Introduction
Attendance at follow-up visits decreases the rate of complications and readmission after operative injuries (Saunders, Fernandes-Taylor, Rathouz, et al. 2014; Tevis et al. 2014; Watts, Kehoe, and Luesley 1997). Risk factors for decreased follow-up include homelessness, increased distance from the clinic site, drug/tobacco use, and lack of private insurance (Whiting, Greenberg, Thakore, et al. 2015; Agel et al. 2021). Insurance status can significantly impact access to and quality of healthcare, with insured individuals experiencing better health outcomes across a range of services (Institute of Medicine (US) Committee on the Consequences of Uninsurance 2002). This trend is also seen among trauma patients, where uninsured status and minority race are associated with higher in-hospital mortality and decreased post-hospital care in patients with severe injuries (Gerry et al. 2016). Another factor that affects patient outcomes is follow-up adherence, which is a known challenge in orthopedic trauma as providers are unable to modify treatment regimens and cannot detect potential complications (Zelle et al. 2015).
Studies have suggested that insurance status, male sex, and tobacco and illicit drug use significantly affect the six-month follow-up of orthopedic trauma patients (Whiting, Greenberg, Thakore, et al. 2015; Zelle et al. 2015; Bhashyam et al. 2023; Bliss, Mora, and Krause 2016; Launonen, Sumrein, Reito, et al. 2019; Zubovic et al. 2021). For example, one study that assessed adult patients with acute hand injuries at a private institution found that uninsured and Medicaid-insured patients were less likely to initiate outpatient follow-up or complete recommended follow-up than privately insured patients (Zubovic et al. 2021).
Previous studies on this topic used data from patients at private academic centers, where insurance status likely plays a larger role in accessing follow-up care than at public hospitals (Whiting, Greenberg, Thakore, et al. 2015; Zelle et al. 2015; Bhashyam et al. 2023; Zubovic et al. 2021; Rucinski et al. 2023). Studies that specifically analyze the role of insurance status on the rate of orthopedic trauma follow-up at public institutions remain limited. Additionally, most of the existing studies analyzed orthopedic trauma patients who underwent surgical management for their injuries during their initial presentation/admission. To our knowledge, there are currently no studies that evaluate the impact of insurance status on the initiation and completion of follow-up of orthopedic trauma patients with non-surgically managed injuries. Our study addresses these literature gaps by exploring the following questions: (1) At a public hospital where access to medical care should not be limited by insurance status, does insurance status still have an impact on the follow-up of orthopedic trauma patients? (2) How does follow-up adherence differ between surgically and non-surgically managed orthopedic trauma patients?
Materials & Methods
Institutional Review Board (IRB) approval was obtained. We conducted a retrospective chart review of 1040 patients who presented to the emergency department or level-one trauma center at a tertiary care hospital in the United States for an injury that required an orthopedic surgery consultation over a 13-month period (January 1, 2021, to January 31, 2022). All adult patients (age 18+) evaluated by the orthopedic surgery team were included, whether they had an isolated orthopedic injury or not. Additionally, both operative and non-operative orthopedic trauma patients were included. Patients younger than 18, patients who died during their hospital stay or soon after discharge, and patients who were incarcerated at the time of injury were excluded.
All data that was used in this analysis were extracted from electronic medical records. The following variables were collected: age, sex, race/ethnicity, primary language, employment status, tobacco use, alcohol use, mechanism of injury, diagnosis, admission status, operative status, insurance status, and type of insurance. Type of insurance was categorized as Private, Medicare, Medicaid, Workers’ Compensation, no insurance, or a Hospital Card (local financial assistance program); these insurance types were then grouped into either “insured” or “uninsured” categories. The “insured” group included patients with Private, Medicare, Medicaid, or Workers’ Compensation insurance, while the “uninsured” group included patients with no insurance or a Hospital Card. Patients with any form of Medicaid, including traditional Medicaid plans and HMO-like plans, were all grouped into one Medicaid category. Patients with a Hospital Card are described as “uninsured-assisted,” whereas patients with no form of insurance or financial assistance are described as “uninsured-unassisted.”
The recommended time to follow up and adherence with follow-up were extracted from the chart review. Follow-up was defined as the patient presenting for the first scheduled clinic appointment or outpatient operation, whichever came first. Patients who attended their first follow-up visit were further stratified to determine the status of follow-up at six months (Zelle et al. 2015). These patients were categorized as completed follow-up (no further follow-up necessary, follow-up as needed, or ongoing follow-up at six months) or lost to follow-up (failure to return as recommended).
Patients were also divided into “COVID” and “post-COVID” groups. The “COVID” group included patients who presented on or before May 31, 2021, and the “post-COVID” group included patients who presented on or after June 1, 2021. These dates were selected because the study institution’s COVID-19 restrictions were completely lifted by the end of May 2021. Follow-up at first appointment and at six months were compared between these groups to assess for confounding effects of COVID-19 restrictions.
The primary outcome of this study was to determine the impact of insurance status on the follow-up of orthopedic trauma patients after discharge.
Statistical Analysis
Demographic data representing our sample were analyzed using descriptive statistics with frequency counts reported for each variable. Subsequently, significant associations with the two dichotomous outcome variables (attended first appointment and follow-up at six months) and other categorical variables were identified using a Chi-Squared test for independence. Pairwise comparisons were done, and all p-values are reported using the Bonferroni adjustment with the significance level set at p=0.05. Selected variables were entered into a logistic regression for analysis of the outcome variables Attended First Appointment and Follow-Up Status at Six Months. All analysis was performed using SPSS Version 28 (IBM, Armonk NY).
Results
1040 patient charts were included for review. In this cohort, 201 patients were not recommended to follow up in the health system of interest and were subsequently excluded from the analysis. Of the 839 patients recommended to follow up, 59.5% were insured while 40.5% were uninsured. On average, the recommended time to follow up after discharge was 1-2 weeks. Additional detailed demographic information is displayed in Table 1).
The most common mechanism of injury was a fall from standing (height <6 feet), and the most frequently injured anatomic location was the upper extremity. A detailed description of the mechanism of injury and anatomic location of injury is shown in Table 2).
There were 262 patients in the “COVID” group, of which 157 (59.9%) were insured and 105 (40.1%) were uninsured, and 577 patients in the “post-COVID” group, of which 343 (59.4%) were insured and 234 (40.6%) were uninsured. Additional information regarding the breakdown of the “COVID” and “post-COVID” groups are in Table 3).
Attended First Appointment
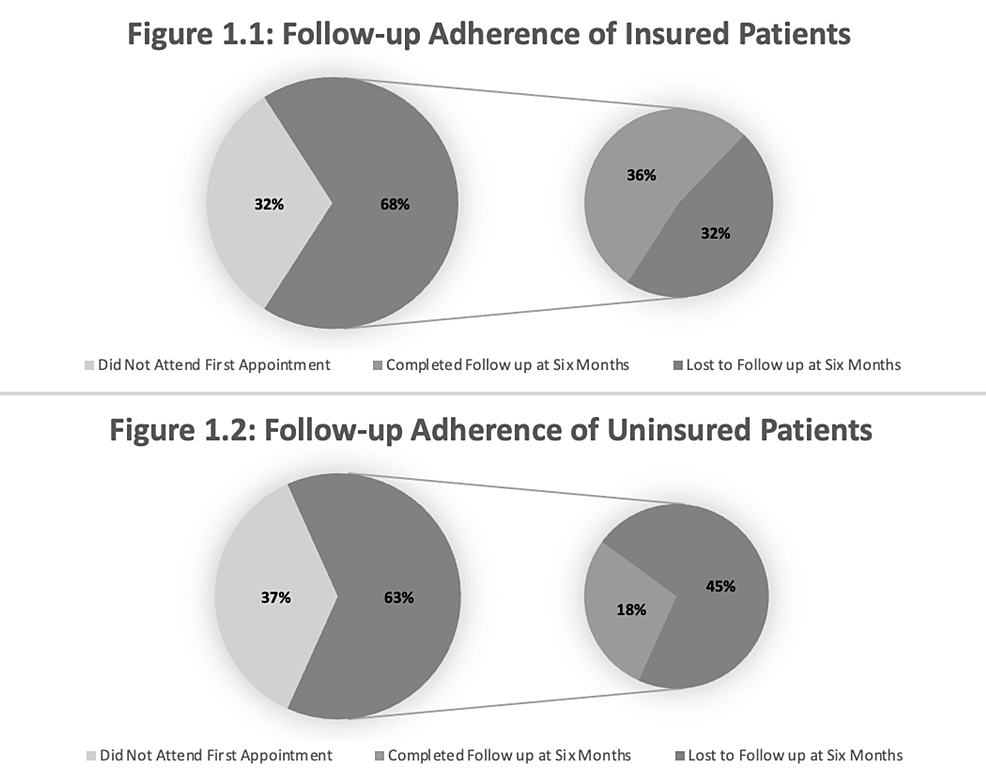
There were 839 patients recommended for follow-up. 556 (66.3%) patients attended their first follow-up appointment, of which 341 (61.3%) were insured and 215 (38.7%) were uninsured. 283 (33.7%) patients did not attend their first follow-up appointment, of which 159 (56.2%) were insured and 124 (43.8%) were uninsured. There was no significant association between insurance status and attendance at first appointment (p=0.111) (Figure 1).

Figure 1 depicts the follow-up rates of insured and uninsured patients. Figure 1.1 shows that 32% of insured patients did not attend their first follow-up appointment, and 68% of insured patients did attend their first appointment; of this 68%, 36% completed the recommended follow-up and 32% were lost to follow-up. Figure 1.2 shows that 37% of uninsured patients did not attend their first follow-up appointment, but 63% did, of which 18% completed recommended follow-up and 45% were lost to follow-up.
A total of 165 patients (63.0%) in the “COVID” group attended their first follow-up appointment, of which 106 (64.2%) were insured and 59 (35.8%) were uninsured. A total of 391 patients (67.8%) in the “post-COVID” group attended their first follow-up appointment; 235 (60.1%) were insured and 156 (39.9%) were uninsured (Table 3). There were no significant differences between COVID groups for patients who attended their first follow-up appointment.
Only 52.8% of current smokers attended their first follow-up appointment compared to 70.6% of never-smokers, which demonstrated a significant association between tobacco use and attendance at first follow-up appointment (p<0.001). Alcohol use was also significantly associated with attending the first appointment - only 61.0% of patients who reported using alcohol attended while 69.6% of patient who denied alcohol use attended (p=0.044).
269 patients presenting with orthopedic trauma injuries were taken to the operating room at their initial encounter. 81.4% of operatively managed patients attended their first follow-up appointment, while only 59.1% of non-operatively managed patients attended their first follow-up appointment (p<0.001). There was also a significant association between ethnicity and attendance at first follow-up appointment (p=0.048). Detailed information about patient follow-up is displayed in Table 4).
Insurance status did not contribute (p=0.185) to the logistic regression model. Of the variables entered, current smoker (p=0.005), speaking Haitian Creole (p=0.028), speaking Spanish (p=0.025), operative management (p<0.001), and age (p<0.029) significantly contributed to the model.
Follow-up at Six Months
Of the 556 patients who attended their first follow-up appointment, 242 (43.5%) completed the recommended follow-up at six months, 181 (74.8%) of whom were insured and 61 (25.2%) of whom were uninsured. There were 314 (56.5%) patients who attended their first follow-up appointment and were then lost to follow-up; 160 (51.0%) of these patients were insured and 154 (49.0%) were uninsured. This demonstrated that significantly more uninsured patients (71.6%) were lost to follow-up at six months than insured patients (46.9%) (p<0.001) (Figure 1).
Insurance category was significantly associated with follow-up status at six months (p<0.001). A pairwise comparison of categories demonstrated that significantly more uninsured-unassisted patients (73.2%) were lost to follow-up than privately insured patients (45.7%) (p<0.001). However, there was no significant difference between uninsured-assisted patients (64.3%) and privately insured patients (45.7%) who were lost to follow-up (p>0.05).
78 patients (47.3%) in the “COVID” group who attended their first appointment completed follow-up at six months, of which 59 (75.6%) were insured and 19 (24.4%) were uninsured. 164 patients (41.9%) in the “post-COVID” group who attended their first appointment completed follow-up at six months, of which 122 (74.4%) were insured and 156 (39.9%) were uninsured (Table 4). There were no significant differences between COVID groups for patients who had completed follow-up at six months.
Tobacco use, alcohol use, and operative versus nonoperative management of injuries was not associated with completion of follow-up at six months. However, there was a significant association between ethnicity and completion of follow-up at six months (p=0.041).
Insurance status did significantly contribute (p<0.001) to the logistic regression model increasing the chance of a patient to have completed follow-up at six months. Black/African American race (p=0.002) was the only other predictor that contributed to the regression, decreasing the chance of a patient to have completed follow-up at six months.
Discussion
Follow-up nonadherence is a widespread problem in orthopedic trauma. Many orthopedic trauma injuries are debilitating and require significant rehabilitation and close follow-up to prevent permanent functional limitation (Luthi et al. 2015). Despite the known importance of outpatient follow-up, Agel et al. found that the follow-up rate was only 29% at the one-year mark for patients who sustained orthopedic trauma injuries (Agel et al. 2021). Previous literature has reported a correlation between insurance status and long-term follow-up in orthopedic trauma patients. For example, Bhashyam et al. studied orthopedic trauma follow-up after surgical intervention and found a significant decrease in follow-up, particularly in patients with Medicaid insurance (Bhashyam et al. 2023). Whiting et al. found that a lack of private insurance led to decreased attendance at the first follow-up visit after orthopedic trauma surgery at a level-one trauma center (Whiting, Greenberg, Thakore, et al. 2015).
In our study, 59.5% of patients who were evaluated by the orthopedic trauma team and recommended for follow-up had health insurance and 40.5% had no form of health insurance. Interestingly, a needs assessment conducted at the time of this study found that 89.5% of adults in the same county as the study institution had health insurance, while the remaining 10.5% were uninsured (“Adults with Health Insurance” 2023). The discrepancy in insurance coverage types between our randomized sample and the general population may emphasize the importance of public hospitals, which offer high-quality healthcare access to uninsured patients who might otherwise go without it.
First follow-up appointment
Our analysis showed that 66.3% of patients presented for their first follow-up appointment, with no significant difference between the insured and uninsured cohorts (68.2% v 63.4%, respectively) (p =0.111). The non-significance of follow-up adherence at the first visit between these groups emphasizes the importance of public hospitals for promoting health equity. These results are further supported by current literature. For example, Whiting et al. reported a 66.9% attendance rate at the first scheduled post-operative clinic visit (Whiting, Greenberg, Thakore, et al. 2015).
Rosenbaum et al. reported a 23% loss to follow-up rate in orthopedic patients requiring short-term follow-up after hand or upper extremity surgery, and a 44% nonadherence rate in only the “self-pay” or uninsured cohort (Rosenbaum et al. 2019). Here, we found a similar (44.3%) rate of nonadherence within the uninsured cohort at the first follow-up visit. Neither our study nor Rosenbaum et al. found a difference between follow-up in the uninsured versus insured analysis. These similar findings could be explained by the fact that both studies were completed at a public government-funded hospital, which further supports the idea of public hospitals functioning as a driver for health equity in the initial injury period.
Insurance status did not influence whether a patient was managed operatively or nonoperatively, though operatively treated patients had a significantly higher rate of adherence at first follow-up appointment than those treated non-operatively. This finding is supported by previous studies that have demonstrated the importance of close follow-up after invasive interventions (Dahlberg et al. 2018; Kirchner et al. 2022). This association of insurance status and operative follow-up is vital when planning treatment, and strategies for increasing orthopedic follow-up within this cohort could place emphasis on education and accessibility (Zelle et al. 2015; Bhashyam et al. 2023; Medford-Davis et al. 2017).
Alcohol and smoking were additional characteristics associated with significant results in follow-up adherence within our study. Patients reporting tobacco usage attended first follow-up visits at a rate of 52.8%, significantly lower than the rate in the cohort reporting no tobacco usage (70.6%) (p<0.001). Patients reporting any amount of alcohol use similarly attended the first follow-up visit at a lower rate when compared to patients with no reported alcohol usage (61.0% v 69.6%, respectively) (p=0.044). Within orthopedics, studies have reported correlations between lack of follow-up care and smoking, drug use, and other substance use (Whiting, Greenberg, Thakore, et al. 2015; Agel et al. 2021). One explanation for these findings is that alcohol and tobacco use are commonly associated with lack of social support, increased financial needs, and generally a lower socioeconomic status, all of which are barriers to care (Whiting, Greenberg, Thakore, et al. 2015; Cerdá, Johnson-Lawrence, and Galea 2011; Collins 2016; Lowry et al. 1996). This population may require early involvement of social workers or substance-use counselors, along with clear post-operative care instructions to enhance follow-up adherence.
Prior studies have also suggested that lower education levels correlate with decreased follow-up adherence at the first appointment. A retrospective review of metacarpal fracture patients found that not being a college graduate was associated with non-attendance at the first follow-up visit (p = .025); however, multivariable analysis did not confirm it as an independent predictor (ten Berg and Ring 2012). Similarly, a study on distal radius fractures identified that a lack of post-secondary education was associated with loss to follow-up (Tejwani et al. 2010).
Geographic distance also presents a significant barrier to first follow-up appointment. In the Whiting et al. retrospective study from a separate level 1 trauma center, patients living more than 100 miles from the clinic were significantly more likely to miss their first follow-up appointment (Whiting, Greenberg, Thakore, et al. 2015). While prior research has examined the role of distance, few studies have specifically evaluated access to public transportation and its impact on orthopedic trauma follow-up adherence. This remains an important avenue for future research, particularly in urban and underserved populations.
While this study’s main focus was not these social drivers of health, all likely contributed to the disparities in follow-up care. These social determinants are closely linked to insurance status and could further explain differences in adherence patterns observed in this study.
Lastly, many hospital systems employ patient navigators or case managers to provide reminders, assist with scheduling, and offer patient education, while social work and financial assistance programs help address underlying socioeconomic barriers. However, there is limited research on the effectiveness of these initiatives on follow-up in orthopedics. Future studies should assess their impact on improving follow-up adherence among high-risk orthopedic trauma patients.
Six-month follow-up
Long-term follow-up is also critical for orthopedic trauma patients (Zelle et al. 2015). Unfortunately, orthopedic trauma generally has poor long-term follow-up rates (Agel et al. 2021). Multiple factors have been correlated with poor follow-up in this population, including lack of health insurance (Agel et al. 2021; Zelle et al. 2015).
In our study, 56.5% of patients were lost to follow-up and 43.5% completed follow-up at six months. Within the cohort who attended their first follow-up visit but were then lost to follow-up, there was no significant difference in rates between insured versus uninsured patients. Overall though, including patients who failed to attend the first follow-up visit, 71.6% of patients who were lost to follow-up were uninsured, significantly different from the insured cohort (p<0.001) (Figure 1). With this, we can infer that uninsured patients have a significantly higher risk of being lost to follow-up at six-months.
The significantly lower rate of follow-up reported in uninsured populations has been previously studied (Whiting, Greenberg, Thakore, et al. 2015; Bhashyam et al. 2023; Bliss, Mora, and Krause 2016). Patients with access to health insurance may be less financially burdened by medical bills, possibly due to better follow-up coverage included in their health insurance plans. On the other hand, debt and lower socioeconomic status places financial and emotional burdens on patients that can interfere with their ability to complete follow-up.
Within the uninsured cohort in our study, the uninsured-unassisted were lost to follow-up significantly more than patients with a Hospital Card (uninsured-assisted). Additionally, there was no difference in the follow-up at six months between privately insured patients and uninsured-assisted patients. This insignificance emphasizes and reassures the critical role that financial assistance programs play in providing equitable access to healthcare from an orthopedic trauma perspective. Without such financial assistance, patients would fall into the uninsured-unassisted cohort which, once again, carries a significantly lower rate of follow-up when compared to patients with some form of health insurance or financial assistance.
COVID-19
This study was performed using data between 2021 and 2022, during part of the COVID-19 pandemic. Pandemic-related factors posed several challenges to healthcare delivery including postponement of elective procedures and limitations on clinic visits.
In our study, there was no significant difference in attendance at first follow-up appointment and follow-up status at six months between the “COVID” and “post-COVID” groups. This finding was consistent across all insurance types, including uninsured-assisted and uninsured-unassisted groups, which suggests that the COVID-19 pandemic did not confound our results regarding the impact of insurance status and follow-up.
Our results are generally inconsistent with the observations made in other studies regarding follow-up during the COVID-19 pandemic (Subathra et al. 2021; Danhieux, Buffel, Pairon, et al. 2020; De Vincentis, Domenici, Ansaloni, et al. 2022; Aragona et al. 2020). There are a few explanations for this disparity. Our study specifically focuses on patients with traumatic mechanisms of injury, whereas a majority of the literature on this topic focuses on less acute and more elective diseases. Additionally, this study was conducted in a state and city that had more skeptical perceptions of COVID-19 and pandemic-related restrictions, especially once the peaks of disease and death burden passed.
Limitations
As is the nature of a large retrospective study, follow-up is determined based on data made accessible by the electronic medical record (EMR). In our study, an additional EMR from an affiliated hospital system was checked for each patient. However, unreported follow-up at different institutions or out of state is possible. Additionally, insurance status at the time of the injury and at the time of follow-up was inferred to be the same, which may not be accurate. Loss of insurance between hospital discharge and scheduled follow-up could be a significant barrier to care and should be evaluated in future research.
The long-term follow-up time frame of six months was based on previous similar studies (Zelle et al. 2015). Follow-up rates beyond this time frame cannot be inferred and could show different results. Additionally, we grouped all Medicaid patients into one category, though it is possible that the various Medicaid plans have different reimbursement structures that can impact patient ability to follow up.
Additionally, follow-up rates may also be influenced by the employment structure of providers. At the Level 1 trauma center where this research took place, all patients—regardless of insurance status—are scheduled for outpatient follow-up at an affiliated public clinic that provides care for both insured and uninsured individuals. However, orthopedic trauma surgeons affiliated with private practices may have different follow-up processes compared to those employed by hospital systems, which could impact the generalizability of our results.
Furthermore, patients categorized as operatively managed underwent surgery during their inpatient admission. However, a small number of patients initially managed non-operatively were advised to return for further surgical evaluation and eventually out-patient surgery. This distinction may have influenced follow-up adherence, as patients who were initially told that surgery was not immediately necessary may have been less motivated to return for further evaluation.
Lastly, another important aspect of follow-up adherence is rehabilitation. While this study focused on follow-up attendance, it did not track referrals for physical therapy, which is critical for functional recovery in many orthopedic trauma patients. Future studies should evaluate PT referral adherence and its impact on long-term functional outcomes. Ensuring that patients follow through with PT may be just as important as attending follow-up appointments in determining overall recovery success.
Conclusions
This study suggests that insurance status did not significantly impact the attendance of orthopedic trauma patients at their first follow-up appointment at a public hospital, but non-operative treatment and alcohol and tobacco usage did. Additionally, patients enrolled in the hospital’s local financial assistance program (Hospital Card) were lost to follow-up significantly less than patients with no form of insurance or financial assistance, and these Hospital Card patients did not have a significantly different rate of follow-up at six-months when compared to privately insured patients. These findings highlight the role of financial assistance programs in improving follow-up adherence for otherwise uninsured orthopedic trauma patients.
Disclosures
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. University of Miami issued approval 20220797. The IRB approved a Waiver of Consent. The IRB approved a full Waiver of Authorization for this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue.