
Introduction
Anterior cruciate ligament (ACL) injuries are becoming more common in the United States with a reported 200,000 cases annually (Looney et al. 2020). These commonly present following a non-contact twisting injury to the knee with an associated swelling of the joint. ACL injuries are commonly treated with reconstruction rather than repair to reduce time away from activities or respective sports. With operative treatment, this helps restore functional stability and has been shown to reduce subsequent meniscus and cartilage damage (Looney et al. 2020). To date, the reported graft failure rate for primary ACL reconstruction is approximately 2-8 percent (Grassi et al. 2017). With failure rates reaching nearly eight percent, revision ACL reconstructions are becoming more prevalent with approximately 13,000 cases performed in the United States each year (Grassi et al. 2017). Studies have shown that revision ACL reconstructions not only result in less optimal outcomes but carry a risk of failure of about 2 to 5.4 percent (Grassi et al. 2017). Graft selection with or without augmentation in ACL reconstruction is a debated topic. FlexBand (Artelon, Marietta, Georgia) has offered promising results as a safe bio-scaffold for augmentation in the knee and ankle (Kelly et al. 2021; Myers et al. 2022). Artelon is a polyurethane urea bioaugmentation substance that has been used for a variety of purposes, including reinforcement of soft tissues, and can be used clinically for the treatment of osteoarthritis (Ko et al. 2011; Robinson and Muir 2011). Additionally, Artelon has demonstrated non-inferior results compared to primary repair in collateral ligament injuries associated with knee dislocations (Myers et al. 2022). This case report discusses two similar patients who underwent a revision ACL reconstruction utilizing Artelon as a bio-scaffold.
Statement of Informed Consent
Both patients agreed to participate and volunteer their information in accordance with this study. They were informed that data concerning the case would be submitted for publication and each patient agreed.
Case Report
Patient 1
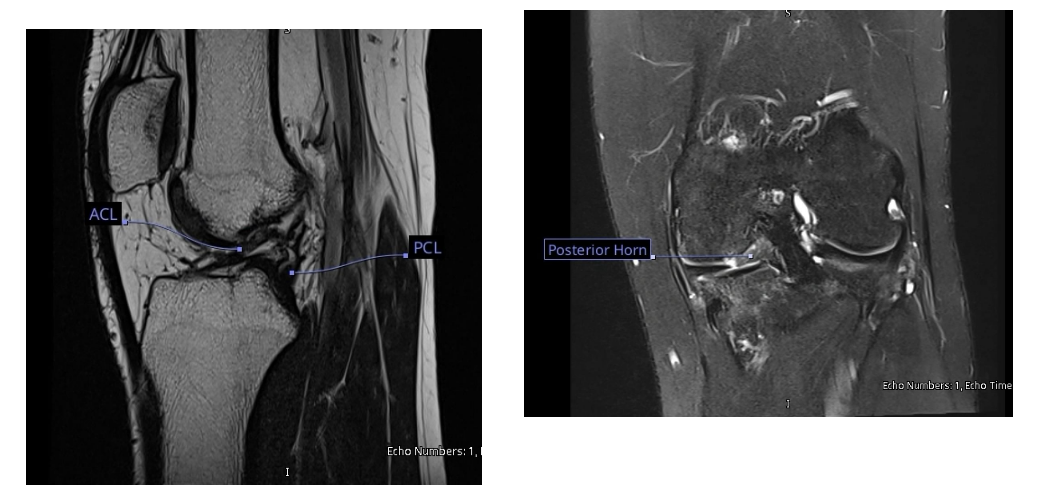
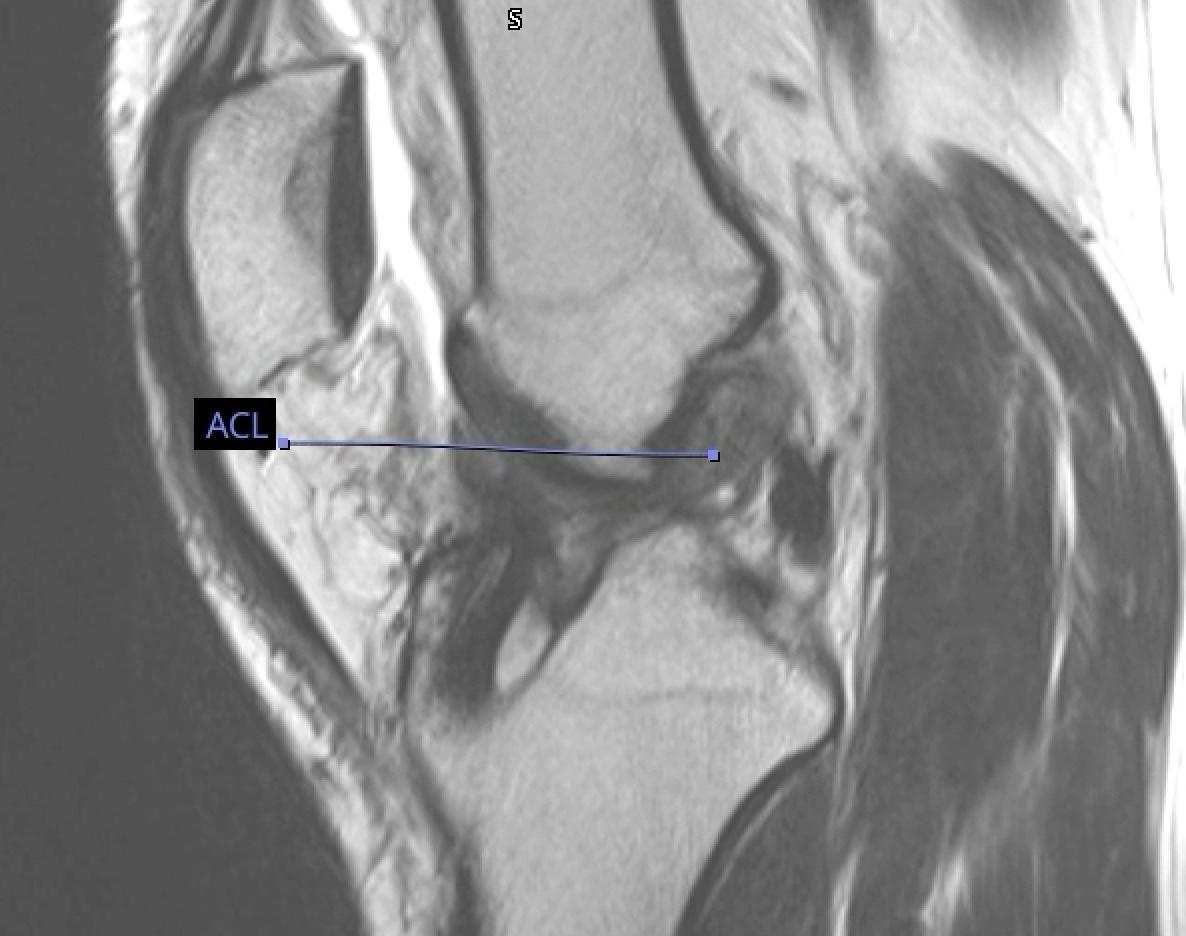
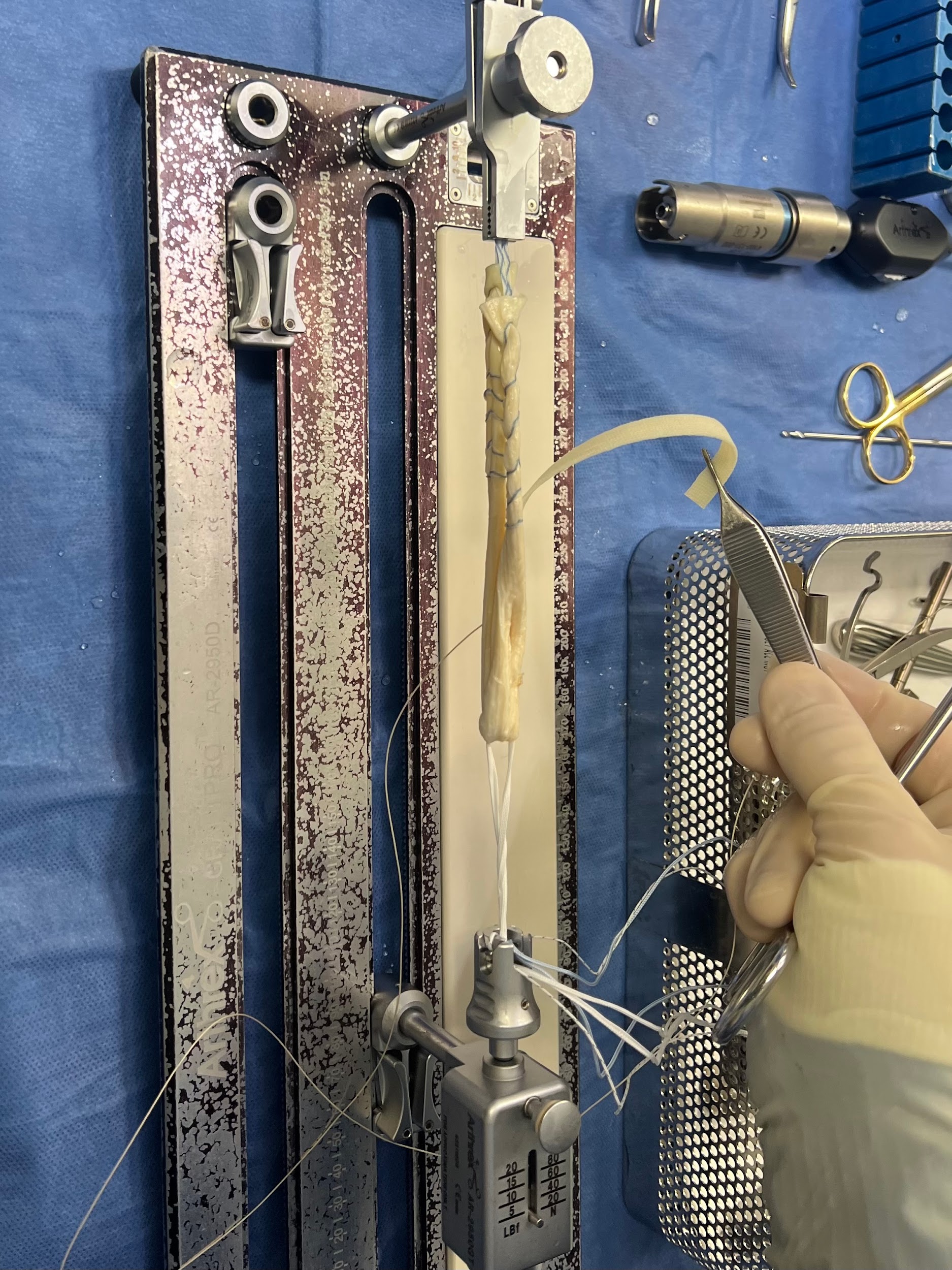
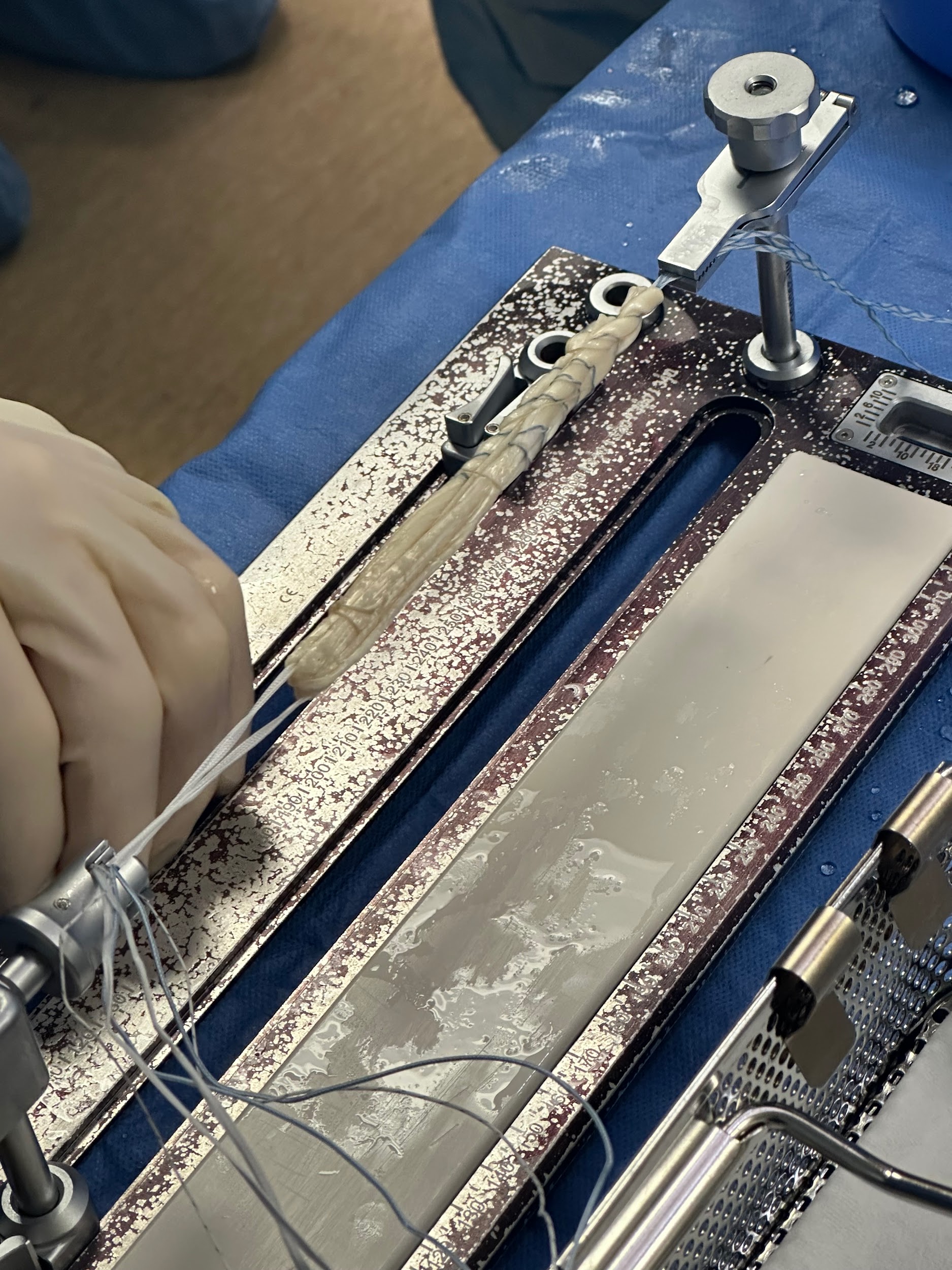
A healthy 22-year-old male presented with anterior left knee pain after noting a popping sensation that started a month prior after falling awkwardly and twisting his knee. Examination revealed near full range of motion with an increase in laxity on Lachman’s exam compared to the right. Magnetic resonance imaging (MRI) demonstrated a complete tear of the left ACL with a concomitant tear involving the posterior root of the medial meniscus (Fig. 1). He subsequently underwent primary left ACL reconstruction with TAT allograft and a partial medial meniscectomy. The choice of graft was left up to the patient and residual knee/harvest pain was the reason for choosing an allograft option instead of harvesting an autograft. This was performed in standard fashion with anterior medial and anterior lateral arthroscopic portals. The posterior root of the medial meniscus was stable with partial fraying present, therefore debridement with an arthroscopic shaver was utilized. The Arthrex system was used with a flip cutter for the femur (25 mm tunnel length) and a standard reamer for the tibia based on the size of the graft. The TAT allograft was then prepped in standard fashion and passed while the button was flipped on the femur. The knee was then cycled with tension applied to the sutures and an interference screw was inserted into the tibial tunnel in a retrograde fashion. Postoperatively, the patient was allowed to weight-bear right away in a hinged knee brace, limiting motion from full extension to 30 degrees of flexion for the first 2 weeks and progressively working up to full range of motion by 6 weeks. Two months later the patient’s pain had improved with appropriate weakness in the left knee (4/5 strength in knee flexion/extension) and a firm endpoint during Lachman’s test. Approximately seven months postoperatively, the patient returned, complaining of significant left knee pain after falling from a rebound attempt while playing basketball. Repeat MRI at this time demonstrated a complete mid substance tear of the left ACL graft and an associated lateral meniscus tear (Fig. 2). The patient underwent a revision left ACL reconstruction with an Artelon bio-scaffold for augmentation of a TAT allograft. The revision procedure was performed in standard fashion as described above during the index procedure in addition to interlocking an Artelon bio-scaffold within the stitching of the TAT allograft using monofilament absorbable suture (Figure 4, Figure 5). Postoperative mobilization and range of motion restrictions were employed the same as before following the index procedure. Physical therapy began shortly after surgery, and he slowly regained motion and strength in the left knee. Six weeks postoperatively, the patient was pain-free and doing well, consistently attending physical therapy appointments. On examination, there was a firm endpoint during Lachman’s test of the left knee and 4/5 strength in knee flexion and extension. At 24 months postoperatively, the patient admitted full strength (5/5 strength in knee flexion/extension) and range of motion (0-120 degrees) along with a stable left knee without symptoms of pain or instability with stairs or quick-cutting movements. He also regained the ability to run brace-free again without worry. No reoperations or complications were noted in the left knee following the revision procedure and the patient noted significant satisfaction with the ability to perform activities similar to his pre-injury level.
_of_the_left_knee_demonstrates_a_complete_tear_in_the_acl_with.png)


_prior_to_securin.jpg)

Patient 2
A healthy 29-year-old male presented with right knee pain that occurred two months prior while playing basketball. He noted right knee instability with a retained ability to ambulate, and an MRI confirmed a complete tear of the right ACL. The patient underwent primary right ACL reconstruction with a TAT allograft performed in standard fashion utilizing the technique described above for Patient 1. The choice of graft was left up to the patient and residual knee/harvest pain was the reason for choosing an allograft option instead of harvesting an autograft. Postoperatively he was placed in a hinged knee brace and allowed weightbearing as tolerated and unlocked from full extension to 30 degrees of flexion for the first 2 weeks and progressively working up to full range of motion by 6 weeks. Three weeks later, the patient’s pain had improved with appropriate weakness and therefore, formal physical therapy was started at that time. Twelve weeks postoperatively, the patient had improved right knee strength and motion with a firm endpoint during Lachman’s test. Two years postoperatively, the patient reported a repeat right knee injury after falling awkwardly. MRI at that time demonstrated a complete tear of the ACL graft (Fig. 3). After this diagnosis, the patient underwent a revision right ACL reconstruction with an Artelon bio-scaffold for augmentation of the TAT allograft (Figs. 4 and 5). This was performed in standard fashion as previously described in Patient 1. Postoperative mobilization and range of motion restrictions were employed the same as before following the index procedure. Physical therapy began shortly after surgery, and he slowly regained motion and strength in the right knee; by seven months postoperatively, he was working again and back to full activity. On exam, full range of motion (0-120 degrees) with a firm endpoint during Lachman’s test was noted along with 5/5 strength in knee flexion/extension. At 24 months postoperatively, the patient admitted he was back to near full strength and pain-free in his right knee. He noted full range of motion and back to pre-injury level of activity with the ability to run brace-free again without signs of pain or instability, even during quick-cutting movements. No reoperations or complications were noted in the right knee following the revision procedure and the patient noted significant satisfaction with the ability to play basketball again similar to his pre-injury level.
Discussion
ACL injuries are becoming more common in the United States nearing 200,000 cases annually with about 150,000 fixed surgically (Looney et al. 2020). Primary ACL reconstruction has become the gold standard treatment, especially in younger active patients, with results generally demonstrating high levels of return to activity and restoration of functional status (Grassi et al. 2017). Rates of revision vary widely among the literature as there are many techniques for ACL reconstruction, however, graft failure remains a major concern among surgeons. With graft failure in primary ACL reconstruction nearing 8%, revision ACL reconstruction has now become a more studied topic (Grassi et al. 2017). A recent systematic review reported that approximately 60% of the patients undergoing a revision ACL reconstruction will develop OA within six years, which is about two times the risk present with primary ACL reconstruction (Grassi et al. 2017). Therefore, studies aimed at graft augmentation in revision cases, as described in this case report, have become a point of focus in the literature. In our study, we sewed the Artelon graft between the folded TAT allograft (Figs. 4 and 5) to help resist rotational forces, since this has been a reported risk contributing to revision failure (Looney et al. 2020). A multicenter prospective longitudinal study termed the Multicenter ACL Revision Study (MARS) performed a multivariate analysis to determine the common modes of failure and clinical outcomes following ACL revision (Samitier et al. 2015; MARS Group et al. 2010). The MARS group reported modes of failure included 32% traumatic, 24% technical, 7% biologic, 37% combination, and less than 1% infection (Samitier et al. 2015; MARS Group et al. 2010). As previously described, clinical signs of failure are typically assessed by signs of instability, stiffness, or pain (Samitier et al. 2015). As for traumatic causes of failure, this can be secondary to trauma itself or aggressive rehab typically. Technical causes of failure have been reported to occur in 22-79% of ACL reconstruction failure cases and 70-80% of these failures are secondary to poor tibia or femoral tunnel placement (Samitier et al. 2015). When reconstructing the ACL, non-anatomic tunnel placement may increase stress placed on the graft and alter graft length and tension (Samitier et al. 2015). In fact, the MARS group reported that non-anatomical femoral tunnel placement was the most common technical error (80%) in their study with tibial tunnel placement (37%) being the next most common (Samitier et al. 2015; MARS Group et al. 2010). There is a paucity of literature regarding outcomes of synthetic augmentation in the setting of ACL primary and revision reconstruction. Theoretically, synthetic augmentation would aid in avoidance of donor site morbidity, as well as avoid complications with insufficient graft diameter, length, and strength while potentially assisting with rotational stability.
In this case report, we described two cases of younger male patients with a history of prior ACL reconstruction who underwent an ACL revision using a TAT allograft with an augmented Artelon bio-scaffold. The main finding in this report is that this procedure can be successful and provide positive outcomes for patients. Interestingly, there are no reports in the literature of patients undergoing a TAT allograft with augmented Artelon for revision ACL cases. Our case report is unique in two ways. First, the use of TAT allograft has previously been shown to be a viable alternative to bone-patellar-bone autografts and hamstring autografts, especially in revision cases or the non-athletic population (Issın et al. 2019). Second, the use of bioaugmentation, specifically Artelon, has not been well studied in the literature, however use of these products presents unique opportunities that may have the potential to improve patient outcomes via resisting graft forces during the healing process (Looney et al. 2020).
Bioaugmentation has been studied to enhance healing and decrease forces on ligament repairs (Myers et al. 2022). Artelon is a polyurethane urea bioaugmentation substance that has been used for a variety of purposes, including reinforcement of soft tissues, and can be used clinically for the treatment of osteoarthritis (Robinson and Muir 2011; Issın et al. 2019). However, there remains an overall scarcity in the literature regarding the use of Artelon in humans (Myers et al. 2022). To support the use in humans, Myers et al. performed a retrospective review on 32 patients who underwent medial collateral ligament (MCL) repair with an Artelon bio-scaffold, and they reported zero hypersensitivity reactions and non-inferior results compared with primary MCL repair (Myers et al. 2022). A study by Gersoff et al studied Artelon augmentation in patellar tendon repairs in dogs and noted improved earlier range of motion, less postoperative pain, and improved strength when compared to animals treated with tendon repair alone (Gersoff et al. 2019).
Potential concerns regarding Artelon use for soft tissue reconstruction include adverse foreign body reactions and graft failure. A study by Hussaini et al. reported zero foreign body reactions to Artelon graft with soft tissue reconstruction in foot and ankle surgeries (Hussaini et al. 2020). They also reported minor complications, with 5.5% developing cellulitis and 9.1% demonstrating delayed wound healing (Hussaini et al. 2020). In cases where non-human tissue is used as a graft or for augmentation, foreign body reactions are always a possibility. Studies with higher levels of evidence are warranted to investigate the incidence of these reactions and the true safety profile of Artelon. The primary limitations of this study include a small sample size of only two patients and two years of follow-up. With this small sample size and follow-up of only 2 years, it limits the generalizability of these findings when analyzing the general population. The large gap in follow-up data with both patients also lessens the reproducibility of these findings and the ability to apply this technique and their results to the general population. However, with 2-year follow-up data, this technique is safe and effective in restoring knee stability in these two patients at mid-term follow-up. Future studies should include larger cohorts analyzing measurable data on primary and revision ACL reconstruction utilizing allograft reconstruction with bio-scaffold augmentation. In addition, designing prospective studies comparing the differences between allograft with and without scaffold augmentation would be beneficial in analyzing the differences in stability and reoperation rates.
Conclusion
In conclusion, there is a paucity of literature regarding Artelon. This was a unique report of two cases which provided successful outcomes after the use of Artelon augmentation in revision ACL reconstruction. We hope this case report raises awareness for Artelon use in cruciate ligament reconstruction and more studies evaluate the longevity and safety of this product.