carry higher early complication rates (Oh et al. 2019). Simultaneous osteotomy corrects alignment in one procedure, preserves ligament tension, and avoids a second anesthesia, though it may slightly increase operative time and blood loss. In Catonné’s prospective series of 26 knees, all osteotomies healed within three months, and patients achieved a mean International Knee Score of 98 at nine years (Catonné, Sariali, Khiami, et al. 2019)—results that align with the rapid union and excellent early function seen in our case.
Traditional fixation methods often used plates or intramedullary nails, which require more dissection and can interfere with component positioning. Biomechanical studies indicate that a diaphyseal-engaging stem that bypasses the osteotomy by at least two cortical diameters provides rigidity comparable to plate constructs, without the added risk of hardware-related soft tissue irritation (Ishida, Tsumura, Takayama, et al. 2011; Lai et al. 2022). Papagelopoulos et al. reported 100% union with stem-only fixation across deformity sites (Papagelopoulos et al. 2007).
Studies focusing on intra-articular correction for moderate deformities report mean postoperative Knee Society Scores (KSS) ranging from 68 to 85, often requiring constrained inserts or resulting in elevated joint lines (Loures et al. 2019; Wang and Wang 2002). In contrast, simultaneous osteotomy groups demonstrate better functional scores and more durable alignment—Catonné’s series averaged a KSS of 98 at long-term follow-up (Catonné, Sariali, Khiami, et al. 2019). Our patient achieved a KSS of 95 and a KOOS JR of 90 at nine months, supporting the idea that restoring neutral mechanics while maintaining ligament tension promotes favorable early function. Registry data further suggest that neutral or slight varus alignment is ideal for implant longevity (Park et al. 2018; Oh et al. 2018), reinforcing the choice of extra-articular correction when intra-articular techniques would leave residual malalignment.
The major limitation of this report is its single-patient study design with nine-month follow-up. However, the prompt union, neutral mechanical axis, and exceptional functional recovery are consistent with findings from larger prospective cohorts. Future research should include gait analysis, cost-effectiveness data comparing stem-only with plate-assisted fixation, and randomized trials assessing the incremental benefit of navigation or robotic assistance for osteotomy planning.
In summary, single-stage metaphyseal osteotomy stabilized using a long tibial stem can safely manage borderline proximal tibial deformity during primary TKA, achieving rapid union, immediate full weight-bearing, and excellent early patient-reported outcomes. Surgeons should personalize decision-making rather than adhering to strict, rigid angular thresholds.