
Level of Evidence: IV
What is already known:
-
Musculoskeletal strain and injury occur in orthopaedic surgeons, related to case volume and practice duration
-
Musculoskeletal strain and injury has been reported as high as 44% in orthopaedic surgeons, with 10% of 140 polled orthopaedic surgeons in one study missing up to 3 weeks of work due to strain
-
Lateral decubitus positioning has traditionally been described as more comfortable for the surgeon, based on expert opinion only
Why this needed to be done:
- There may be many modifiable, identifiable risk factors for musculoskeletal strain for orthopaedic surgeons performing shoulder arthroscopy regularly
What are the new findings:
-
Identifiable risk factors for musculoskeletal strain include patient height, monitor position and working distance from the surgical field (including arthroscopic instrument length)
-
Lateral decubitus patient positioning identified more at-risk working positions for musculoskeletal strain than beach chair
-
Observational functional assessments can be used in orthopaedic surgery to determine and potentially mitigate risk factors for at work musculoskeletal strain and injury
INTRODUCTION:
Occupational injury and work-related musculoskeletal symptoms (WMS) in the general population are estimated to cost over $190 billion annually in the United States, with combined effect of direct cost and productivity loss (Davis et al. 2013; Szeto et al. 2009). Ergonomics was formally defined in 1949 to better characterize the anatomy, physiology, psychology and engineering systems approach to work-place health and productivity (Supe, Kulkarni, and Supe 2010). Despite consensus statements and work-place health and safety recommendations, WMS has a high prevalence in the health-care field, and specifically to surgeons (Hallbeck et al. 2017; Hegmann et al. 2016; Linaker and Walker-Bone 2015; Papaspyros, Kar, and O’Regan 2015; Stucky et al. 2018). Reports of WMS for surgeons in multiple disciplines is as high as 68% for combined, general musculoskeletal pain (Stucky et al. 2018). Site-specific WMS has been characterized in surgical disciplines of plastic surgery, general surgery and surgical endoscopy, vascular surgery, neurosurgery, cardiovascular surgery, and otolaryngology to greater degrees than orthopaedic surgery (Capone et al. 2010; Stucky et al. 2018; Supe, Kulkarni, and Supe 2010). Sites of injury include eye strain, neck, back, arm/shoulder, hand and wrist, and leg pain (Stucky et al. 2018). It has been shown that surgeons performing minimally invasive or endoscopic surgery have a higher risk of generalized, and site specific pain (Stucky et al. 2018). During endoscopic surgery, there is decoupling of the visual and motor axes with loss of direct tactile feedback, resulting in greater difficulty of tissue manipulation and dexterity. This, combined with the lack of depth perception and peripheral vision cues predisposes to static positioning, or highly specific repetitive motions (Supe, Kulkarni, and Supe 2010).
WMS in orthopaedic surgeons is as high as 44% (Davis et al. 2013). A survey of 140 orthopaedic surgeons across varied subspecialties demonstrated a correlation of injury to duration of practice. Of respondents, 10% had missed work, up to periods of 3 weeks duration (Davis et al. 2013). The short- and long-term economic implications have not been characterized for orthopaedic surgeons suffering WMS but can be inferred. Shoulder surgeons can perform arthroscopic procedures with patients positioned in the lateral decubitus, or beach-chair position. The benefits of each position have been previously characterized for indications such as instability surgery or rotator cuff repair (Hamamoto et al. 2017; Li et al. 2015; Peruto, Ciccotti, and Cohen 2009). The lateral decubitus position requires axial traction of the operative arm, and with this positioning has been described as providing decreased potential for fatigue and greater surgeon comfort. This is based on level V evidence, with no ergonomic analysis previously performed (Hamamoto et al. 2017; Lajtai G, Aitzetmüller G. 2017).
Our study aims to characterize ergonomic factors of arthroscopic shoulder surgery in both beach-chair and lateral decubitus positioning. By providing risk factors for WMS and potential solutions in this pilot study, we hope to better inform shoulder surgeons of longitudinal safe practices and stimulate further research. Secondarily, we will characterize differences in WMS risk factors and ergonomics between beach-chair and lateral decubitus positioning that challenges the current recommendations.
METHODS:
Study Design
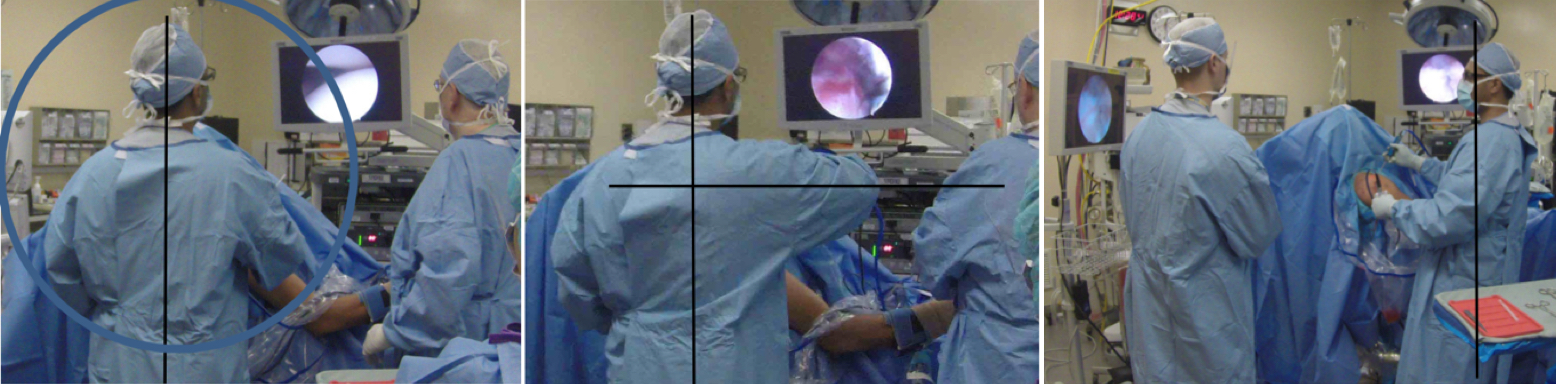
An observational pilot study of surgeon ergonomics during arthroscopic shoulder surgery was performed. Video recordings and photographs of surgeons during arthroscopic shoulder surgery in both beach-chair and lateral decubitus patient positioning were produced and analyzed by an occupational therapist (OT) specializing in occupational functional assessments. The focus of the media assessments was surgeon positioning in relation to the surgical operative site, namely the acromioclavicular joint, and repetitive motioning. The occupational therapist was tasked with providing risk factors for musculoskeletal strain or injury and potential solutions in a site/body segment specific manner. Mechanical risk factors of strain including force of activity, vibration, and contact stress were not analyzed due to limitations of the surgical field. Data collected included surgeon demographics, operative duration, average surgeon elbow working height (measured from the ground), height of the acromioclavicular joint (measured from the ground), and surgeon body part positioning relative to the patient and arthroscopic monitor including head and neck, shoulder, upper extremity, back, and lower extremities.
Participants
Three arthroscopic procedures were included for analysis, two in beach-chair positioning and one in lateral decubitus position. Two procedures involved arthroscopic subacromial decompression with rotator cuff repair, and one involved subacromial decompression alone. Two surgeons were used for the study, one predominantly performing arthroscopic shoulder procedures in the beach-chair position (surgeon A), and one predominantly performing arthroscopic shoulder procedures in the lateral decubitus position (surgeon B). Both surgeons are fellowship trained in advanced arthroscopic techniques and perform in a high-volume academic center. All procedures were performed on patient’s right shoulders for comparison.
Statistical Analysis
Qualitative analyses are provided of surgeon positioning and ergonomics given the small sampling size. Descriptive statistics were not produced given the small sample size.
RESULTS:
Beach-Chair positioning Risk Factors
Surgeon A completed two procedures in the beach-chair position. Standard patient preparation and draping with positioning adjuncts of beach chair table (Smith & Nephew, T-Max Shoulder Positioner) and Spider Limb Positioner (Smith & Nephew) for arm control were employed for both procedures. In a relaxed position, standing erect, surgeon A had a measured elbow height of 116.8 cm. Surgeon A is right-hand dominant and weighs approximately 82kg.
The first case duration was approximately 60 minutes. During the first case, the acromioclavicular height was kept at 129.5 cm, and above surgeon waist level to the mid-abdomen. Video analysis demonstrated sustained neck extension due to monitor positioning and when using longer instruments causing the surgeon to lean back at the torso, remaining static in the lower extremity. Repetitive shoulder abduction to 90 degrees was seen for 15 – 90 second intervals. Arthroscopic instrument length and surgeon positioning in proximity to the patient were seen as risk factors for increased shoulder abduction. Arthroscopic shaver and electrocautery use for tissue debridement were noted to provide repetitive forearm movement in extremes of radial and ulnar deviation during prono-supination arcs. Static positioning was noted of the lower extremities as well as distance of surgeon to the patient.
The second case duration was approximately 60 minutes. The acromioclavicular height was largely maintained at the surgeon’s waist level, or 116.8 cm from the ground. The monitor height was noted to be lower during this case resulting in less repetitive and sustained neck extension, though neck extension was noted to occur occasionally. The monitors were noted to be to the sides of the surgeon’s mid sagittal plane, causing neck rotation greater than 30 degrees for sustained periods with concomitant lateral flexion. The surgeon additionally utilized a second screen and rotated his torso to be in line with the monitor, eliminating the rotation and lateral flexion. When the surgeon was oriented more anterior or posterior of the patient’s shoulder performing the repair, surgeon shoulder positioning was noted to frequently be below 45 degrees, increasing to 60 to 90 degrees when the surgeon was working directly lateral with the same instruments. Twisting movements of the lower back were noted when the surgeon attempted to reach for instruments despite having a surgical assist and nurse present, both of which were able to visualize the monitors. The surgeon was noted to perform repetitive rotational forearm activities in end-range radial and ulnar deviation of the wrist, as well as static lower extremity positioning as during the first case.
Beach-Chair positioning Solutions
Potential solutions to muscular strain positioning or patterns of the surgeon were provided by the OT. Lowering the height of the monitor, and producing more dynamic involvement of the lower extremities including stances or turning to be perpendicular to the arthroscope screen would reduce neck extension, lateral flexion, or rotation, both static or dynamic. Appropriate positioning of the surgeon regarding distance to the operative field could additionally be optimized to prevent leaning of the torso, or excessive reach and shoulder abduction. Given the varying lengths of the instruments, dynamic positioning in this manner could potentially reduce abduction of the shoulders. Lowering of the operative field, in this case the acromioclavicular height to or below the working level of the surgeon’s elbows or waist could additionally reduce repetitive, prolonged, or excessive shoulder abduction. The repetitive wrist motions are required due to the finite nature of the soft tissue work, however, focus on providing more proximal muscle control and using the upper arms could prevent repetitive strain about the wrists or hands. Given the frequent periods of standing, appropriate shoe wear or padded steps were recommended to prevent lower limb and lower back strain. A list of identified risk factors and solutions to prevent strain for the beach-chair patient positioning are provided in Table 1.
Lateral Decubitus positioning
Surgeon B completed one procedure, identified as a subacromial decompression plus rotator cuff repair with patient in the lateral decubitus position. Standard patient positioning using a bean-bag positioner with arm holder in abduction (Arthrex) was utilized. The case duration was approximately one hour and ten minutes. In a relaxed position, standing erect, surgeon B had a measured elbow height of 118.1 cm. Surgeon B was additionally right-hand dominant and weighed 68kg.
During the case, surgeon B kept the acromioclavicular height from the ground at approximately the measured elbow height, or waist level, of 118.1 cm. Video analysis of surgeon B demonstrated appropriate at or below eye level screen positioning, however rotation of the neck greater than 30 degrees occurred when surgeon B was working through the anterior portals to see the screen. Additionally, this reaching motion caused trunk rotation with forward flexion for periods up to three minutes. Shoulder positioning demonstrated abduction periods beyond 60 degrees for up to three minutes at a time when the surgeon was working through the anterior shoulder portals. Further reaching in these positions was affected by the length of the arthroscopic equipment used. In addition to shoulder abduction, composite motions of flexion, abduction and internal rotation of the shoulders or combined with scapular elevation and elevation of the shoulders/trapezius was demonstrated for periods up to three minutes in duration. As seen with surgeon A, repetitive end-range radial and ulnar deviation of the wrist was demonstrated, as was full prono-supination arcs throughout the case. Surgeon B however demonstrated these forearm and wrist motions combined with reaching over the patient to work through the anterior portals. There was consistent static lower extremity positioning throughout the case.
Lateral Decubitus Solutions
Review of the video of surgeon B provided potential solutions to muscular strain risk factors demonstrated. Repositioning the monitor during portions of the case could be employed to reduce neck or trunk rotation. Changing position to be in closer proximity to the surgical field, or the surgeon standing at the patient’s head more frequently could reduce shoulder abduction, flexion and internal rotation, as well as scapular elevation. Additionally, lowering the patient further could reduce scapular elevation required to work through portals, or in reaching. Forearm and wrist range of motion was identified as necessary given the finite nature of the work, however could be mitigated with additional involvement of proximal arm movements. Anti-fatigue matting and appropriate footwear could be employed to reduce lower extremity or lower back strain with prolonged standing. Table 2 demonstrates risk factors for WMS and solutions for patient positioning in the lateral decubitus position.
DISCUSSION:
Utilization of arthroscopic technology has changed the way orthopaedic surgeons interact with patients in an operating room. To date, there have been numerous studies of surgeon ergonomics and risk factors for injury in general surgery/endoscopic surgery, plastic surgery, obstetrics and gynecology, urology, and neurosurgery, however none in orthopaedic surgery, and specifically shoulder arthroscopy (Soueid et al. 2010; Stucky et al. 2018). Arthroscopic shoulder surgery typically requires multiple portals around the anterior, lateral, and posterior aspects of the acromion and glenohumeral joints, requiring surgeons to perform necessary measurable surgical actions in a number of planes about the surgical field. The effect of patient positioning in surgical outcomes for patients has been previously described, however none have characterized the ergonomics of these positions for the surgeon (Hamamoto et al. 2017; Li et al. 2015; Peruto, Ciccotti, and Cohen 2009).
Video analysis characterized patterns of risk for muscular strain and overall ergonomics of each patient position on two high-volume arthroscopic shoulder surgeons. Patient height, monitor position, length of arthroscopic equipment and working distance from the surgical field appeared to be risk factors for muscular strain during arthroscopic shoulder surgery. Surgeon A, performing beach-chair positioning demonstrated a number of risks towards neck, back, shoulder, upper and lower extremities during each case. Paramount to neck strain is height of the monitor, as well as height of the patient and surgical field. This has been previously characterized in endoscopic surgery as a risk factor for neck strain (Papaspyros, Kar, and O’Regan 2015; Supe, Kulkarni, and Supe 2010). Sustained or repetitive shoulder abduction has been shown to contribute to neck and shoulder strain or injury (Hegmann et al. 2016; Linaker and Walker-Bone 2015). Increased shoulder abduction was caused by working through lateral portals, though could have been mitigated by repositioning the screen and the surgeon themselves to accommodate. In comparison to surgeon B performing surgery with a patient in the lateral decubitus position, the beach-chair position required no reaching of the surgeon, repetitive or sustained scapular elevation, or composite shoulder motions with arms in abduction. Both surgeons required repetitive and prolonged forearm and wrist motions to complete subacromial decompression and rotator cuff repair, however surgeon B required this with sustained periods of shoulder elevation, flexion, abduction and internal rotation. It was noted that the abducted, hanging arm in the positioner additionally blocks the surgeon’s options for positioning, requiring further reaching around the patient. Given this analysis, it appears that performing these arthroscopic procedures in the lateral decubitus position has inherent risk factors for neck and shoulder strain given the requirement to reach and work through both anterior and posterior/lateral portals, independent of surgical field height or monitor position. Both surgeons were quite static throughout the case regarding their lower extremities, which occurs in arthroscopic procedures, and could benefit from standing pads or shoe-wear to reduce leg and lower back strain.
Characterizing the ergonomics of arthroscopic procedures could provide better evidence for work-place health and safety guidelines and adherence. Given the evidence that orthopaedic surgeons across subspecialties have a high prevalence of WMS, with approximately 10% having missed work or taken leave, providing risk factors and solutions as our study has may have long term financial implications through improved surgeon health and well-being. Minimally invasive or endoscopic procedures carry a higher odds ratio of WMS to surgeons and thus it is important to further characterize the ergonomics of arthroscopic surgery. Our pilot study provides a frame-work for further characterization through gold-standard video analysis and review that may be replicated to better inform the effect of arthroscopy in general, but also the impact of patient positioning as an independent risk factor for WMS. Lateral decubitus positioning has been previously described as more comfortable for the surgeon than beach-chair, however this is based on expert recommendation with low-level evidence and our study challenges this notion (Hamamoto et al. 2017; Lajtai G, Aitzetmüller G. 2017). Surgeons as stakeholders in hospital development work with multidisciplinary teams in implementing change, such as in design of operating rooms (Bayramzadeh et al. 2018). Informing surgeons of risk factors and solutions to WMS and longitudinal career health and safety provides greater evidence based input to these processes.
There are a number of limitations of our study. Our study utilizes two high-volume, fellowship trained shoulder surgeons for comparison. Each surgeon was recorded performing surgery in their patient position of choice, mitigating potential for unfamiliarity. Only three procedures were recorded and analyzed, precluding any potential statistical analysis of risk factors or solutions. Additionally, given the small number of procedures viewed, there is potential bias introduced from spurious actions, and it is impossible to provide a clear trend of recurrent risk factors. The analysis of only two surgeons could provide individual habits not necessarily generalizable to the shoulder surgeon population. Furthermore, only subacromial decompressions and rotator ruff repairs were assessed, which may differ from other procedures, or combined arthroscopic and open procedures. Additional surgeon demographics may factor into ergonomic positioning, as both surgeons were right handed working on right shoulders, and may be different with opposite sides. Video analysis by OT reviewers has been described as the standard in occupational ergonomic assessments which we have been able to provide (Supe, Kulkarni, and Supe 2010). Despite this, analysis from a single reviewer could be limited or biased. The video analysis could not comment on additional mechanical risk factors for strain or injury including force, vibration or contact stress given the sterility of the field. The surgeon’s may suffer from the Hawthorne effect as they are aware that they are being analyzed, changing their performance and affecting the video review (Supe, Kulkarni, and Supe 2010).
CONCLUSION:
Through video analysis of two orthopaedic surgeons, the ergonomics of shoulder arthroscopy has been described for patient beach-chair and lateral decubitus positioning. It is apparent that shoulder arthroscopy provides repetitive motions and positioning of a surgeon’s neck, back, shoulder, and extremities that places the surgeon at risk for muscular strain or injury. Patient height, monitor position, length of arthroscopic equipment, working distance from the surgical field, and patient positioning in the lateral decubitus position appeared to be risk factors for muscular strain during arthroscopic shoulder surgery in this study. Patient positioning in the lateral decubitus position resulted in increased, sustained periods of composite shoulder motions in positions at risk for causing muscular strain or injury about the neck and shoulders. This is due to the position of the patient in the centre of the bed, arm in the surgical field statically, and reaching while using anterior portals by the surgeon. Further study is required to better characterize surgeon ergonomics during arthroscopic procedures to reduce risk of strain and injury. Further work in this field could have profound effects on medical finances and orthopaedic surgeon health.
Statements
The authors have no competing interests or conflicts of interest to report. This study was unfunded.

