


Introduction
Degenerative pathology of the lumbar spine such as spondylolisthesis, scoliosis, and degenerative disc disease are leading causes of global disability and diminished quality of life (Chu, Clark, and Angst 2006; Kalichman et al. 2010). When symptoms are refractory to conservative management, minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) offers an effective treatment option via restoration of disc height and vertebral alignment through a stable fused spinal segment (Holly et al. 2006; Cole et al. 2009). Compared to the open procedure, MIS TLIF has been associated with similar long-term positive clinical and radiographic outcomes, with the additional benefit of less postoperative pain, earlier rehabilitation, shorter length of hospital stay, and diminished complication rate (Peng et al. 2009). This success has contributed to the consistent annual increase in the number of MIS TLIF procedures performed over the past decade (Kobayashi et al. 2018).
Given the continued increase in frequency of the procedure and advancements in perioperative medicine, there has been a growing interest in the safe transition of MIS TLIF to the outpatient and ambulatory surgery center settings (Emami et al. 2016; Bovonratwet et al. 2018). This trend may contribute to considerable cost savings through decreased utilization of hospital resources, less narcotic usage, and faster returns to work (Adogwa et al. 2011). Despite this potential, the procedure has yet to widely adopted in the outpatient and ambulatory surgery center settings.
Our team performs a high volume of elective MIS TLIF procedures, a majority of which take place on an outpatient basis. Only recently have we been able to obtain insurance authorization and payment for the 22633 TLIF CPT code in our stand-alone ambulatory surgery center. As such approximately, 50 MIS TLIFs have been performed in the ASC setting. Previously we have reported our extensive MIS TLIF experience in an outpatient hospital setting. By critically analyzing our practices and adopting methods of standardization and efficiency from other areas of orthopaedic surgery, we have safely and effectively made the transition to the outpatient setting. In this paper, we highlight some of the key principles of this standardization such that other teams can learn from our example and consider similar changes to their own clinical practice.
Lessons from Hip and Knee Arthroplasty
Hip and knee arthroplasty are amongst the most common procedures performed by orthopaedic surgeons annually (Eltorai et al. 2018). Once requiring a multi-day hospital stay, recent advancements in patient care have resulted in an explosion of total joint arthroplasty being performed in the outpatient setting. In fact, over the next five to ten years, it is estimated that outpatient total joint arthroplasty will increase by 70% while the inpatient procedure is anticipated to increase by only 3% over the same time frame (Bert, Hooper, and Moen 2017). The success of this transition has been made possible by patient selection protocols, intraoperative efficiency, multimodal analgesic regimens, and synchrony with anesthesia.
Osteoarthritis of the hip and knee follow a predictable cascade and many patients become surgical candidates for total joint arthroplasty after failing conservative management. The procedure itself follows routine, reproducible steps, with minimal variation (Robinson et al. 2006; Lingard, Berven, and Katz 2000). In degenerative lumbar spine surgery, on the other hand, there is an attitude that a wide range of pathologies and indications for surgical intervention result in a high degree of procedural and technique variability. It is the belief of our group that, despite differences in baseline pathology, surgical technique is largely unchanged. This attitude has empowered our team to learn from our arthroplasty colleagues and introduce methods of standardization to improve the safety and efficiency of the MIS TLIF in the outpatient setting.
Patient Selection
Successful outpatient MIS TLIF surgery begins with identification of an appropriate patient. Based on their clinical experience with a number of outpatient spine procedures, Chin et al. proposed criteria for a good outpatient candidate. These included living within 30 minutes of a hospital, body mass index (BMI) of less than 42, clearance from a general practitioner and/or cardiologist, American Society of Anesthesiologists (ASA) Physical Function Score of 3 or less, and a responsible adult living with the patient (Chin et al. 2017). Although age was not identified as a criterion by these authors, other studies have found that age greater than 65 is a substantial risk factor for postoperative complications following lumbar surgery in the outpatient setting (Lang et al. 2014; Fleisher et al. 2004).
Our group urges caution when considering outpatient MIS TLIF in patients over 65, diabetics, and those with an ASA score of 3 or higher. Unlike inpatient lumbar fusion surgery, it is also critical to evaluate anxiety levels and social support for patients being considered for outpatient fusion surgery. Many patients, even those without formally diagnosed anxiety disorders, may share concerns regarding postoperative pain, being able to care for themselves, and mobility (Strøm et al. 2018). Preoperative screening and education is therefore critical, and treatment of said anxiety prior to surgery may ultimately improve long term outcomes (Adogwa et al. 2016). Despite the aforementioned criteria and cutoffs, a large number of patients are good candidates for outpatient MIS TLIF. We typically utilize criteria including an ASA scoring of 2 or less, BMI of 38 or less, and a responsible care-giver at home to observe the patient for the first 23 hours. Of patients that underwent outpatient TLIF since 2016, the mean age was 47.0 (range 30.3-64.7) and mean BMI was 27.6 (range 18.6-37.8) (Table 1). All outpatient TLIF procedures were performed at a single level. We have not been able to successfully negotiate with the commercial payers regarding a multi-level TLIF in a stand-alone ASC and as such it is currently cost-prohibitive to perform such procedures in our geographic market. Preoperative spinal diagnoses for patients undergoing outpatient MIS TLIF included degenerative spondylolisthesis, isthmic spondylolisthesis, and herniated nucleus pulposus (Table 2).
Intraoperative Efficiency
Ambulatory surgery center staff training and standardization of instrumentation are key steps to the safe adoption of high-volume outpatient spine surgery. In current practice settings, spine surgery oftentimes features a high degree of variability (Daffner, Beimesch, and Wang 2010; Aubin, Labelle, and Ciolofan 2006). Consider for example that spine teams, even those at the same institution, may perform the same procedure using different operating room tables, microscopes, surgical instruments, and implants. Total joint arthroplasty, on the other hand, typically follows uniform methods for patient positioning, procedural technique, and surgical instrumentation for a given hospital system. The adoption and instilment of similar standardized procedures in outpatient spine surgery is not only possible, but critical to success, safety, and efficiency.
Although not unique to the ambulatory setting, staff training for a high-volume, time-sensitive environment is essential to achieve the benefits offered by outpatient spine surgery. The ability of staff to train and become familiar with the steps and instrument sequencing of the MIS TLIF can strongly influence procedure duration. Moreover, awareness of a preferred operating room setup facilitates faster turnover and a potential for a greater total number of cases for a given surgical day.
Similarly, consolidation of instrument trays can contribute to increased efficiency and diminished costs. Cichos et al. reported their experience with tray consolidation in total joint arthroplasty at a single institution (Cichos et al. 2019). After querying their total joint arthroplasty surgeons, they removed 433 of 792 instruments from 11 unique instrument trays. The time saved as a result led to an estimated 20% overall cost reduction, and an annual savings over $250 thousand. Similar consolidation efforts can be successful in spine surgery, particularly for minimally invasive procedures.
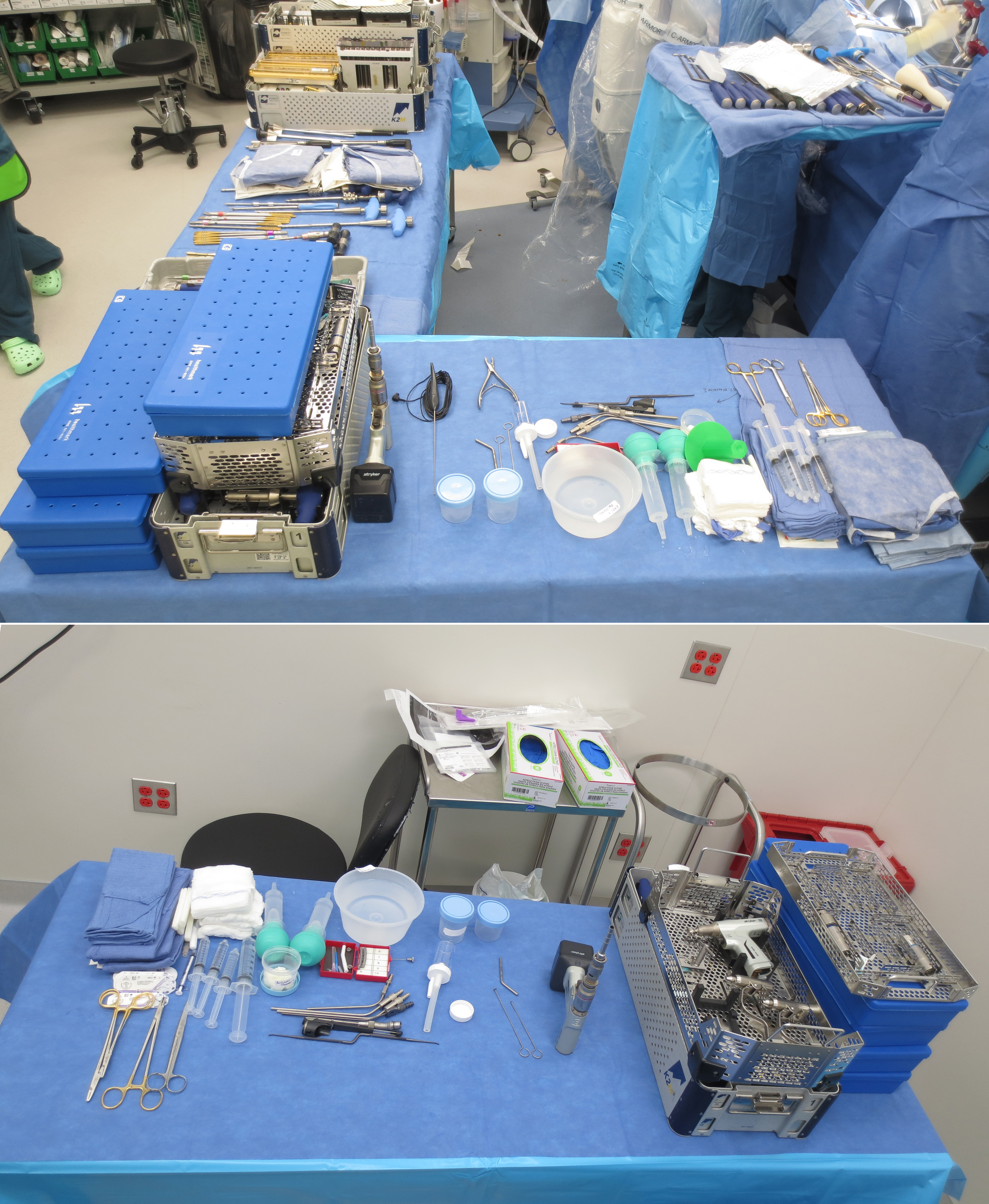
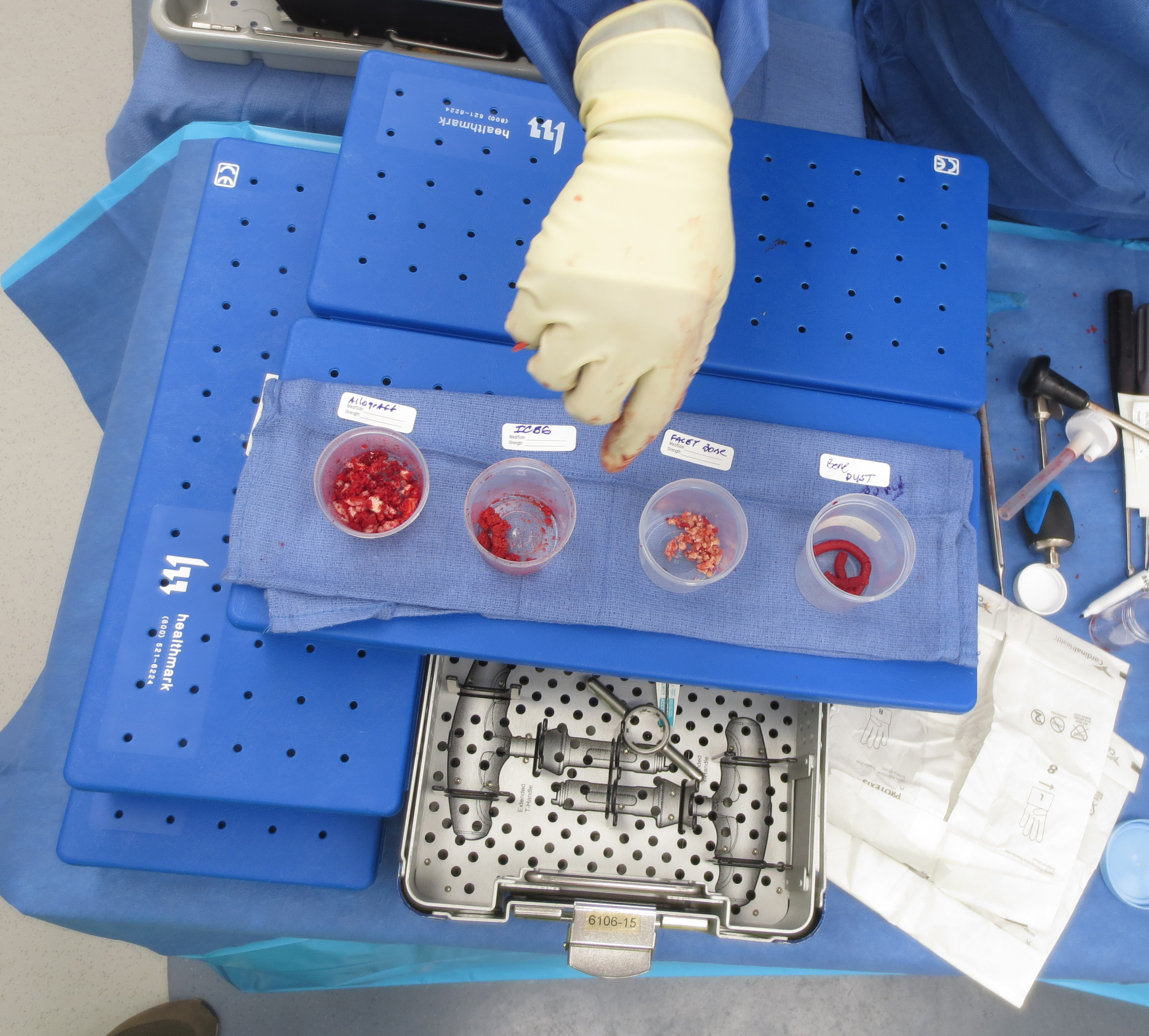
In traditional open spine surgery, different sets of retractors and instruments may be necessary based on the procedure being performed, the number of levels being operated on, and the patient’s body habitus. For minimally invasive surgery, however, the procedure takes place through a uniform-sized tube that not only limits iatrogenic harm to the paraspinal musculature, but also allows for a standardized surgical technique (Styf and Willén 1998). In our MIS TLIF, for example, once the facet joint of interest has been localized under fluoroscopy with a K-wire, a series of dilators are placed over the wire, and consistently a 20 mm non-expandable tubular retractor is placed and affixed to the surgical table. This same 20 mm tube is utilized regardless of the number of levels being instrumented or the patient’s body habitus. This contributes to not only surgeon comfort and efficiency, but also that of the surrounding surgical team. The instrument trays are also limited in number and are organized in a procedure specific fashion (e.g. percutaneous pedicle screw placement, decompression, iliac crest bone graft harvesting, and interbody fusion preparation, Fig. 1-6).






Multimodal Analgesia Protocol
As other aspects of the surgical process are standardized and streamlined, so too must the management of postoperative pain. In recent years, a multimodal analgesia protocol has been created and optimized by our practice which allows for decreased utilization of narcotic medications and their adverse side effect profiles while maintaining appropriate levels of pain control (Table 3) (Rajpal et al. 2010; Singh et al. 2017). This approach enables us to send patients home within 24-hours of surgery with appropriate pain control, which until recently was not feasible.
As its name suggests, multimodal analgesia uses several different medications that target multiple physiological pathways via different mechanisms of action. By utilizing this “multi-pronged” approach, lower doses of any one type of medication can be used, thereby minimizing the potential of dose-dependent adverse effects (Buvanendran et al. 2003). A diminished reliance on opioid medications in particular may reduce rates of a number of serious side effects (Singh et al. 2017). Furthermore, opioid medications frequently increase risk for postoperative nausea and vomiting, which can be a major barrier to successful outpatient surgery (Swegle and Logemann 2006; Garcia et al. 2013). Decreased opioid utilization can also lead to earlier mobilization, and can facilitate earlier participation in physical therapy (Berger et al. 2009). This streamlines the postoperative period and allows patients to initiate their recovery process more rapidly.
Our MMA protocol also emphasizes the importance of the preoperative window. Consistent and effective medication administration before surgery can allow medications more chance to accumulate in the body and proactively mitigate the inflammatory changes that occur in the operating room and during recovery as a result of surgical trauma (Buvanendran et al. 2005; Kim et al. 2006). In addition, proper preoperative patient counseling is just as vital to successful pain control and surgical outcomes as the medication protocol itself. Patients expectations must be assessed and managed regarding what recovery will entail, what clinical outcomes can be expected, and to what extent various medications will be made available. This dialogue is important for both surgeon and patient to determine together whether the proposed surgical protocol is a good fit for that particular patient, and vice-versa. An important part of managing these expectations is developing an understanding that narcotic medications should not need to be continued more than a few weeks postoperatively. Limiting longer-term narcotic usage can help avoid the development of tolerance as well as opioid-induced hyperalgesia, both of which are associated with increased pain and poorer clinical outcomes (Chu, Clark, and Angst 2006; Koppert and Schmelz 2007; Lee et al. 2011). This can also reduce the pressure on physicians and office staff to re-prescribe pain medications.
Finally, it is important for the anesthesia and surgical staff to collaborate closely in order to maximize pain control, while minimizing adverse effects and length of stay. This can entail involvement of the anesthesiologist at the time of the preoperative office visit to help determine whether the patient is a good candidate for the MMA protocol and how it can best be implemented to achieve satisfactory outcomes.
Outcomes
Transition of TLIF procedures to the outpatient setting has been successful in a number of ways. Mean operative times for patients that underwent an outpatient TLIF was 110.7 minutes. Additionally, patients undergoing surgery in outpatient settings demonstrated statistically significant improvements from preoperative baseline in VAS back (p=0.005), VAS leg (p=0.001), ODI (p=<0.001), and PROMIS-PF (p=0.010) by the 6-month postoperative timepoint (Table 4).
One key to this success has been the avoidance, early recognition, and proper management of perioperative complications. Many complications unique to MIS TLIF reflect the need to work in a relatively small window bound by neural elements (Sclafani and Kim 2014; Lau et al. 2011; Wang and Zhou 2014). Implant malpositioning, for example, has been cited as one of the most common complications (Sclafani and Kim 2014). To help avoid this, fluoroscopy is used during patient positioning, incision planning, endplate preparation, and implant placement. All patients receive a final set of radiographs prior to discharge to ensure proper positioning. Unanticipated medical or anesthesia-related complications, such as atrial fibrillation, acute coronary syndromes, and postoperative nausea to name a few, are also possible. To combat these possibilities, in addition to having a synchronous relationship with experienced anesthesia colleagues, all our standalone ASC facilities are within 20 minutes of an affiliated hospital with intensive care unit capabilities. When perioperative complications do occur, a comprehensive review process is triggered between our surgical team, the anesthesia staff, and the ASC team. This enables all parties to recognize any shortcomings and opportunities for improvement.
Patients meet discharge criteria from the ASC once their pain is controlled, they are able to urinate, and they can ambulate safely. Early mobilization with our team of physical therapists helps to identify any patients that may benefit from extra time and effort. After discharge from the facility, all patients are scheduled for follow-up appointments with plain radiographs of the lumbar spine at 6-week, 12-week, 6-month, and 1-year timepoints to ensure that they are progressing appropriately in their postoperative course.
Conclusion
The MIS TLIF procedure is a highly effective treatment option for degenerative pathology of the lumbar spine, and its use is only expected to increase. The successful transition of this procedure to the outpatient setting is dependent on standardization of protocols to improve safety and efficiency. Key lessons can be learned from total joint arthroplasty, and other types of surgery with streamlined and uniform methods. Spine surgical teams can adopt these methods of standardization in their own routines to help expand their MIS TLIF outpatient practice.