



Introduction
Total knee arthroplasty (TKA) is the current gold standard treatment for end-stage osteoarthritis of the knee. However, multiple documented reports have found rates of dissatisfaction to be as high as 20% (Gunaratne et al. 2017). Post-operative dissatisfaction is often multifactorial with patients citing continued pain, decreased mobility, limited improvement in knee function, and chronic swelling (Gunaratne et al. 2017). Acute tissue swelling after TKA can lead to overall patient discomfort, decreased joint range of motion (ROM), while lengthening the post-op recovery period (Battista and Wickline 2023). Previously published literature has found that 10-34% of TKA patients still experienced surgical site discomfort three months after surgery (Wylde et al. 2018). Moreover, 20% of individuals observe increased swelling and discomfort post-surgery compared to their preoperative condition (Battista and Wickline 2023; Beswick et al. 2012; Li et al. 2020). Substantial tissue injury sustained during the TKA procedure precipitates a complex cascade of inflammation resulting in tissue swelling contributing to most reported post-operative complications (Osei, Rebehn, and Boyer 2016).
Single-frequency bioelectrical impedance analysis (SF-BIA) is established as an effective and efficient way to measure swelling after a TKA (Loyd et al. 2021). The measurement is easy to perform and does not exert additional stress on the patient (Battista and Wickline 2023). SF-BIA has been used to monitor swelling after TKA and provide a baseline curve including the top and lower percentiles for swelling over six weeks postoperatively (Loyd et al. 2021). A follow-up study out of the same program demonstrated decreased swelling and a 93% satisfaction rate utilizing a compression garment, home exercise, and manual lymphatic drainage (Carmichael et al. 2022).
The lead author of this study has previously published a TKA perioperative protocol outlining a standardized patient program that includes education in print and video format, recommending a pre-and post-op anti-inflammatory diet with protein supplementation emphasis, encouraging low impact pre-op exercise, foregoing tourniquet use intraoperatively, MCL-sparing kinematic surgical technique, utilization of a sagittally stable knee implant, post-operative low weekly step count maximums, home exercise program in lieu of formal PT, prescriptions of low dose prednisone, aspirin and non-steroidal anti-inflammatory drugs (NSAIDs), and no strengthening for 6 weeks (Wickline et al. 2023).
The purpose of this study was to compare patient outcome measures after the addition of an intraoperative anti-inflammatory bactericidal rinse, a post-operative cryocompression device, extended length oral tranexamic acid, and edema-controlling stockinette to previously published control group data (Wickline et al. 2023).
Methods
This non-concurrent cohort study was conducted to measure the effects of peri-operative treatment algorithms on post-operative swelling in patients undergoing TKA. Subject data from three trial sites were included in this study, Genesee Orthopedics & Plastic Surgery Associates (New Hartford, NY), St. Elizabeth Medical Center (Utica, NY), and Apex Surgical (Westmoreland, NY). All TKA procedures were conducted by a single surgeon.
All participants included in this study were ≥18 years of age, having been scheduled to undergo unilateral primary total knee replacement. Participants included in this study also provided informed consent, were willing and able to follow post-operative protocol requirements, and had no contraindications to the procedure. Additionally, subjects agreed to the purchase of a cryocompression device and patented lymphatic stockinette. Enrolled patients committed to appointments for SF-BIA assessments at the interval of pre-op, 7-, 14-, 21- and 42-days post-operative. The study was conducted in accordance with Health Insurance Portability and Accountability Act guidelines, adhered to tenets of the International Conference on Harmonization E6 Good Clinical Practice (ICH GCP) and the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Review Board (IRB) for the Protection of Human Subjects of Mohawk Valley Health System in Utica, NY. All patients provided written consent to use de-identified data for the purpose of this report. No compensation was given for participation.
Participants were excluded from participation if they previously had major lower extremity surgery within 6 months on the opposite side or major lower extremity surgery on opposite side with permanent resultant lymphedema / swelling or pre-op findings noted that one leg was markedly larger than the other (>20%). No patients on dialysis or having a glomerular filtration rate < 30 mL/min/1.73 min (Battista and Wickline 2023) were included. Patients having previous vein harvesting for coronary artery bypass graft, history of vein surgery or artery bypass below aortic bifurcation, post gastric bypass, positive findings for rheumatoid arthritis, pacemaker or implantable defibrillator were also excluded. Pregnant or lactating females were not included in the trial. Subjects taking loop diuretics, opioid analgesics (>5 pills within 90 days of surgery), and anticoagulants (other than aspirin) were also excluded. Furthermore, subjects unable to follow study protocol instructions or provide informed consent or those residing more than 20 miles from the office site did not meet inclusion criteria.
All patients received the same baseline swelling reduction interventions as described previously, and historical controls were extracted from that study (Wickline et al. 2023). In addition, the multimodal group had four additional interventions: intraoperative anti-inflammatory bactericidal irrigation solution (XPERIENCE® Advanced Surgical Irrigation, Next Science ®, Jacksonville, FL), post-operative cryocompression, (Polar Care Wave, Breg Inc., Carlsbad, CA), extended length oral tranexamic acid (1300mg daily for 15 days), and patented edema-controlling stockinette (EdemaWear®, Compression Dynamics, LLC. Omaha, Nebraska). (Figure 1) Patients were instructed to use the stockinette 24/7 and the cryocompression at least 14 times a day for 30-40 minutes for two weeks. After the two week visit, patients were no longer required to use the stockinette and could reduce cryocompression to six times per day.
There was no funding, compensation, or product support provided by any of the companies whose products were used in this study.

Study Assessments
Single frequency-bioimpedance (SF-BIA)
Single frequency-bioimpedance (SF-BIA) assessment was used to measure lower extremity swelling. Measurements were obtained using the Quantum® II body composition analyzer (RJL Systems, Clinton Township, MI). Subjects were made to lie flat for 10 minutes.
Four surface electrodes were placed on the non- surgical limb as described below.
-
20 cm proximal to the superior pole of the patellar over the midline of the thigh.
-
10 cm proximal to the superior pole of the patellar over the midline of the thigh.
-
On a point midway between the medial and lateral malleolus.
-
10 cm distal to the midway point between the malleoli over the 2nd ray.
Once appropriately placed, the electrodes were attached to the SF-BIA device. The device was turned on and after a lag of at least 5 seconds, values were recorded. The same procedure was then followed for the surgical limb. Lower levels of assessed bioimpedance indicated higher fluid content and therefore greater swelling. Percent swelling was calculated as a difference in the surgical limb to the non-surgical limb using the formula:
(1−(surgical limb BIA ÷nonsurgical limb BIA)) × 100%
Normalizing swelling in the surgical limb against the non-surgical limb of the same patient enabled accurate measurements of changes in fluid status in the surgical limb over time and allowed for valid swelling curve comparisons within and between cohorts despite the variability in body compositions. After normalization, the swelling calculated pre-op was subtracted from the swelling calculated post-op. This calculation yielded the difference in swelling at each time point. The time points and time frame for swelling evaluations were selected based on prior observations by the principal investigator on typical post TKA pain spikes and previously published timepoints to allow for direct comparison.
Patient Satisfaction
Patients were contacted via phone after their six-week follow-up appointment for their opinion of the post-operative therapeutics added to the protocol. (Figure 2) They were asked about their overall satisfaction with the post-op regimen, choosing from very satisfied, satisfied, neutral, unsatisfied, and very unsatisfied. Patients also rated their comfort with the edema-controlling stockings and cryotherapy on a scale of 1-10, 10 being the most comfortable. Additionally, participants were asked if they had experienced any specific issues with the protocol.

Range of Motion
Range of Motion (ROM) measurements were obtained by the primary author with a goniometer pre-operatively, 2-weeks post-operatively, and 6-weeks post-operatively.
Statistical analysis
Outliers have been included in the analysis as nonparametric tests are robust to skewness and medians are reported, which are inherently skewed less by outliers. To avoid inaccurate results, missing values were excluded from the analysis and no interpolation methods were included. Hence, sample sizes for 21- and 42- for the multimodal treatment plan and for 14-, 21-, 42- for the control treatment plan vary from their respective participant totals. The Mann-Whitney U test has been analyzed as an alpha value of 0.05 and is two-tailed.
The primary method for analyzing the data was through a Mann-Whitney U test. Nonparametric analyses provide a perfect realm in analyzing dataset that have sample sizes too small for assuming any distribution form, including the Gaussian/normal distribution, or skewed data. Assumptions for the Mann-Whitney U test are sound and has been tested using the Levene Test of Homogeneity of Variances. Both the primary test and the assumption verification test were performed at a level of significance α = 0.05 and in a two-tailed manner. All analyses have been performed through R (version 4.0.1) utilizing the car, effectsize, and pwr packages.
Results
This analysis was performed to determine if there is a difference in SF-BIA measurements between the updated multimodal treatment plan cohort compared to outcomes of subjects in the control treatment plan cohort at 7-, 14-, 21-, and 42- postoperative days. There was a total of 24 subjects participating in the updated multimodal treatment plan compared to 30 participants in the historical control group that were included in the analysis. The average age for the control was 68 compared to 66 in the multimodal cohort, 63% of patients in the control had a BMI >30 compared to 70% in the multimodal cohort, in both groups three patients had diabetes. As seen in Figure 3, Outliers are noted in the control plan at 7-, 21-, and 42- days postoperative.
Descriptive statistics are outlined in Table 1 and visualized in Figure 3a-d.

Prior to moving forward with the Mann-Whitney U test, the assumption for the test having two samples of uniform variances must be satisfied. This has been tested in the data through the Levene Test for homogeneity of variances. The results for the Levene Test are shown in Table 2.
The null hypothesis of the Levene test is that the variances between the groups are the same (homoscedasticity is achieved), whereas the alternative hypothesis states that the variances between the groups are different (heteroscedasticity is achieved). Since the p-values for seven days postoperative is 0.4604, fourteen days postoperative is 0.826, twenty-one days postoperative is 0.1196, and 42 days postoperative is 0.4969 are all greater than the level of significance set at 0.05, we fail to reject the null hypothesis that the variances between the cohorts are the same at all postoperative intervals. Hence, the Mann-Whitney U test assumption of equal variability in the dataset is satisfied.
Analyzing the groups at the different increments individually allows us to pinpoint when the differences between the two plans are significantly different. Therefore, multiple iterations of the Mann-Whitney U test were performed. Results for the Mann-Whitney U test are outlined below in Table 3.
The hypothesis for the Mann-Whitney U test are as follows:
H0: There is no difference in medians between patients in the multimodal and control plans
H1: There is a difference in the medians between patients in the multimodal and control plans
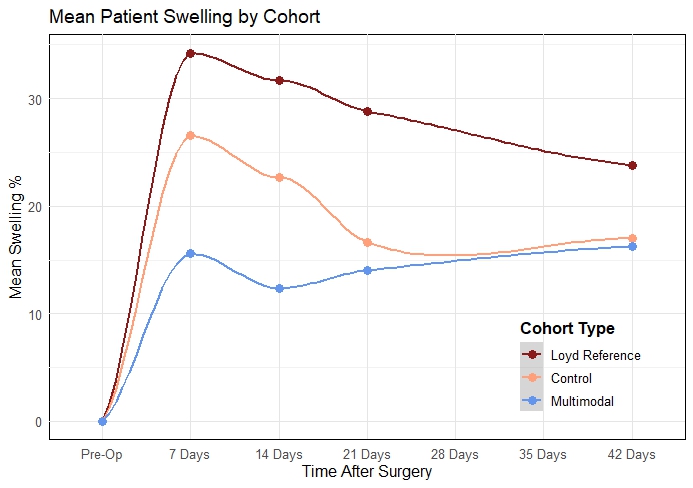
When comparing the Multimodal perioperative protocol to the Control, the difference in SF-BIA measurements was seen as statistically significant in the earlier portion of the healing process, with p-values of 0.0054 and 0.0036 after 7 days and 14 days respectively (Table 3). This suggests that our multimodal swelling protocol (bactericidal lavage, cryocompression, extended oral tranexamic acid, edema stockings) is better at reducing early postoperative swelling than conventional treatment.
The shift parameter (median of differences sample observations of the multimodal cohort and the control cohort), as well as the confidence intervals at 95%, were calculated for each post-op milestone. The shift parameter and confidence intervals are 11.66 CI 95% [3.79,19.42] after 7 days post-op, 10.56 CI 95% [2.97,16.88] after 14 days post-op, 4.89 CI 95% [-4.09,14.07] after 21 days post-op, and 0.96 CI 95% [-6.70,8.05] after 42 days post-op.
The effect size and power of the analysis for the statistically significant postoperative intervals 7 days and 14 days were calculated using a rank biserial test and the test for two proportions of different sizes. Both tests were ranked at a level of significance of 0.05 in a two-tailed fashion. Values for the effect size and power of each significant result is outlined in Table 4.
The power of the study for the statistically significant postoperative intervals is at 36.2% at 7 days and 38.5% at 14 days. The mean patient swelling by cohort is illustrated in Figure 4.

In addition to patient swelling metrics, the overall patient satisfaction in the multimodal cohort and the knee flexion ROM for both the control and the multimodal cohorts were also recorded. Details for these metrics are shown in Table 5.
Of the 25 patients in the multimodal cohort, 24 participants ranked the treatment option as “very satisfied,” and 1 participant ranking the plan with “satisfied.” All participants in the multimodal plan would recommend this perioperative treatment plan to individuals who also needed a TKA procedure. The averages for the edema wearing and comfort, as well as the Breg comfort, were scored highly and found to be 9.56, 9.56, and 9.25, respectively.
The average postoperative knee flexion ROM scored better in the multimodal cohort than the control cohort. Mean knee flexion ROM in the multimodal cohort were 114.52 in multimodal versus 110.71 in control after 14 days postoperative treatment and 122.28 in multimodal versus 119.6 in control after 42 days postoperative treatment. (Table 6)
Discussion
Despite overall success in terms of returning to activities of daily living, total knee replacement is a much-feared procedure by the general public due to historical association with pain, concern for return to high-level activities, and long recovery (Suarez-Almazor et al. 2010). In fact, Kelly et al. showed that swelling and pain related to the procedure were the most frequent reasons for 90-day ED visits after both THA and TKA (Kelly, Prentice, and Wang 2018).
It therefore stands to reason that recovery protocols which help mitigate the intensity of the inflammatory response may yield less pain and opioid usage, faster range of motion recovery, less arthrofibrosis, potentially lower 90-day episode of care costs (through lower recidivism/ER utilization), and ideally earlier resumption of normal activities and thereafter sport activities.
Previous studies by the lead author using an inflammation/swelling reduction protocol have indeed led to extremely low post-op operative opioid usage (10 pills or less) and have lower than expected average swelling at POD 7 and 14 as compared to the national normative reference chart (Stevenson and Wickline 2020). Lower post-operative swelling was associated with improved range of motion, less opioid usage, and earlier cessation of assistive devices (Battista and Wickline 2023).
In the lead author’s experience, aggressive post-operative therapy protocols lead to the greatest increases in post-operative swelling compared to other factors. He believes that studies that look to quantify the effectiveness of other swelling reduction interventions without instituting a gentle post-operative therapy protocol will likely fail to show a difference due to the magnitude of swelling caused by aggressive therapy protocols. This is the reason that tourniquet and cryotherapy studies have been inconclusive to date. Interestingly, the Denver group that provided cases for the Loyd reference swelling paper subsequently published a follow-up paper showing much lower swelling values when an at-home therapy protocol was included in their new protocol (Loyd et al. 2021; Carmichael et al. 2022). Therefore, it would be ideal if another research center directly compared an aggressive therapy protocol and a therapy protocol such as the one proposed by Wickline et al (Wickline et al. 2023). to verify this belief using single channel bioimpedance with the same measuring tool.
Like the lead author, once a research site verifies that a change in the post-op therapy protocol yielded a substantial improvement in swelling, then that site can begin looking at other factors that may reduce swelling (such as tourniquet usage and cryotherapy etc.) and may be able to find significance due to removing the therapy variable as a confounder.
In previous work, Wickline et al. showed that a specific antibacterial rinse also had anti-inflammatory properties when compared to dilute povidone-iodine (Battista and Wickline 2023). Therefore, this rinse was incorporated into the protocol (Battista and Wickline 2023).
Due to the logistical challenge of obtaining 7 and 21 post-operative day data, three additional interventions were chosen to add to the control protocol to allow for a smaller sampling size and ideally show enough improvement to achieve significance. It is not conceivable that POD #7 swelling will ever reach zero and indeed may never dip below 10%. The following paragraphs discuss the basis for cryocompression, extended length tranexamic acid (TXA), and a unique, patented compression stockinette made with patient compliance in mind.
Rest, ice, compression, and elevation are mainstays of treatment for acute musculoskeletal injuries with most surgeons recommending icing following joint replacement surgery. Application of ice follows the principles of thermodynamics where collision theory suggests that temperature reduction leads to less molecular kinetic energy leading to fewer collisions between molecules and thereby decreasing the rate of inflammatory chemical reactions (Libretexts 2022). Cryotherapy has evolved from simply being plastic bags containing ice cubes (first generation) to circulating ice water (second generation) to electronically controlled devices which allow for improved control of the cold therapy (third generation) (Thacoor and Sandiford 2019). Clinical studies looking at models of knee swelling have found that cryotherapy can offset reductions in quadriceps strength associated with intra-articular swelling (Rice, McNair, and Dalbeth 2009). A Cochrane review on the use of cryotherapy from 2012 evaluated 11 randomized controlled trials finding evidence supporting lower blood loss (255 mL), improved pain control (-1.3 points on VAS scale) at 48 hours (not 24 or 72 hours), or improved motion at discharge (11 degrees) but the authors noted that these were all backed up by low quality evidence (Adie et al. 2012). Cryotherapy – particularly third generation (computer assisted) cryotherapy – has been shown to reduce opioid consumption compared to controls by up to 40-60% (Wyatt et al. 2023; Brouwers et al. 2022; Thijs et al. 2019; Su et al. 2012). Additionally, cryotherapy has been shown to increase flexion by 5-10 degrees at early time points up to 6 weeks postoperative (“Van Ooij B et Al.” 2020). One advantage with third-generation cryotherapy units is that they not only provide lower temperatures to the skin but also an element of compression to help drive the cold deeper into the tissues. Compression may also decrease bleeding from injured tissues like applying pressure to any dermal laceration.
The use of tranexamic acid (TXA) has become widespread over the last decade and a half in total joint arthroplasty, mostly as a means of reducing the likelihood of postoperative blood transfusion. Almost all surgeons administer TXA through an intravenous route prior to incision and most often at the time of closure but studies have shown that additional postoperative doses can further decrease blood loss (Wang et al. 2019; Lei et al. 2020).
Multiple studies have shown that extended TXA has demonstrated improved reduction of post-operative edema (Wang et al. 2019). Additionally, Lei et al. found a dose-dependent decrease in pain with additional doses of TXA (Lei et al. 2020). Recent publications illustrate the utility of TXA to reduce inflammatory mediators and decrease the incidence of post operative infection (Draxler et al. 2019). The 2023 AAHKS Clinical Research Award Paper was given to Kirwan et al. for their investigation on TXA versus placebo for 3 days postoperative; they found that the TXA group had increased knee flexion at 6 weeks (116 vs 107 degrees) and improved pain scores at 2 and 6 weeks (2.5 vs. 3.9 and 1.4 vs. 2.8, respectively) (“Award Study Investigates the Safety and Clinical Efficacy of Extended Postoperative Oral Txa Use in Total Knee Arthroplasty” 2023).
There are not many contraindications for the use of TXA. Per recent clinical practice guidelines put forth by the American Academy of Hip and Knee Surgeons, administration of TXA is not considered unsafe in patients with a known history of venous thromboembolism, myocardial infarction, cerebrovascular accident, transient ischemic attack, or prior vascular stent placement. Caution should be used with extended dosing of TXA in certain populations, including those with renal insufficiency and seizure disorder (Fillingham et al. 2019). Tranexamic acid is 95% excreted in the urine so extended use of this agent in patients with severe renal impairment is not recommended; no dose adjustments are needed in patients with hepatic impairment (Fillingham et al. 2019). Additionally, patients who have active thromboembolic disease are not routinely given an antifibrinolytic such as TXA (Fillingham et al. 2019). Finally, it should be noted that the only true contraindication to administering TXA is in patients with known anaphylaxis to this medication (Fillingham et al. 2019).
Although there is a plethora of data supporting the use of compression devices in the management of chronic venous disease and/or lymphedema, to date the utilization of compression for edema reduction post TKA has been driven by surgeon preference rather than evidence based. The use of an elastic wrap (ie., - ACE wrap) immediately post-surgery historically was cited to increase compartment pressure and help to reduce bleeding, tissue edema and size of effusions (Brodell, Axon, and Evarts 1986). However, a more recent meta-analysis concluded there was insufficient clinical evidence to support routine use of compression bandage (Liu et al. 2020).
Anti-embolic stockings (AES,i.e. -TED hose), conventionally included as one of the prophylactic methods employed to prevent venous thromboembolism (VTE) in an immobile patient, has also been used ‘off-label’ in the ambulatory patient to assist with edema management post TKA. Beyond the lack of definitive evidence relative to the effectiveness of AES, there are practical barriers to proper utilization of elastic anti-embolic stockings including body habitus and surgical incision sites. Patients, family, and even medical staff struggle with donning/doffing the compression stockings even when applied to a normal shaped limb. Often patients’ body habitus (specifically calf size relative to thigh circumference) does not match up with sizing guidelines resulting in ineffective compression dosage delivery and may contribute to edema formation and/or superficial tissue damage due cording or rolling of the compression textile (Best et al. 2000).
The efficacy of other types of compression devices, including short stretch compression bandages, traditional compression stockings (thigh high), Velcro wraps and advanced textiles touting semiconductors embedded within the fabric have also been studied. Comparison of the outcomes is hindered by differences in their methodologies, sample size and variables measured.
The STICKs study evaluated the impact of the application of short stretch compression bandages on the full leg (Brock et al. 2017). The authors found no significant difference in knee swelling, range of motion, pain score, or length of stay between the control group, which did not receive compression, and the treatment group, which received compression with a short stretch bandage applied only during the first 24hrs (Brock et al. 2017). Similarly, Munk et al. observed no substantial effect on knee swelling or pain score following the use an elastic compression thigh high stocking for one month following total knee arthroplasty (Munk et al. 2013). Hendrickx et al., evaluated inelastic adjustable compression wrap and found no effect on swelling in the acute postoperative phase (0-2 days) however did observe reduced swelling at day 14 within the subacute phase (Hendrickx et al. 2020). A positive impact was observed by Justice and Jacob, citing a reduced effusion and improve knee flexion in the study group using what was described as ‘a non-compressive sleeve embedded with semiconductor elements (Incrediwear).’ Outcomes were assessed 3 weeks after total knee arthroplasty compared to traditional compression stocking*.* (Justice and Jacob 2023)
In a previously published call to action paper outlining the importance of perioperative protocols to control post-operative edema, the lead author reported positive result with the use of an innovative compression stockinette in both the pre-op and post-operative phase (Wickline et al. 2023). Clinically referenced as a longitudinal, elastic stockinette, or ‘fuzzy wale,’ this compression stockinette features a patented design with vertically oriented, alternating channels of high compression and area of little or no compression. This design applies compression to only 30% of the skin, leaving the other 70% uncompressed, and has been clinically reported to reduce edema (Ehmann et al. 2020).
With a resting pressure of only 8-12mmHg, the mechanism of action is hypothesized to stem from the mechanics of the dermal lymphatics which are stimulated by dermal stress and strain (Jafarnejad et al., n.d.). Lymph flow from the tissue into the initial lymphatic capillaries depends on oscillating and gradient pressures.36.37 The unique pressure profile facilitates formation of tissue channels, even in areas where dermal lymphatics are impaired as seen in patients with excessive tissue fibrosis. Dermal lymphatics are responsible for the uptake of extracellular fluid, or edema in the tissue, and account for 70% of the lymphatic system (Solari et al. 2020).
Additionally, unlike other compression stockings which can be extremely difficult to apply, in the authors’ experience this product is easy for patients to apply even after TKA. The ease of donning and low resting pressure may have contributed to increased compliance in the study. The “small-shaped” size was found to fit patients with thigh circumference less than 24" and the medium thigh high product for thighs measuring >24".
Thus, this investigation supports the use of the updated Multimodal perioperative treatment algorithm including the intraoperative use of an anti-inflammatory bactericidal rinse and post-operative cryocompression, extended length oral tranexamic acid (TXA) (1300mg daily for 15 days), and edema-controlling stockings was more effective in decreasing post-operative edema than the control in patients undergoing TKA early in the postoperative course being significant at both the 7 day and 14-day mark. Two weeks after the procedure date, all three post-operative interventions in this multimodal protocol (TXA, cryocompression, and edema stocking) were discontinued. The regression of gains achieved in the first two weeks with the multimodal swelling protocol certainly presents an opportunity to continue one or more interventions beyond two weeks. Similar increases in swelling were also noted by Carmichael et al. after removal of all interventions (Carmichael et al. 2022).
Consideration of patient satisfaction for treatments inherently promotes holistic care. With all but one patient in the multimodal treatment cohort being “very satisfied” and the other patient being “satisfied” with its protocol, as well as a 100% rate of recommending the protocol, the multimodal treatment approach was one that overall fared very positively. Although there are additional materials that the patients in the multimodal cohort had to use and follow (i.e. the stockings and the cryocompression unit) which may deter from compliance, the mean scores for usage and comfort of these materials were greater than 9 with medians of 10 for each scalable category. This suggests that these additional materials may not be perceived as a burden for patients to use in their postoperative care.
Patient satisfaction may also be increased and relatively more favored in protocols that show improved functionality. When comparing the multimodal to the control cohort, the average postoperative knee flexion ROM scored consistently better in the multimodal cohort. Average knee flexion ROM in the multimodal cohort was 4 degrees greater than the control cohort after 14 days postoperative and 3 degrees greater than the control cohort after 42 days. With higher average knee flexion ROM seen early in the healing process, patients may perceive the treatment they are doing as beneficial, improving compliance for the protocol as the treatment period continues.
Limitations
There are limitations to this study. The first is that it is a non-randomized, non-concurrent cohort study with a small sample size by design, as this was a feasibility study. The multimodal swelling protocol was offered to every patient, but due to the cost and additional postoperative visits involved, some patients only opted to selectively purchase only one or two of the items in the protocol and were not included in the study. More motivated patients could have purchased cryotherapy device and edema stockings; these patients could have been more compliant with other recommendations for postoperative care (rest, elevation, step counts) which would also improve outcomes further in the multimodal group. Since all items were bundled in the protocol at once, the authors are unable to ascertain whether all the benefit is coming from one intervention or a synergistic combination of the four.
Conclusion
This pilot feasibility study was conducted to collect data to assist in powering a future larger cohort trial. When other surgeons look to add components of this multimodal swelling protocol to their practice, they could perform additional prospective studies adding one of these items at a time to see which may be more beneficial than others. Additionally, it would be recommended to try the interventions for 3-4 weeks’ duration rather than just 2 weeks to see whether the benefits seen at the 14-day timepoint carry forward to 21 or 42 days postoperative.
Edema management in the peri-operative phase has the potential to positively impact both surgical and patient outcome measures. The proposed multimodal swelling protocol has demonstrated a positive effect on edema in the immediate post-operative phase. Additional investigation is required to determine the unique effect of each component (i.e., anti-inflammatory antibacterial rinse, TXA, cryocompression, longitudinal stockinette). Furthermore, there is a need to determine whether the length of multimodal protocol (4-6 weeks vs. 2 weeks) and/or a different dosage of TXA may also impact outcome measures. Other elements recommended for future studies that should be considered include how to mitigate the increase in swelling after patients become more active or how to further fine tune recommendations for step counts to help minimize swelling.
One final but important consideration when implementing this protocol is that it was developed by a surgeon who eschews formal physical therapy for the first six weeks, like the way one would treat an ankle fracture or tibial plateau fracture. An attempt to replicate these results while still using aggressive physical therapy protocols would be unlikely to have a similar outcome. This is due to the amount of swelling generated by thrice a week therapy session obscuring positive but small gains in swelling reduction from each tested modality.