INTRODUCTION
Wrist denervation is a well-established treatment option for carefully selected patients with chronic pain due to wrist arthrosis, carpal osteonecrosis, or other wrist maladies and for whom conservative measures have not provided symptomatic relief (Wu and Strauch 2019). The typical patient is a middle-aged adult who is unwilling to risk the potential morbidity associated with surgical interventions such as wrist arthrodesis or arthroplasty which directly address the intracarpal pathology. For many patients, a reasonable alternative procedure is wrist denervation wherein the articular nerve branches to the radiocarpal joint are transected to reduce wrist pain without producing motor or sensory loss (Wu and Strauch 2019).
Wilhelm performed the first wrist denervation procedure in 1959 after reporting his cadaver studies on wrist joint neuroanatomy in the German medical literature. He advocated for total wrist denervation using a 5-incision surgical technique featuring articular branch neurotomies of multiple nerves including the posterior interosseous, superficial radial, lateral and posterior antebrachial cutaneous, and anterior interosseous nerves (Wilhelm 2001). Although early patient outcomes were reported as favorable (Geldmacher, Legal, and Brug 1972; Buck-Gramcko 1977), complications such as dysesthesia, painful neuroma, and complex regional pain syndrome were later recognized (Smeraglia et al. 2020), tempering enthusiasm for the procedure.
Subsequently, Berger proposed a surgical technique for partial wrist denervation (PWD) which included neurectomies limited to the posterior interosseous nerve (PIN) and the anterior interosseous nerve (AIN) just proximal to the distal radioulnar joint (DRUJ). At this location, separated only by the interosseous membrane (IOM), the adjacent nerves are easily approached and segmentally resected through a single dorsal incision (Berger 1998). As cadaver dissections have shown that the PIN innervates the central two thirds of the dorsal radiocarpal joint (Fukumoto et al. 1993; Van de Pol et al. 2006) and that the AIN is the most important contributor to palmar wrist innervation (Van de Pol et al. 2006), there is clearly an anatomic basis for the efficacy of PWD. Technically simple, single-incision PWDs focusing only on the articular branches of the PIN and AIN are now the most common wrist denervations performed in the United States (Milone, Klifto, and Catalano 2018).
With the emergence of wide-awake local anesthesia no tourniquet (WALANT) technique in hand surgery (Hearon, Isaacs-Pullins, and Lalonde 2023), many hand and wrist procedures formerly done in hospital operating rooms under tourniquet control and regional or general anesthesia are now being performed in outpatient surgery centers with wide-awake anesthesia and no tourniquet. In this context, the purposes of this manuscript are to review the indications and contraindications for wrist denervation, to describe our approach to PWD using the WALANT technique, and to document our method for diagnostic block of the PIN and AIN to confirm that PWD is well indicated.
INDICATIONS AND CONTRAINDICATIONS
Skeletally mature patients with carpal pathology causing chronic wrist pain resistant to nonoperative management and with only mildly restricted wrist motion should be strongly considered for PWD (Kadiyala and Lombardi 2017). This palliative, motion-sparing procedure is indicated for selected patients with post-traumatic arthrosis of the radiocarpal and/or midcarpal joints, often presenting as scaphoid nonunion advanced collapse (SNAC) wrist or scapholunate advanced collapse (SLAC) wrist (Berger 1998; O’Shaughnessy et al. 2019). Those with wrist osteoarthrosis or inflammatory arthritis (O’Shaughnessy et al. 2019; Peltz et al. 2019) may also be good candidates for PWD, as are some patients with osteonecrosis of the scaphoid (Preiser disease) or lunate (Kienbock disease).
Contraindications to PWD include septic arthritis of the wrist or other active infection, poor patient cognition, or unreasonable patient expectations regarding the surgical outcome (Kadiyala and Lombardi 2017). Those with markedly restricted wrist motion from diffuse arthrosis are not good candidates for PWD and are better served by limited intercarpal arthrodesis, total wrist arthrodesis, or total wrist arthroplasty. Similarly, patients with post-traumatic radiocarpal incongruity after intra-articular distal radius fracture should be considered for corrective osteotomy of the distal radius or other procedures targeted directly at the underlying wrist pathology.
Contraindications to using the WALANT technique for PWD are few. An absolute contraindication is true lidocaine allergy which, although exceedingly rare, should be assessed with a subcutaneous challenge test (Hearon, Isaacs-Pullins, and Lalonde 2023) by an allergist or other knowledgeable expert. Patient anxiety regarding the wide-awake method is a relative contraindication which may be ameliorated by preoperative patient education (Jagodzinski, Phillips, and Lalonde 2022).
INJECTION AND SURGICAL TECHNIQUES
Preparations for Diagnostic Injection
The rationale for diagnostic injection to block the PIN and AIN should be discussed with the patient beforehand and informed consent should be obtained and documented. The patient should understand that the short-acting lidocaine injection may produce temporary wrist pain relief for about an hour. In our experience, a positive response to the injection may predict wrist pain relief following PWD, whereas a negative response suggests that PWD may be of little benefit.
Pre- and post-injection pain severity at rest and with wrist motion should be rated on a 0-10 Visual Analogue Scale (VAS) where 0 indicates no pain and 10 designates severe pain. Also, percentage pain relief should be estimated on the day of the injection before the patient leaves the office when the assessment is most reliable. Pain relief estimation deferred until a follow-up visit is subject to recall bias.
In preparation for the injection, the patient may be seated in a comfortable chair or, preferably, may be positioned supine on an exam table. In either the seated or recumbent position, the affected pronated forearm should be well supported on an adjacent arm board or hand table. Precautions for injection-induced vasovagal syncope are appropriate.
Technique for Diagnostic Injection
Two mL of 1% lidocaine without epinephrine is drawn into a 5-mL syringe. After skin prep with alcohol, the injection is administered through a 1½-inch, 25-gauge needle. The bony landmarks for the injection are Lister’s tubercle and the dorsal sulcus between distal radius and ulna. The site of injection is 1 cm ulnar and 3 cm proximal to Lister’s tubercle (Grutter et al. 2004) near the ulnar border of the distal radius on the dorsal wrist.
The needle is introduced perpendicular to the skin and is directed toward the radial shaft beneath the fourth dorsal compartment. This compartment contains the extensor indicis proprius (EIP), extensor digitorum communis (EDC), and the PIN before it arborizes into its terminal branches to innervate the dorsal wrist joint capsule. A small volume, not more than ¾-1 mL of 1% lidocaine, is injected into the fourth dorsal compartment to anesthetize the PIN.
The needle is then redirected and minimally advanced in the palmar direction across the ulnar border of the radial shaft and through the IOM. In some cases, mild resistance is appreciated as the needle penetrates the IOM. With the needle tip in this location just anterior to the IOM, about ¾-1 mL of 1% lidocaine is injected to anesthetize the AIN. The needle is withdrawn, and Band-Aid applied.
Following the injection, the patient is observed for a minimum of 15-20 minutes as the anesthetic sets up. Wrist pain improvement at rest and with provocation is assessed before the patient is dismissed. At least 50% pain relief is our threshold to indicate the patient for elective PWD.
Preparations for Partial Wrist Denervation
Suitable venues for this minor outpatient surgery include an ambulatory surgery center (ASC) or a well-appointed office-based procedure room (OPR). Using a hospital operating room is not cost-efficient in most settings (Leblanc, Lalonde, and Lalonde 2007). Intravenous (IV) access for sedation is not required, and the procedure may be accomplished using field sterility technique (LeBlanc et al. 2011) at the surgeon’s discretion.
When PWD is performed as a standalone procedure, WALANT technique is our preferred method of anesthesia. Local anesthesia is administered in the ASC preoperative holding area or in the OPR with the patient supine and the affected upper limb well supported. The goal is to anesthetize the distal one third of the dorsal forearm in preparation for a 3-4 cm incision between the radius and ulna in the surgical approach for the denervation.
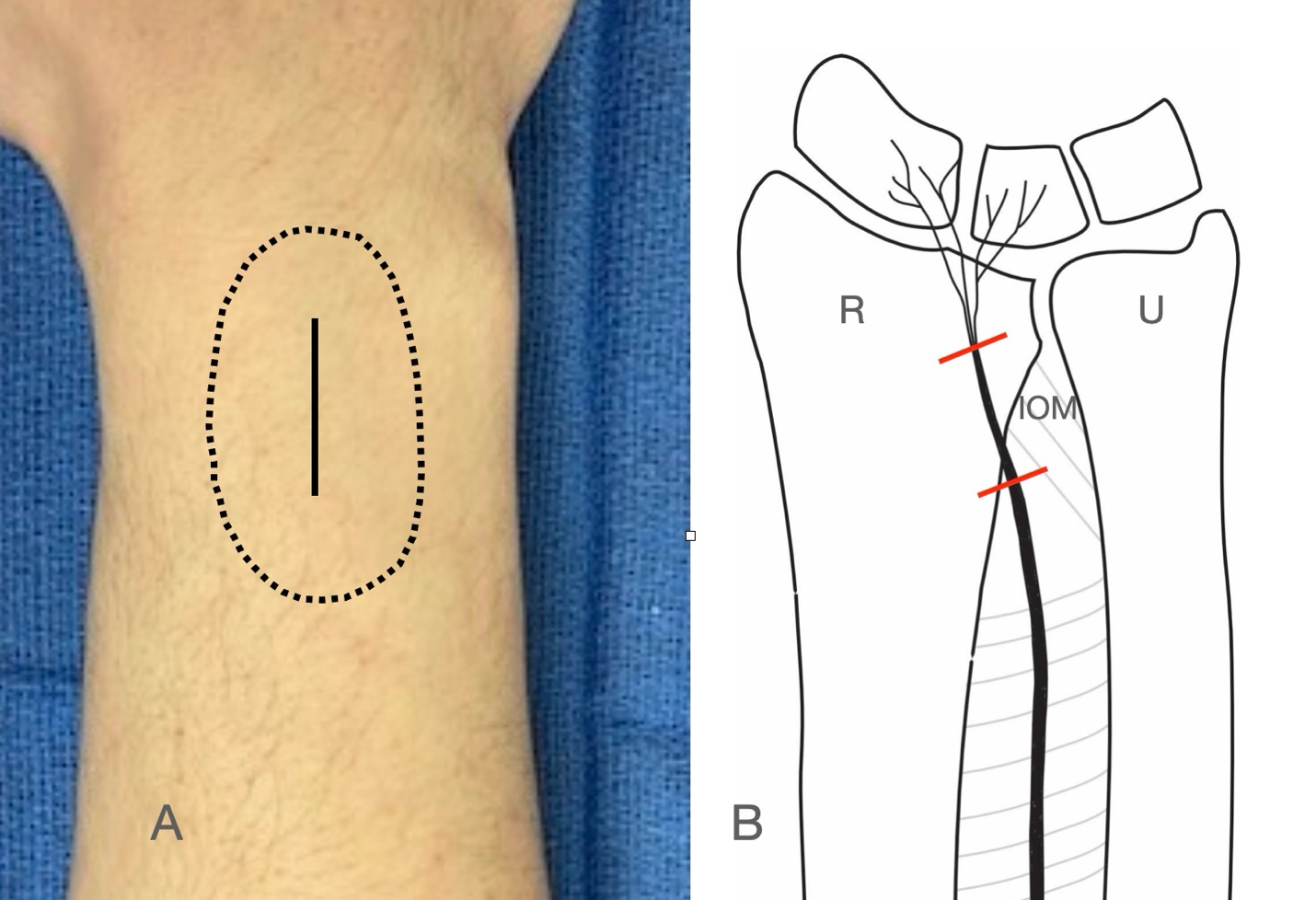
Two 10-mL syringes are filled with 1% lidocaine with 1:100,000 epinephrine which may be buffered with 8.4% sodium bicarbonate in a 10:1 lidocaine to bicarbonate ratio (Lalonde 2022). After alcohol prep of the dorsal forearm, the anesthetic is administered through a 1½-inch, 25-gauge needle using tumescent technique targeting an area as shown in Fig. 1A. The total volume used is 15-20 mL depending upon patient size. This small volume is within the conservative dosing limit for lidocaine of 7 mg/kg body weight. To assure the vasoconstrictive effect of the epinephrine, thereby minimizing intraoperative bleeding and optimizing visualization, the anesthetic should be allowed to set up for at least 25 minutes before making the skin incision (McKee et al. 2013).
Surgical Technique for Partial Wrist Denervation
The patient is placed supine on the operating table with the affected upper extremity supported on an adjacent arm board or hand table. No IV access or pneumatic tourniquet is required. However, owing to the proximity of the perineural vasculature, bipolar electrocautery is often used to assure hemostasis. The forearm is prepped with Betadine scrub followed by alcohol and the patient is draped in a standard fashion. The operative procedure is performed using 4.5x loupe magnification to help identify the AIN which is approximately 1 mm in diameter at the level of resection.
The surgical method for PWD emulates that described by Berger with modification to accommodate the WALANT technique. After allowing about 25-30 minutes for the anesthetic to setup, an approximate 3-4 cm longitudinal skin incision is made centrally on the dorsum of the anesthetized distal forearm, starting 2 cm proximal to the wrist and extending proximally. Dorsal veins are mobilized and retracted or suture-ligated and divided. The subcutaneous layer is dissected and elevated from the deep antebrachial fascia. Depending on the thickness and permeability of the deep antebrachial fascia, the anesthetic may be supplemented at this point during the procedure by introducing 1-3 mL of 1% lidocaine with 1:100,000 epinephrine directly into the fourth dorsal compartment and then waiting a few minutes for the anesthetic effect.
The deep fascia is opened with a 69 Beaver blade, the EIP and EDC tendons are retracted ulnarly, and the PIN terminal branch is identified on the floor of the fourth dorsal compartment adjacent to the distal radius. After carefully dissecting the nerve from the accompanying posterior branch of the anterior interosseous artery, a 2 cm segment of the PIN is resected (Fig. 1B). The specimen is usually discarded but may be sent for histologic confirmation of tissue type if warranted.
_clinical_photo__right_dorsal_wrist_and_distal_forearm._area_designated_by_the_dotted_.jpeg)
Next, the IOM distal to the distal oblique bundle is sharply incised longitudinally exposing the deep head of the pronator quadratus. The 1-mm wide terminal sensory branch of the AIN, which is often accompanied by the anterior interosseous artery and its venae comitantes, is found on or closely adjacent to the anterior surface of the IOM. The terminal AIN is segmentally resected, hemostasis is achieved with bipolar electrocautery as needed, and the excised 1-2 cm nerve segment is discarded. To preserve the AIN motor branches innervating the pronator quadratus, the AIN must be resected not more than 2 cm proximal to the DRUJ (Grafe et al. 2005).
Wound Closure and Aftercare
The IOM and antebrachial fascia are left open, while the skin subcuticular layer is closed with interrupted and inverted 4-0 resorbable monofilament suture. A small compressive dressing held in place with Coban is applied to the wound. No immobilization is required.
The patient is dismissed from the ASC or OPR with instructions to take mild non-opioid analgesics for wound pain, to keep the wound clean and dry for a minimum of 3 days, and to avoid sports or lifting activity. Wound check occurs 10-14 days after surgery. If the incision is well healed and recovery uneventful, then the patient may resume regular activity as tolerated.
Representative Case
A 78 year-old right-hand dominant retired attorney presented with an 18-month history of right wrist pain which interfered with his ability to play golf. He described a variable sharp pain localized to the dorsoradial wrist, aggravated by radial-to-ulnar wrist motion and by golfing back swing. Pain had increased over the preceding 3 months. He denied antecedent wrist trauma and previous wrist surgery.
Physical exam of the right wrist revealed dorsiflexion 60°, palmar flexion 35° with pain, radial deviation 5°, and ulnar deviation 35°. There was tenderness over the dorsal carpus at the capitolunate articulation. Plain radiographs of the wrist revealed increased scapholunate diastasis with radioscaphoid and capitolunate arthrosis consistent with stage III SLAC wrist.
Diagnostic block of the PIN and AIN produced 50% temporary pain relief. In keeping with our treatment algorithm, the patient underwent PWD using the WALANT technique. At 6 weeks post-surgical follow-up, the patient’s wrist pain had improved. At 5½-year follow-up, the patient denied any wrist pain whatsoever, having required no interim wrist surgery. On 0-10 VAS, he rated his satisfaction with PWD as 10, stating he would choose to have the procedure again for similar indications, and he would recommend the procedure to others.
DISCUSSION
Since first using the WALANT technique for PWD over a decade ago, our experience has been associated with high patient satisfaction, as in the case presented, and lower overall cost in part because the patient does not incur a separate anesthesia fee. This minor surgery also requires few, if any, opioids during the recovery period. Thus, we continue to advocate for the innovative wide-awake anesthesia method in patients indicated for PWD as a standalone procedure. Of course, use of the WALANT technique is not imperative for a successful surgical outcome.
As enumerated elsewhere (Berger 1998), the advantages of PWD compared with other salvage procedures such as partial or total wrist arthrodesis include technical simplicity, shorter operating time, lower cost with no need for fusion plates or other implants, fewer potential surgical complications, shorter postoperative recovery time, and possibly better wrist motion. Moreover, PWD does not preclude a secondary wrist arthrodesis or other salvage procedure if the denervation does not yield a satisfactory outcome. We have found that PWD is particularly useful in geriatric patients who want to shorten postoperative recovery and in those with medical co-morbidities for whom a more invasive procedure increases the likelihood of a surgical complication.
Although disruption of wrist proprioception resulting in Charcot arthropathy has been raised as a potential complication of PWD, no such procedure-related adverse events have been found in published case series. For instance, in 195 patients treated with wrist denervation and followed an average of 4.1 years, no Charcot-like joints were seen (Buck-Gramcko 1977). In a smaller series of 19 patients (20 PWDs) with mean follow-up of 2.5 years, no complications related to the surgery were reported (Weinstein and Berger 2002). Furthermore, a study 23 patients after posterior interosseous sensory neurectomy showed no significant decrease in wrist proprioception (Patterson et al. 2010). The authors concluded that Charcot arthropathy is unlikely after PWD because there are other sensory nerve branches innervating the wrist and intact neuroreceptors in the adjacent skin and muscle which also contribute to proprioception.
Preoperative education establishing patient expectations following PWD is key to a successful outcome. Patients must understand that PWD is intended to improve their pain profile, but not necessarily to eliminate their wrist pain. In fact, an acceptable early postoperative result may be followed by increasing wrist pain over time owing to underlying disease progression. For instance, although patients with early SLAC or SNAC wrist and functional wrist motion demonstrated good short-term wrist pain improvement after PWD in some studies (Weinstein and Berger 2002; Abdelaziz et al. 2019), longer-term outcomes showed increasing revision rates (O’Shaughnessy et al. 2019). In the latter study, the overall survival rate of the denervation regardless of surgical indication was 85% at 1 year, 71% at 5 years, and 57% at 15 years, illustrating that symptomatic relief of wrist pain wanes over time.
Judicious patient selection for PWD should also focus on excluding poor candidates for the procedure. For example, patients with limited active wrist motion are likely to be early treatment failures (Weinstein and Berger 2002) and, therefore, have an absolute contraindication. Those with predominantly ulnar-sided wrist pain localized to the distal ulna and/or the DRUJ are also unlikely to benefit from PWD and are considered to have a relative contraindication (Peltz et al. 2019). Similarly, patients with unsettled workers’ compensation claims (Weinstein and Berger 2002) or other secondary gain issues (Sgromolo et al. 2018) are not reliable candidates for denervation.
Although the utility of preoperative injections in candidates for PWD has been debated, we strongly favor blocking the PIN and AIN as a diagnostic tool in the preoperative assessment. In our experience, a positive diagnostic injection test portends a good outcome, whereas a negative test often predicts a treatment failure. In early studies (Dellon 1985; Berger 1998) investigators advocated for preoperative injections, but later studies suggested that diagnostic injections had poor predictive value (Weinstein and Berger 2002; Hofmeister, Moran, and Shin 2006). Confirming that injections have fallen out of favor, a recent survey of surgeon-members of the American Society for Surgery of the Hand found that only 19% of respondents always used preoperative lidocaine block as an aid in the decision-making process (Kale, Foote, and Medvedev 2022). Of course, even with good pain relief from a diagnostic injection, a satisfactory outcome following PWD cannot be guaranteed (Kadiyala and Lombardi 2017). The difference between post-injection and post-denervation wrist pain may be due to multiple factors including surgical scarring, incomplete denervation, and variations in injection technique (Sgromolo et al. 2018).
Importantly, injection location and volume of anesthetic administered may influence the predictive value of the diagnostic block. In our technique, ¾-1 mL of lidocaine is introduced into the fourth dorsal compartment to block the PIN, and the same small volume is placed just anterior to the IOM to anesthetize the AIN. If both nerves are precisely blocked, then the potential efficacy of PWD may be accurately estimated. However, if the injection is poorly located and the target nerves are missed, then PWD effectiveness is underestimated. Conversely, using an excessive volume of lidocaine may unintentionally block other sensory afferent nerves at the wrist leading to an overly optimistic estimate of pain relief after PWD (Milone, Klifto, and Catalano 2018; Sgromolo et al. 2018). In this regard, serial blocks with long-acting local anesthetics to improve the reliability of injections as a predictor of surgical outcome have been recommended (Weinstein and Berger 2002).
CONCLUSION
Patients with chronic wrist pain from post-traumatic arthrosis, carpal osteonecrosis, or other etiologies who have retained functional wrist motion should be considered for PWD as an alternative to more invasive wrist salvage procedures such as wrist arthrodesis or arthroplasty. In our experience, a minimum of 50% wrist pain relief after diagnostic lidocaine block of the PIN and AIN using our preferred technique is a prerequisite for an operative indication. PWD may be safely performed in an ASC or OPR using the WALANT technique innovation with the expectation of few complications, high patient satisfaction, and reduced procedure cost.