


Introduction
Pain following orthopaedic surgical procedures remains undertreated due to inadequate analgesic options. Opioids have well-known limitations for both individuals and society. Single-injection local anesthetic-based peripheral nerve blocks have been used for decades to treat postoperative pain but have a duration of action of less than 24 hours. The analgesia may be prolonged with the use of liposomal bupivacaine or a perineural local anesthetic infusion (continuous peripheral nerve block), but these are similarly limited in duration to approximately 72 hours (Ilfeld 2017). For many orthopaedic procedures, the duration of pain is measured in weeks and not hours or days. One analgesic alternative—percutaneous peripheral nerve stimulation—can improve post-surgical analgesia while concurrently decreasing or obviating opioid requirements without any adverse systemic side effects (Ilfeld, Plunkett, Vijjeswarapu, et al. 2021). However, the only lead/electrode available to date cleared for treating acute pain within the United States (SPRINT, SPR Therapeutics, Cleveland, Ohio) was developed for chronic pain conditions and costs many thousands of dollars (Ilfeld and Finneran 2020). Therefore, while this device is being further investigated, it is not anticipated to gain widespread use clinically. In addition, this device does not provide the potent analgesia required by patients in the immediate postoperative period, and therefore a single-injection local anesthetic peripheral nerve block is added, requiring two separate procedures and associated equipment.
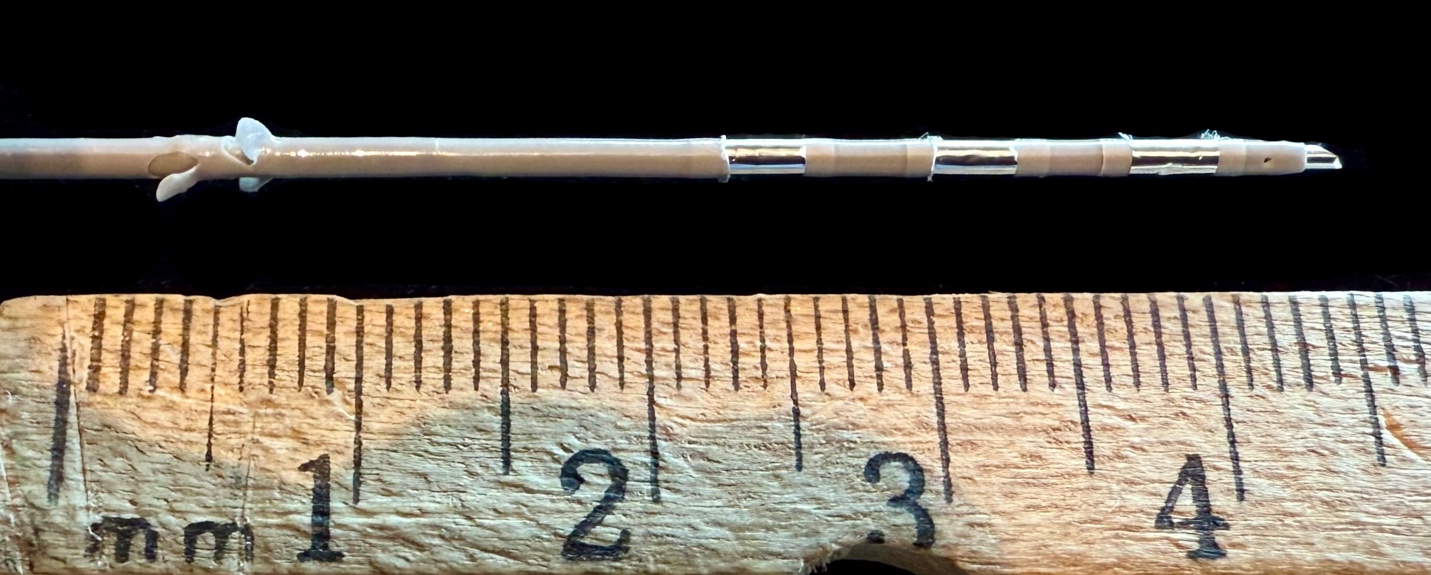
One possible solution is a novel device currently under investigation to treat postoperative pain. The RELAY system (Gate Science, Moultonborough, New Hampshire) is comprised of a basic catheter-over-needle device to allow ultrasound-guided percutaneous insertion, leaving a perineural catheter after simple withdrawal of the internal needle (Figure 1). A single-injection bolus of local anesthetic may be quickly administered. Following surgery, the catheter may be attached to a portable infusion pump to provide an ambulatory perineural local anesthetic infusion (continuous peripheral nerve block). Unlike previously described perineural catheters, the RELAY has an embedded wire and integrated pulse generator that permit stimulation of the targeted peripheral nerve(s) for up to 28 days. A smartphone application enables a Bluetooth connection with the pulse generator, allowing patients to titrate the stimulation intensity.
_is_comprised_of_a_basic_cat.jpeg)
The device therefore theoretically enables analgesia for multiple weeks with a single percutaneous procedure. This is potentially revolutionary because it would allow a healthcare provider to deliver (1) a single-injection peripheral nerve block; (2) a continuous peripheral nerve block; and (3) neuromodulation using a single device that can theoretically be placed in the same amount of time required for a single-injection peripheral nerve block. Instead of providing fewer than 24 hours of postoperative analgesia, up to 28 days of pain control could be delivered without disruption of existing practice patterns. We here provide the first description of this novel device when used to provide pain control following a reverse total shoulder arthroplasty procedure.
Case Report
The United States Food and Drug Administration approved the feasibility study protocol under an Investigational Device Exemption. Following prospective registration (NCT06818708) and approval by the local Institutional Review Board (University of California San Diego, La Jolla, CA), we enrolled an otherwise healthy 67-year-old woman undergoing unilateral (right), primary reverse total shoulder arthroplasty. Following written informed consent and in the supine position, the patient had standard intraoperative external monitors placed and oxygen delivered by facemask. The pulse generator was turned on by pressing a single button and connected via Bluetooth to a mobile device (iPhone 16, Apple Inc., Cupertino, CA) using a proprietary app (GateKeeper, Gate Science, Moultonborough, NH). The minimum and maximum currents were set to 0.2 mA and 10.0 mA, respectively. The catheter had 3 electrodes at the end, with the most distal programmed as the anode and the middle as the cathode with the proximal electrode inactive.
The right side of the neck was cleansed with chlorhexidine gluconate and isopropyl alcohol and covered with a sterile fenestrated drape. Intravenous sedation/analgesia with midazolam (1 mg) and fentanyl (50 μg) was administered for patient comfort as is standard for peripheral nerve block administration. The target nerve(s) were visualized using ultrasound with a linear transducer in a sterile sleeve. A transverse cross-sectional (short axis) view of the brachial plexus roots was observed and the transducer rotated approximately 90°, resulting in an oblique, cross-sectional view of the C5/C6 nerve roots with the transducer oriented roughly cephalad-caudad. A skin wheal of lidocaine was raised immediately superior to the transducer to anesthetize the skin and then the track towards the target roots.
Through the local anesthetic skin wheal, the device was advanced immediately posterior to the C5/C6 nerve roots (Figure 2) with small boluses of D5W (5 mL) via the integrated needle to open the potential space between the roots and surrounding fascia. The pulse generator was initiated at 0.2 mA and the current increased until the patient perceived a “pleasant massage” over her shoulder (2.2 mA). The internal needle was removed and lidocaine 2% with epinephrine (10 mL) injected via the remaining catheter. Accurate catheter tip placement was demonstrated with a decreased cutaneous sensation to cold temperature over the deltoid muscle. Bupivacaine 0.5% with epinephrine (10 mL) was subsequently injected to maximize the single-injection peripheral nerve block duration. The catheter was rotated counterclockwise to help anchor the device with small projections (“tines”) emanating from the catheter at approximately 4 cm from the distal end (Figure 3). The device was secured with wound closure adhesive (2-Octyl 2-cyanoacrylate) applied to the exit point, benzoin, a chlorohexidine-impregnated biopatch around the catheter entry point, and an overlying occlusive dressing (Figure 4). A ropivacaine 0.2% infusion was initiated with a portable infusion pump (ambIT, Avanos Medical, Alpharetta, GA) via the catheter (8 mL/h basal infusion, 4 mL bolus dose, 30 min lockout period, 500 mL reservoir). Her pulse generator was turned off.
_being_inserted_under_ultras.jpeg)

_seen_following_insertion_ad.jpeg)
The patient underwent an uncomplicated surgical procedure under a general anesthetic of inhaled anesthetic combined with nitrous oxide.
Within the recovery room, the patient reported no surgical pain and her pulse stimulator turned back on with a current of 2.2 mA. We chose the lowest current level perceived by the patient during insertion to avoid over stimulation. With the local anesthetic peripheral nerve block, patients can tolerate very high electrical currents; but when the local anesthetic effects resolve, the current can be too high and induce pain. This is a confusing situation for patients because they do not know if the pain they are experiencing is due to a current that is too high—in which case the solution is to decrease the current—or is due to surgical pain, in which case the solution is to increase the current. Therefore, we start patients at a very low current (perceived threshold) and have them increase when their peripheral nerve block begins to resolve and their surgical pain increases. The patient was discharged home with verbal and written instructions as well as additional occlusive dressings to redress the device, if desired. She downloaded the controlling application to her own phone and was taught how to connect to the pulse generator and adjust the current level.
When queried the day after surgery, the patient’s initial single-injection nerve block resolved earlier that morning and she experienced a maximum pain score measured on the 0-10 Numeric Rating Scale (NRS) of 3, and an average NRS of 1. The patient’s NRS was 0-1 for the remainder of her perineural local anesthetic infusion. The pump/tubing was disconnected the morning of postoperative day (POD) 3 by an investigator, after which neuromodulation was the exclusive analgesic necessary with maximum and average pain scores of 0.5 and 0 on POD 4, respectively. The catheter/lead was removed by the participant’s caregiver on POD 7 with instructions provided by telephone by an investigator: the occlusive dressing was removed and gentle traction applied to the pulse generator while rotating the catheter clockwise. The disposable pulse generator/catheter were discarded in the trash. The patient was contacted on POD 8 and reported no pain following POD 4. No opioids were required following surgery.
Conclusions
This case report illustrates the feasibility of using a novel device that, with a single ultrasound-guided insertion, enables the delivery of a single-injection peripheral nerve block, a subsequent multi-day perineural local anesthetic infusion, and up to 28 days of peripheral nerve stimulation. It is applicable to any peripheral nerve and most surgical procedures of the extremities. Unlike local anesthetic, electrical current induces no sensory, motor, or proprioception block; and, therefore, may be used in the lower extremities without inducting weakness and increasing the risk of falling. Multiple devices could be used for bilateral surgery or unilateral procedures in which blockade of multiple peripheral nerves is desired. Considering the significant unmet need for nonopioid postoperative analgesic options, further investigation of this new device appears warranted.