

Introduction
The legalization of cannabis in many states, both recreationally and medically, has changed access and utilization across the United States (Petrilli et al. 2022; Kalaba and Ware 2022). The medical implications of cannabis use are complicated, with varying reports on its positive and negative effects on health outcomes as varied as bone health (Menendez et al. 2014), pregnancy (Menendez et al. 2015), and mental health (Court-Brown et al. 1995). Increased access to a drug means more potential users and thus more potential substance use disorders (SUD). SUD frequently co-occurs in patients with traumatic injury (Shymon et al. 2020). SUD not only contributes to onset and severity of trauma itself but also hinders post-trauma care (McCrabb, Baker, Attia, et al. 2019), for example, ongoing substance use contributes to poor adherence to postoperative instructions, increased emergency department (ED) utilization (Thyagaturu, Bolton, Li, et al. 2023; Vakharia et al. 2020; Choi and Kang 2020), and thus potentially poorer clinical outcomes for these patients.
In the setting of orthopaedic trauma, SUD is associated with increased rates of wound infection, malunion, and poor return to function (Petrilli et al. 2022; Lo, Hedges, and Girardi 2022). The detrimental effect of SUD on the outcomes for surgical trauma patients has been described for most drugs of abuse; unfortunately, the impact of cannabis use (which decreases bone density, is associated with increased rates of lower extremity trauma, and predominantly affects younger patients [Kalaba and Ware 2022]) on orthopaedic trauma outcomes has not been well described.
Given the relatively younger age distribution of both lower extremity trauma patients and cannabis use disorder (CUD) patients (Abuse, n.d.), there is a high probability that the patients presenting to the clinic could be cannabis users, both documented and undocumented. In addition, since trauma surgeries are often unplanned, they subject their patient population to a high risk of minimal preoperative optimization. Since hospital readmissions pose a cost and resource burden, it is essential to investigate how having a CUD impacts readmission rates in this population, which will aid in targeting areas where healthcare management can be improved. Cannabis use has been documented to increase, decrease, and have no effect on readmission rates (Abuse, n.d.; Vasilenko, Evans-Polce, and Lanza 2017; C. I. Campbell et al. 2017), varying among different patient populations. Understanding cannabis use and its impact on orthopaedic surgical outcomes could help inform and redesign hospital readmission mitigation strategies.
The increase in the access and utilization of cannabis, with its complex medical implications and effects on bone health and orthopaedic outcomes, warrants an investigation into its impact on trauma patients. The purpose of the current study is to evaluate the demographic composition of the population with CUD and assess its impact on non-union rates and ED utilization following lower extremity long bone fractures. Our hypothesis is that CUD will elevate the non-union rate, and there will be a significantly higher ED utilization rate in this group (Gómez-Barrena, Padilla-Eguiluz, and Rosset 2020; Menendez and Ring 2016; Heath et al. 2022).
Methods
Study design
This study was a retrospective database review (retrospective cohort study with a control group) of a claims database (PearlDiver Technologies, IN, USA), which covers a wide range of medical and prescription data, with records dating from 01/01/2010–10/31/2022. Patients were identified using diagnostic codes within the Central Procedural Terminology (CPT) and International Classification of Diseases (ICD)-9 and ICD-10 classifications system. The database includes claims billed to all payer types, including commercial insurance, Medicare, Medicaid, self-pay, and more. The data is deidentified and compliant with the Health Insurance Portability and Accountability Act (HIPAA).
Study setting and eligibility criteria
Patients records between January 2010 to April 2022 were identified for open and closed surgical procedures for lower extremity fractures (including femoral, tibial, and fibular shaft fractures) and retrieved using CPT codes (CPT-27506, CPT-27507, CPT-27758, CPT-27759, CPT-27784, CPT-27500, CPT-27750, CPT-27780). Patient records with no prior history of the procedure were included and were tracked for 20 years (10 years before and after the index procedures). All patients with an associated claim of CUD (Table 1) were included in the CUD group.
Variables
The primary outcome was the non-union rate at 16 weeks (Court-Brown et al. 1995), at 9 months, and 30-day ED utilization which were defined using ICD-9 and ICD-10 codes, as billed by providers. Diagnosis of non-union is not a standardized process and by nature of database research we cannot know how the physicians came to make the diagnosis, but non-unions should be diagnosed based on both clinical and radiographic features (Andrzejowski and Giannoudis 2019). The non-union rate was reported as a percentage of total patients, while ED utilization was determined using 30-day ED visits and 30-day ED re-admissions for each group. The top diagnoses for readmissions were also reported. The secondary outcomes involved assessing CUD as a predictor for both non-union rates and ED utilization.
Statistical analysis
T-tests and chi-square tests were conducted to compare the demographics for both groups including age (years), gender (male), Elixhauser Comorbidity Index (Maron, Neifert, Ranson, et al. 2020) (ECI, a scale to quantify disease burden in orthopaedic operations of 31 different categories including but not limited to: congestive heart failure, chronic pulmonary disease, renal failure, metastatic cancer, HIV/AIDS, and depression) (Menendez et al. 2014, 2015), percentage of the population with insurance coverage and their respective plans. A multivariable regression analysis to evaluate CUD as the predictor of primary outcomes was conducted, controlling for age, gender, ECI score, percentage of the total insured population and plan.
Results
The query revealed a total of 263,770 patients with surgical procedures for lower extremity fractures not meeting any exclusion criteria, out of which 259,977 were in the control group while 3,793 patients had CUD. Baseline characteristics for both groups revealed significant differences: patients in the CUD group were notably younger (34.47 years vs. 37.78 years), exhibited a higher prevalence of males (64.96% vs. 47.24%), had higher ECI scores (4.55% vs. 3.51%), and showed statistically significant variations in the utilization of insurance plans (Table 1).
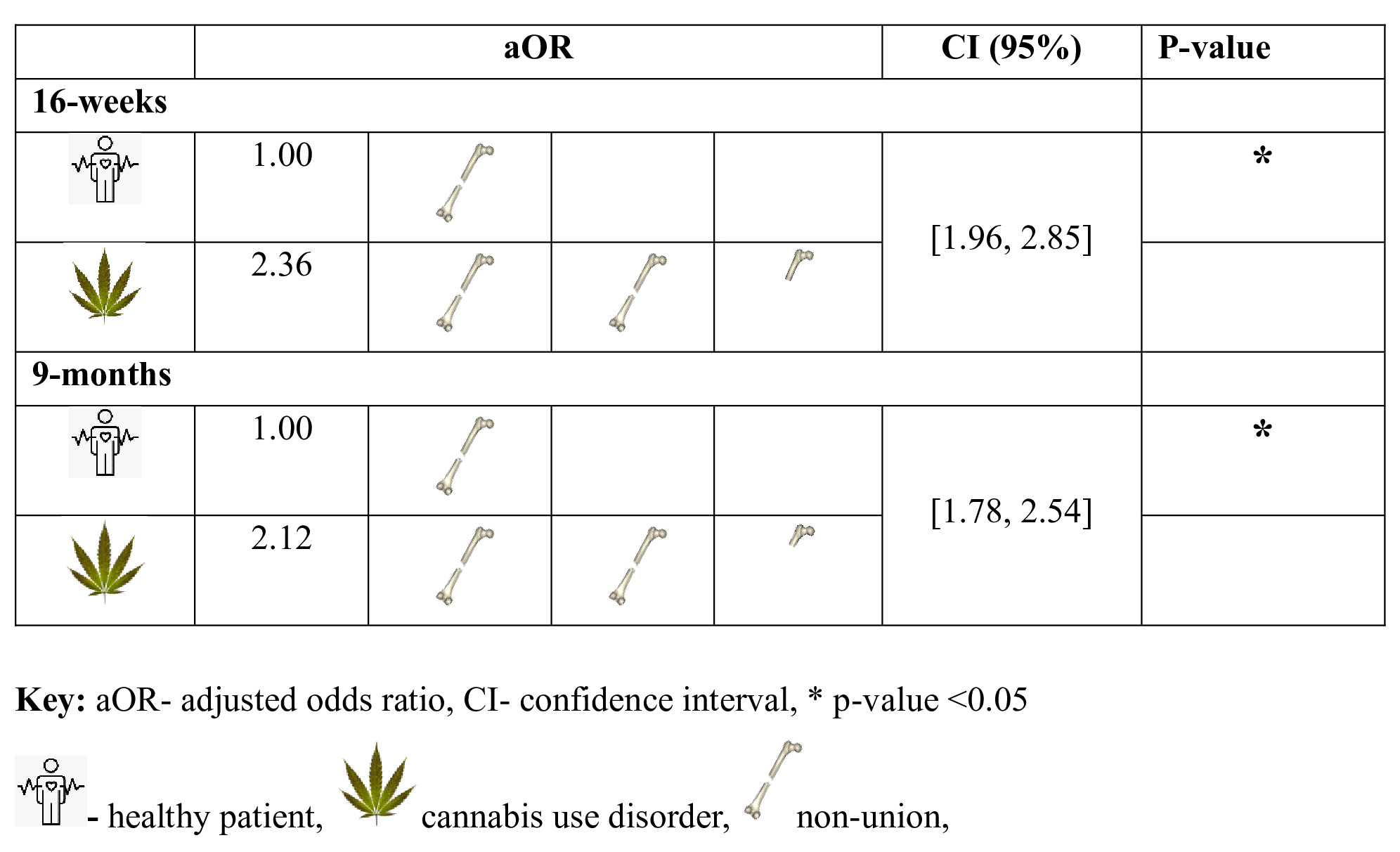
The incidence percentages of non-union at 16 weeks (6.39% vs. 2.55%) and 9 months (6.27% vs. 2.59%) were higher in the CUD group compared to the non-CUD group (Table 2). After controlling for age, gender, ECI score, percentage of insured patients and their respective plans, having a CUD was associated with a 2.36-fold higher likelihood at 16 weeks (95% confidence interval [CI] 1.96, 2.85, p-value < 0.05) and a 2.12-fold higher likelihood at 9 months (95% CI 1.78, 2.54, p-value < 0.05) of experiencing non-union (Figure 1).

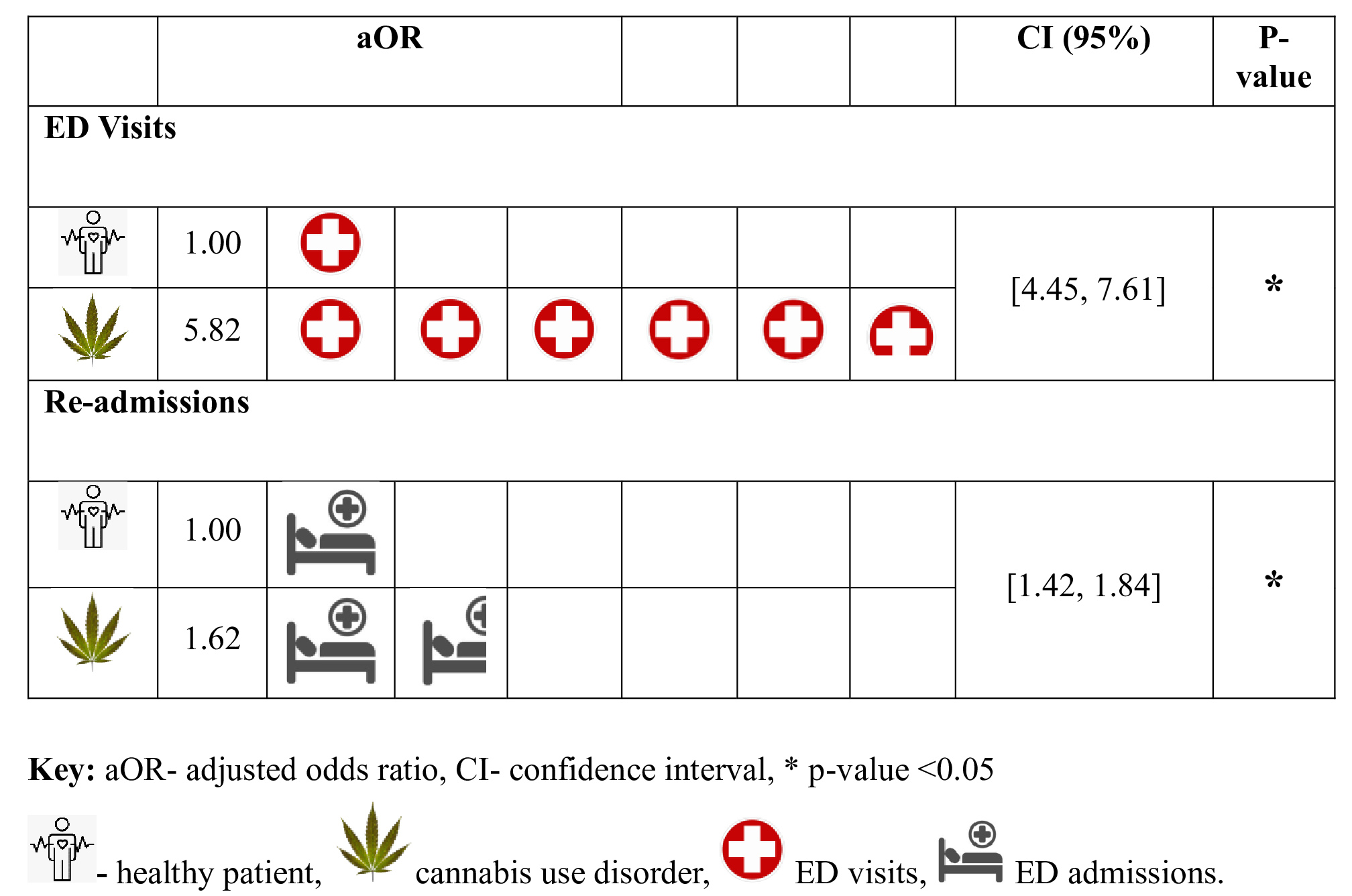
On average, there was a higher percentage of ED visits (52.96% vs 27.31%) and readmissions (22.70% vs 11.20%) in the non-CUD compared to the CUD group (Table 4). In multivariate analysis after adjusting for age, gender, ECI score, and the percentage of insured patients, patients in the CUD group were 5.82 times more likely to have ED visits (95% CI 4.45, 7.61, p-value < 0.05) and 1.62 times more likely to have readmissions (95% CI 1.42, 1.84, p-value < 0.05) compared to patients without CUD within the 30-day period following their index procedure (Figure 2). The admitting diagnosis for readmissions within 30 days included both medical and musculoskeletal causes; however, in the CUD group, psychiatric diagnoses also ranked among the top 10 diagnoses (Table 5).

Discussion
This study leveraged PearlDiver claims database to evaluate the impact of CUD on the incidence of non-union and ED utilization following surgical management of lower extremity fractures.
The results demonstrated that CUD is associated with a higher risk of non-union, observed at both 16 weeks and 9 months post-procedure. Furthermore, individuals with CUD are less likely to seek ED utilization in terms of visits and readmissions. However, when adjusting for potential confounders including age, gender, comorbidity burden, and insurance coverage, CUD becomes an independent predictor of increased ED utilization. This study also offers a demographic profile of lower extremity trauma patients with CUD versus those who do not, which is predominantly younger males (compared to older females in the non-CUD group), patients who have a greater comorbidity burden, and more comprehensive insurance coverage compared to patients presenting with lower extremity trauma without CUD.
While evidence from animal studies indicates that cannabidiol (CBD) agonism does not have detrimental effects on bone healing (Raphael-Mizrahi and Gabet 2020), animal studies with direct cannabis smoke do show impaired bone healing (Heath et al. 2022). This brings out an important distinction. Cannabis contains cannabinoids, the chemicals found within cannabis. Cannabinoids include both tetrahydrocannabinol (THC), a psychoactive component of cannabis, and CBD, a non-psychoactive component. These terms are often used and thought of interchangeably, but they are different compounds with different properties The key insight is that the impact of cannabis smoke on bone healing cannot be solely attributed to CBD or THC, underscoring the multifaceted nature of cannabis and the imperative for more targeted and comprehensive research to elucidate its specific components and mechanisms.
Our study highlights how the incidence of non-union rates remains high in patients with CUD, even when controlling for potential confounders such as demographics and comorbidity burden. Drawing conclusions regarding how CUD impacts bone healing is challenging due to limited and conflicting data in human subjects. Clinical studies on human subjects offer evidence that associates heavy cannabis use with high bone turnover, low bone density, and an increased risk of fracture (G. M. Campbell and Sophocleous 2014) or increased risk of revision after arthroplasty (Heath et al. 2022), while other studies have found no difference in the rate of joint revision and have shown improved healing of chronic wounds (Heath et al. 2022). Future research with larger, well-controlled clinical studies is necessary to elucidate the precise impact of cannabis use disorder on bone healing and to guide evidence-based recommendations for patient management.
There is a high prevalence of co-existing psychiatric disorders in patients with CUD (Hasin and Walsh 2021). This is also evident in our study, where psychiatric illnesses constitute a significant portion of the top 30-day admitting diagnoses in the CUD group. Psychiatric co-morbidities complicate rehabilitation for lower extremity long bone injuries, impacting patient engagement and adherence to care routines. Anxiety and depression may hinder motivation and resilience, leading to non-compliance with rehabilitation regimens. Additionally, the use of antipsychotics may impact metabolic processes, increasing the risk of fractures (“The Risk of Bone Fracture after Long-Term Risperidone Exposure Is Not Increased Compared to Other Atypical Antipsychotics: A Retrospective Cohort Study,” n.d.) which may also explain the increased non-union risk in this cohort. Consequently, a collaborative approach involving orthopaedic surgeons, mental health professionals, and primary care providers is crucial for comprehensive care of orthopaedic trauma patients.
The CUD group displayed lower 30-day ED utilization following their fracture procedure. Increased healthcare utilization in CUD patients may be more closely tied to underlying substance use behavior than cannabis use itself. When adjusting for confounding variables, a noteworthy positive predictive relationship between CUD and 30-day readmissions emerged. There is evidence suggesting that patients with marijuana use disorder exhibit high rates of inappropriate use of healthcare services in the ED. Effectively addressing their comorbid conditions may help reduce this unnecessary reliance on emergency care (C. I. Campbell et al. 2017). CUD patients are more likely to seek addiction treatment and other specialized services, as well as primary care services, following an inpatient encounter. This potential linkage could reduce the need for subsequent acute care. Previous studies conducted in healthcare delivery systems in northern California have indicated that patients who maintain ongoing primary care and addiction treatment are less likely to have subsequent ED visits and inpatient admissions which explains the lower 30-day ED utilization in CUD group before adjusting for confounders.
CUD is an independent predictor of ED utilization which can be explained by the observations within our study. The admitting diagnoses for 30-day readmissions in the CUD group were mostly related to pain and psychiatric concerns. Secondly, CUD may complicate their post-operative care leading to higher medical complications, prompting them to seek ED services.
This study has several limitations. Firstly, we utilized a large database where it is difficult to get granularity in the results, such as method of ingestion of cannabis, whether a user used medical marijuana or not, and the accuracy of eligibility of identified patients are dependent on how and when CPT/ICD 9/10 codes were coded. For example, some physicians may personally deem 16 weeks too early to diagnose non-union, and thus some patients could be missing from this group. We felt it was worthwhile to include this group because non-unions diagnosed in this timeframe may potentially be worse and thus of clinical significance and potentially worth research in the future. Subsequently, the eligible population potentially missed individuals with undocumented cannabis use. Similarly, stigma associated with drug use may have led to undisclosed cannabis use in our control group. Due to the non-uniform legalization of cannabis across the U.S. and significant underdiagnosis in the country (Bonn-Miller, Bucossi, and Trafton 2012), we selected the Pearldiver database to include a large population. Consequently, due to coding limitations there was a stark difference in numbers between the control population and the population with CUD. We did not explicitly control for other substance use disorders, beyond their inclusion in the ECI, which may exist in this patient population. Despite these limitations, our exploration of cannabinoid uses in patients undergoing long bone fracture procedures emphasizes the importance of targeting the causes of 30-day readmissions to reduce ED utilization post-surgery. Prospective studies should examine outcomes in relation to the extent and severity of marijuana-related problems.
Future research on this topic could focus on a number of different variables. One potential area of interest for future investigations is whether route of ingestion in CUD plays a role in outcomes. Another could be studying what percentage of those with CUD used marijuana medically and whether that impacted outcomes. Additional studies could look to stratify patients based on which lower extremity weight-bearing bone was fractured, as the clinical course for these fractures can vary, as well as report on causes of non-union in cases where the cause is known.
Conclusion
This study investigates the interplay between CUD and outcomes in lower extremity long bone fracture surgeries. CUD patients are typically younger, male, and have a higher comorbidity burden. Individuals presenting to orthopaedic trauma care with CUD are at a higher risk of non-union at 16 weeks, at 9 months, and 30-day utilization of the ED.