

Introduction
Total joint arthroplasty (TJA), including total knee arthroplasty (TKA) and total hip arthroplasty (THA) have experienced a surge in demand in recent years due to advances in surgical techniques and an aging population with degenerative joint disease (Kurtz, Ong, Schmier, et al. 2007). As the landscape of patients undergoing TJA becomes more medically diverse, the management of comorbidities and medications becomes increasingly important. The issue of perioperative anticoagulation management in patients on chronic anticoagulation is of utmost concern, as an estimated six million patients require perioperative anticoagulant management yearly (Zulkifly, Lip, and Lane 2018; Healey et al. 2012).
The role of mechanical and pharmaceutical anticoagulation in TJA is well-established, as these surgeries are historically high-risk for venous thromboembolism (VTE) occurrence (Kahn and Shivakumar 2020). With the advancement of surgical techniques, improvements in perioperative care, and development of safer and more efficacious drugs, the incidence of VTE has seen a significant decrease (Partridge et al. 2018; Chan et al. 2015). Prior studies have investigated the optimal perioperative anticoagulant regimen, with recent guidelines suggesting the use of aspirin and other anticoagulants over DOACs (Healey et al. 2012; Anderson et al. 2019; CRISTAL Study Group et al. 2022; Dunn, Spyropoulos, and Turpie 2007).
Since the establishment of DOACs as the preferred anticoagulation strategy (Class I for all) by the American Heart Association, DOACs have become the predominant anticoagulant in the outpatient setting, used for cardiovascular disease and increasingly used in orthopedic surgery patients in the postoperative setting (January et al. 2019; Hagedorn et al. 2023). Of this group of drugs, Factor Xa inhibitors (FXaI), like apixaban and rivaroxaban, are commonly used. While these drugs aim to prevent VTE formation, they pose significant bleeding risk to major surgery and therefore are regularly stopped prior to surgery. Appropriate perioperative management of these drugs is critical, as an interruption for too long may increase the risk of VTE, whereas early resumption may increase the risk of bleeding (Dunn, Spyropoulos, and Turpie 2007). However, despite the growing normalcy of joint reconstruction in patients on chronic FXaI, few studies have addressed the perioperative management of these drugs.
The PAUSE study investigated the safety of a standardized perioperative DOAC management strategy in patients on chronic anticoagulation. The study pioneered basic guidelines for start and stop intervals, finding that stopping medication 1 day preoperatively in low-bleeding risk procedures, and 2 days preoperatively in high bleeding-risk procedures, and resuming 1 day post-operatively in low-bleeding risk, and 2-3 days post-operatively in high-bleeding risk procedures was associated with low rates of major bleeding or thromboembolism (Douketis et al. 2019). Importantly, the PAUSE study found higher rates of major bleeding associated with high-bleeding risk procedures in the factor Xa inhibitor (apixaban and rivaroxaban) cohorts and suggested further study on this topic. Additionally, the study did not address the question of postoperative dosing.
In our study, we analyzed the cohort of interest from the PAUSE study, patients on chronic factor Xa inhibitors after TJA, a high-bleeding risk surgery, and utilized the recommended interruption and resumption intervals as suggested by the PAUSE study. Due to lack of expert consensus on the optimal dosing schedule of FXaI after total joint arthroplasty in patients on chronic anticoagulation, the aim of this retrospective cohort study is to investigate the risk of significant bleeding or VTE events with respect to resuming a full-dose or modified half-dose postoperative FXaI dosing protocol following total joint arthroplasty.
Methods
In this institutional review board-approved study, data was electronically collected from the Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI) (Hughes, Zheng, and Hallstrom 2019). Inclusion criteria were defined as adult patients who underwent primary, elective TKA or THA at a large, academic hospital between January 1st, 2014, and May 1st, 2021. All study patients were on either apixaban or rivaroxaban prior to TJA. Acceptable dosages for apixaban included 2.5 mg and 5 mg twice daily. Included dosages for rivaroxaban were 10 mg and 20 mg once daily. Patients were excluded from the study if they were on additional anticoagulants, underwent bilateral TJA, or had a known hematological disorder that increased their risk of perioperative bleeding or coagulopathy. To account for the potential impact of tranexamic acid on the different dosing outcomes, its use was consistent between the two groups and documented in the MARCQI database for comparison. All surgeries were performed by one of two fellowship trained arthroplasty surgeons.
Patient assignment to the postoperative dosing regimen (half-dose or full-dose) was determined by the established protocols of the individual surgeons performing the surgeries. Specifically, some surgeons consistently used one protocol for all their patients, while others used a different protocol. This ensured that dosing regimen selection was not influenced by patient characteristics or surgeon preference, thus reducing selection bias risk.
The primary outcome of this study was the occurrence of significant bleeding within six months postoperatively. Significant bleeding events were defined as gastrointestinal bleeds, hemarthrosis, hematuria, and other bleeding, which included major oral bleeding, intracranial bleeding, and completely blood-soaked wound dressings. Hemarthrosis was defined as the presence of joint swelling and/or drainage that soaked through the wound dressing. Minor wound bleeding, which was defined as blood on the wound dressings that did not soak through the dressing, was noted, however, this finding was considered a standard postoperative change and not defined as a significant bleeding event. A secondary outcome assessed in this study was the occurrence of VTE events, including pulmonary embolism (PE), deep vein thrombosis (DVT), and strokes, within six months postoperatively.
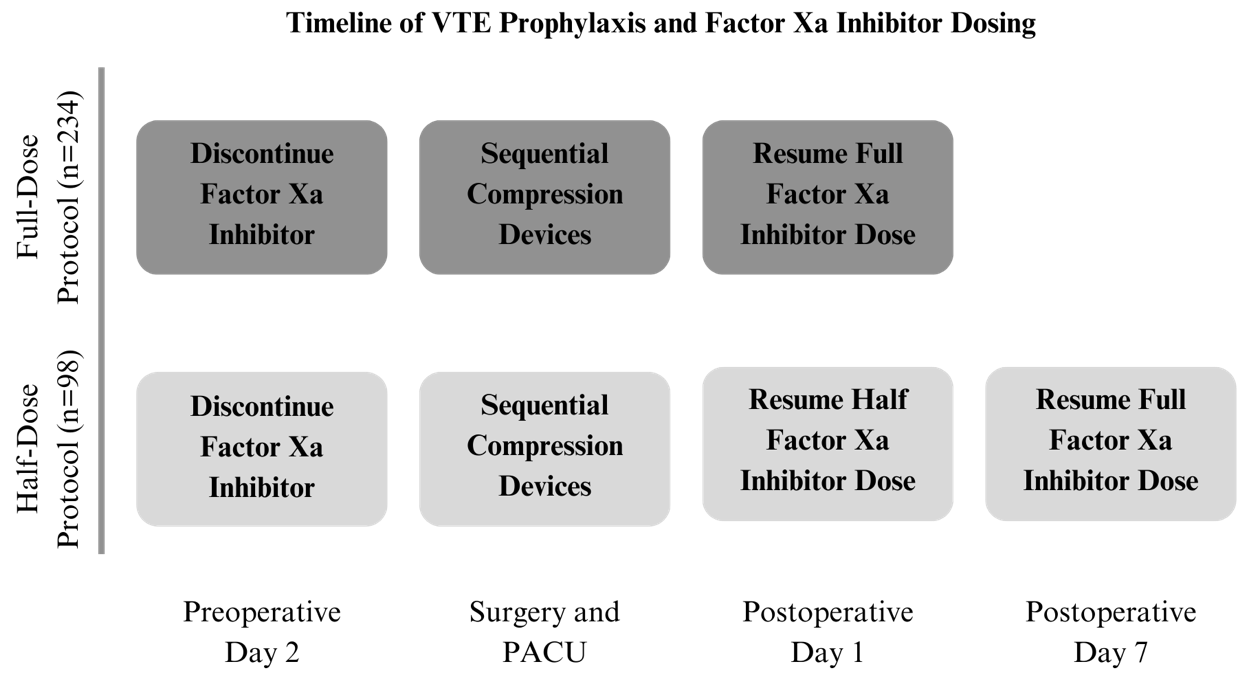
Patients were divided into two cohorts based on the postoperative dosing schedule of the DOAC (Fig. 1). All patients in this study were instructed to discontinue their DOAC 2-3 days prior to surgery. Patients in group A (half-dose group) were instructed to resume their DOAC at a half-dose on the morning of post-operative day (POD) 1 and continue the half-dose DOAC until POD 6. On POD 7, patients in group A resumed the full-dose DOAC. Patients in group B (full-dose group) were instructed to resume their DOAC on the morning of POD 1. During the postoperative period of their hospital stay, all patients received VTE prophylaxis with sequential compression devices and daily physical and occupational therapy.

Of the 10,243 patients queried from the MARCQI database, 332 patients met the inclusion criteria and were included in this study. Ninety-eight patients were assigned to group A and 234 were assigned to group B. Patient demographics were collected and included age, sex, race, ethnicity, body mass index (BMI), smoking status, weekly alcohol intake, diabetes mellitus diagnosis, and American Society of Anesthesiology (ASA) score. The occurrence of significant bleeding events and thromboembolic events were collected for each patient.
Data analyses
Descriptive statistics were completed for each variable. Variables were first investigated using univariate analyses in the form of Student’s t-tests and Chi-square analyses. The primary statistical analysis conducted was multivariable logistic regression analysis to assess the risk of each covariate on significant bleeding and thromboembolic event risks. Adjusted odds ratios with 95% confidence intervals were reported. The statistical significance of covariates from regression analysis was defined as P<0.05. Data was analyzed using Statistical Package for the Social Sciences statistical software (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, New York: IBM Corp).
Results
There was no significant difference in patient age, sex, BMI, ASA score, smoking status, or weekly alcohol consumption between the two cohorts (Table 1). Additionally, there was no difference in patients with a history of DVT/PE between the two cohorts. The mean age of patients in the half-dose group was 72 years (range, 48 to 92 years, N = 98) and the mean age of patients in the full-dose group was 73 years (range, 43 to 95, N = 234, P=0.279). The half-dose group had 8.2% (N = 8) of patients who were current smokers, while the full-dose group only had 2.6% (N = 6) of patients who were current smokers. While smoking status (P=0.057) and ASA score (P=0.068) did not reach statistical significance, these variables were included in subsequent regression analysis.
The overall study incidence of significant bleeding events was 6.9% (N = 23) and the overall incidence of thromboembolic events was 1.5% (N = 6). The incidence of significant bleeding events in the half-dose cohort was 6.1% (N = 6) and 7.3% (N = 17) in the full-dose cohort (P=0.708) (Table 2). For each of the sub-types of significant bleeding event, there was no statistically significant difference in the incidence of gastrointestinal bleeds, hemarthrosis, hematuria, or miscellaneous major bleeding. For thromboembolic events, the half-dose group had an incidence of 2.0% (N = 2) and the full-dose group had an incidence of 1.3% (N = 3) (P=0.605). There were no strokes in the half-dose group or the full-dose group.
Multivariable logistic regression analysis was corrected for patient age, sex, smoking status, and ASA number (Table 3). The DOAC dosing schedule was not predictive of significant bleeding events (adjusted Odds Ratio (aOR)=0.66, 95% Confidence Interval (CI) [0.24-1.83], P=0.424). Similarly, the DOAC dosing schedule was not predictive of thromboembolic events (aOR=1.33, 95%CI [0.19-9.38], P =0.774).
Discussion
The findings of this retrospective study on Factor Xa inhibitor (FXaI) dosing in postoperative joint replacement patients provide important insights into the perioperative management of patients on chronic factor Xa inhibitor therapy. With a cohort of 332 patients, the study aimed to investigate the relationship between two distinct dosing regimens, full-dose and half-dose factor Xa inhibitors, and their impact on bleeding and VTE events after TJA. The results revealed that the incidence of significant bleeding events in the half-dose cohort was 6.1% (N = 6) and 7.3% (N = 17) in the full-dose cohort, with no statistically significant difference observed (P=0.708) (Table 2). Similarly, VTE events were documented in 2.0% (N = 2) of patients in the half-dose group and 1.3% (N = 3) in the full-dose group, with no statistical significance observed (P=0.605). Future prospective studies with larger sample sizes are needed to further investigate these observations and provide more definitive conclusions.
For patients at high-risk for VTE on chronic anticoagulation, resuming postoperative anticoagulation remains critical. However, resuming anticoagulant therapy after surgery requires intricate care, as starting anticoagulation too early may increase the risk of bleeding, while starting too late may increase the risk of VTE (Dunn, Spyropoulos, and Turpie 2007). The PAUSE study attempted to fill this knowledge gap by creating a schedule of DOAC interruption and resumption for elective surgery based on their prospective study. This study recommended stopping DOAC 1 day before and resuming 1 day after low-bleeding risk surgery and stopping DOAC 2 days before and resuming 2-3 days after high-bleeding risk surgery (January et al. 2019). Of note, the PAUSE study found higher rates of major bleeding associated with high-bleeding risk procedures in the factor Xa inhibitor (apixaban and rivaroxaban) cohorts and suggested further study on this topic.
Our study analyzed the cohort of interest from the PAUSE study, patients on chronic factor Xa inhibitors after TJA, a high-bleeding risk surgery, and utilized the recommended interruption and resumption intervals as suggested by the PAUSE study. We analyzed cohorts by resumption dosing regimen, full-dose and half-dose, and found no statistically significant difference in the rates of VTE or bleeding. The results in combination with findings from prior literature imply that a reduction in the dose of factor Xa inhibitors postoperatively may be a viable approach to minimize bleeding complications without exposing patients to an elevated risk of VTE. However, it is equally reasonable to consider that the full-dose regimen might be preferred for medical reasons, particularly given the lack of statistically significant differences in postoperative complications. Therefore, the data supports that either dosing regimen could be appropriate, and the choice may be left to the clinician’s discretion based on individual patient factors and clinical judgment.
The comparable rates of bleeding and VTE events between the full-dose and half-dose regimens suggest that a more conservative, half-dose approach may provide a safer alternative without compromising the effectiveness of VTE prevention. While pharmaceutical anticoagulation remains paramount, other advances in perioperative care including improvements in surgical technique, greater compliance with mechanical thromboprophylaxis, shorter operative times, greater use of regional anesthesia, more effective analgesia, faster postoperative mobilization, increased day-case procedures, and shorter length of stay have contributed to significantly decreased rates of symptomatic VTE and mortality over the last few decades (Kahn and Shivakumar 2020; Partridge et al. 2018; Xu et al. 2019). Postoperative bleeding remains a serious concern in TJA, as hematoma formation can lead to joint infection with disastrous long-term health and financial consequences (Kwong et al. 2012; Muntz et al. 2004; Vera-Llonch, Hagiwara, and Oster 2006).
There are numerous factors outside of pharmacological thromboprophylaxis that contribute to VTE, and it is possible that many patients are being exposed to more anticoagulation than is necessary without additional clinical benefit (Chan et al. 2015). In a systematic review of fourteen phase III randomized controlled trials of VTE prevention with various anticoagulants, Chan et al. found low rates of symptomatic VTE and mortality (0.99% and 0.26%, respectively) and relatively high rates (3.44%) of clinically important bleeding, indicating that postoperative anticoagulation may have a higher adverse effect of bleeding than previously anticipated.
While our retrospective study provides valuable insights into FXaI management after TKA, it is essential to acknowledge certain limitations that may influence the generalizability and interpretation of our findings. Firstly, the retrospective nature of the study introduces inherent biases, such as selection bias and information bias, as we rely on existing medical records. This is somewhat mitigated using data monitored by paid nurse data abstractors (Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI)) (Hughes, Zheng, and Hallstrom 2019). Additionally, the study design lacks randomization, which may affect the internal validity of our comparisons between patients in each dosing group, half-dose and full-dose. Furthermore, lack of dosing data, including reason for medication, past medical history, and variations in patient adherence to the prescribed dosage can impact the robustness of our results. Despite these limitations, our study contributes valuable real-world evidence to the existing literature on factor Xa inhibitor therapy post-total knee arthroplasty.
The clinical relevance of these findings cannot be overstated. Joint replacement surgery is commonly performed in patients with advanced age and multiple comorbidities, making the balance between VTE prophylaxis and postoperative bleeding a critical concern. The results of this study offer a promising avenue for the optimization of anticoagulation management in joint replacement patients. This research provides orthopedic surgeons and healthcare providers with a potentially safer and more tailored approach to anticoagulation by demonstrating that the half-dose regimen is as effective as the full-dose regimen in preventing VTE.
Conclusion
The findings of this study demonstrated no statistically significant difference in occurrence of significant bleeding or VTE events between patients resuming their preoperative factor Xa Inhibitor therapy at a full-dose or modified 7-day half-dose protocol. Subsequently, when adjusted for patient demographics, there was no statistically significant relationship between postoperative bleeding and VTE events with respect to the postoperative DOAC dosing regimen. In conclusion, these findings underscore the need for further prospective trials and clinical guidelines that incorporate half-dose factor Xa inhibitor regimens as a potentially safer and equally effective alternative to anticoagulation management following total joint arthroplasty, ultimately benefitting a growing and more diverse patient population.