








Introduction
Prior to COVID19, the health care system faced significant challenges as we moved away from fee for service to more risk-based payment models. There was growing pressure to contain costs even in the context of a growing economy because of declining reimbursements. In the post-COVID19 era with a struggling economy, there will be even greater cost containment pressures to create margin to overcome lost revenue. One area of opportunity is with surgical supplies, especially for high volume, high cost procedures such as total knee replacements. Current use of preference cards generated by electronic medical records (EMRs) while useful in initial onboarding of basic surgical supplies for a new surgeon is a static document. As trends and techniques change, rarely does the EMR generated preference card reflect those changes leading staff to open and waste unnecessary surgical supplies. Updating the data requires significant work to understand and collect the new information which is difficult to do as an ongoing process (Harvey, Smith, and Curlin 2017). With staff cross trained across numerous specialties, they are forced to memorize thousands of instruments, dozens of workflows across dozens of surgeons and surgeries. This process has not changed in decades despite the significant growth in new surgical procedures, technical difficulty, implants, and instruments. The influence and support of outside personnel such as medical device representatives has been critical in helping operating rooms maintain proficiency because of the lack of internal tools and resources. These traditional manual workflows create a lack of standardization, lack of knowledge transfer, unnecessary utilization, inefficiencies, and potential use of non-value added implants and instruments (Ikuma et al. 2020). If the surgical preference card can be clinically integrated with the surgical procedure, costs and inefficiencies can improve. Research has shown this novel technology improved surgeon time spent performing surgery (“cut to close”) by up to 20% (Ahmad et al. 2018). This was accomplished by improved circulator and scrub tech performance when utilizing this technology compared to traditionally managed surgeries using EMR generated preference cards and medical device representative assistance (Ahmad et al. 2018).
How does novel technology to digitize surgical processes to create a single integrated dynamic digital surgical preference card and digital technique guide impact surgical supply costs in knee replacement surgeries compared to traditional non automated knee replacement surgery workflows using medical device representatives?
Materials and Methods
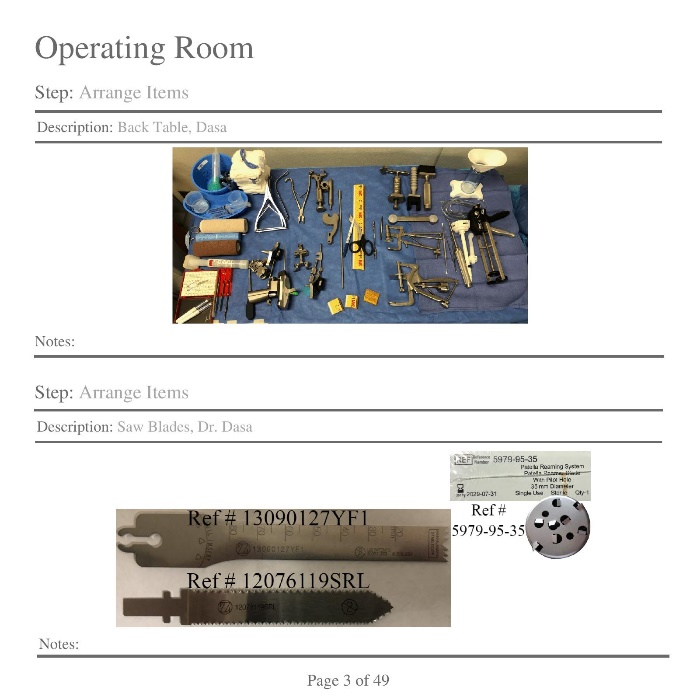
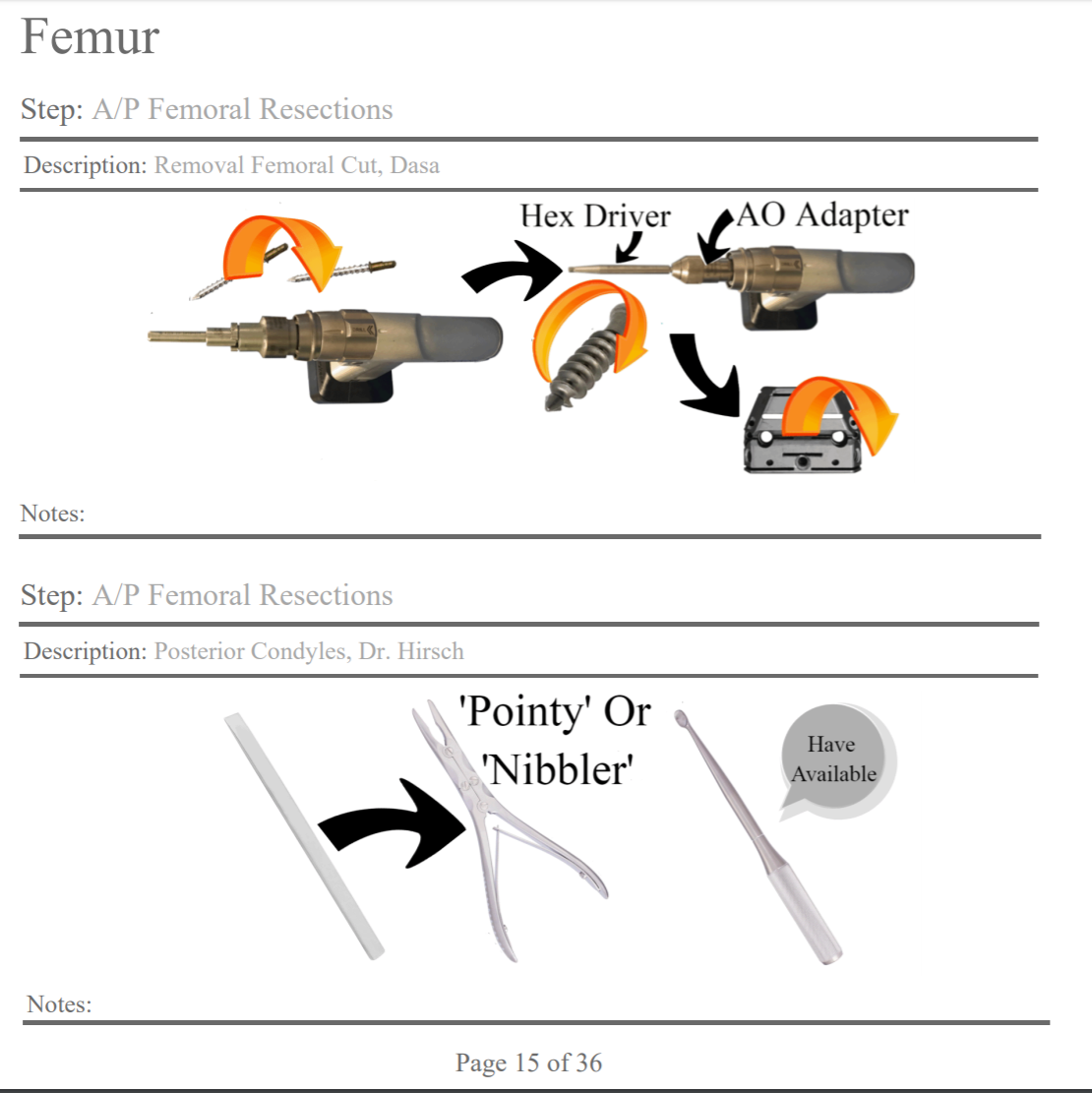
A novel innovative patented technology (SIGHT Medical, Alexandria LA) was created to digitize surgical processes and interface with hospital data systems such as EPIC and Lawson (Electronic Resource Planning software (ERP)) within the Ochsner Health System (New Orleans, LA). The automated technology was simultaneously deployed across three fellowship trained surgeons (CM, VD, GC) at three different hospitals over a course of 3 years (2017-2019) in patients greater than 60 years old undergoing knee replacement surgery. The technology enables the OR staff to manage the technical support during surgery, implant inventory, instruments, surgical supplies, and additional workflows and processes such as room set up (Figure 1 a and 1b). Additionally, the technology was integrated with supply chain software (ERP- Lawson) which allowed automated implant stock and procurement. The data was updated and managed in real time by all stakeholders creating a dynamic and up to date tool that was an adjunct to the standard EMR based surgical preference cards and OR workflows.


For automated surgeries (patient age >60 yo), the technology in addition to EMR-based surgical preference cards without the presence of a medical device representative was used to manage technical support during surgery, implant inventory, instruments, surgical supplies, and additional workflows such as room set up (Figure 2a-d). Cemented knee replacement implant systems were onboarded by the vendor (Zimmer Biomet NexGen TKA Warsaw, IN; United Orthopedics U2 TKA, Irvine CA) into the technology platform prior to the first surgery. The surgeon’s surgical preferences and technique were digitized in the platform by the medical device representative and OR staff prior to the first surgery. The medical device representative, using a vendor portal, monitored and managed these processes remotely or in person if needed. The digital guide was displayed on a heads-up computer screen and voice controlled by the scrub tech who wore a wireless microphone (Figure 3).




_managing_the_digital_technique_g.jpeg)
For traditional surgeries (patient age <60 yo), standard EMR based surgical preference cards with the presence of a medical device representative were used to manage technical support during surgery, implant inventory, instruments, surgical supplies, and additional workflows such as room set up. Cemented implants were used by GC and CM (Zimmer Biomet Persona TKA Warsaw, IN and Stryker Triathlon TKA, Mahwah, NJ) and were considered premium implants for this younger patient cohort. VD used all uncemented implants (Zimmer Biomet Persona TKA Warsaw, IN) without patella resurfacing for this same younger patient cohort.
Medical Surgical (med/surg) supplies and billable medical supplies were captured by the OR staff using standard hospital EMR and materials management workflows. Supplies are generally grouped into 2 categories, routine and non-routine. Routine or Med/surg supplies are bundled with the procedure and include items such as sponges, towels, drapes, and electrodes. Non routine or Billable Medical supplies are items which can be potentially reimbursable by various insurance companies and include items like shavers and special bovie cautery (n.d.). Length of stay was captured in the EMR. Aggregated deidentified outcome measures of surgical supply costs, length of stay, and number of cases were analyzed using the Ochsner Health System data analytics platform (Tableau, Seattle, WA).
Results:
A total of 1023 knee replacement surgeries were reviewed within the Ochsner Health system over the 3-year period (Table 1). There were 560 traditional surgeries and 463 automated surgeries. Automated surgeries had an average of $479/surgery in med/surg supply costs compared to $557/surgery for traditional surgeries. There was an average $2,444/surgery in billable medical supply costs in automated surgeries and $4,660/surgery for traditional surgeries. Average length of stay for automated surgery patients was 1.18 days and 1.08 days for the traditional surgery patients. The Ochsner health system length of stay average for all surgeons and patients in traditional knee replacement surgeries was 1.53 days over the same 3-year period. No automated surgeries required in person medical device representative support however surgeons requested the representative to be available for intra operative support for 5 surgeries due to the complexity of the surgery. The medical device representative was within the hospital but not in the operating room.

CM had 2.5% variation of med/surg supply costs over 3 years in automated surgeries and 66% variation in traditional surgeries. GC had 19% variation in automated surgeries of med surg/surg supply costs compared to 36% in traditional surgeries. VD had 41% variation in med/surg supply costs in automated surgeries compared to 46% in traditional surgeries (Graph 1a).
.png)
CM had 27% variation in billable medical supply costs in the automated group compared to 5% variation in the traditional group. GC had 5% variation in billable medical supply costs in the automated group compared to 18% in the traditional group. VD had 18% variation in billable medical supply costs in the automated group compared to 15% in the traditional group (Graph 1b).
.png)
Discussion:
By digitizing surgical processes and creating tools for collaboration, hospitals can enable their staff to better manage resources and reduce waste. The data from this retrospective study shows $78 in average cost savings in med/surg supply costs and $2216 in billable medical supply average cost savings by automating many of the surgical workflows and processes. Costs varied widely across categories, surgeons, and hospitals. The smallest amount of year over year variation was seen in surgeries using the technology for med/surg supply costs and the greatest amount of variation was seen in traditional surgery med/surg supply costs. The only area where costs were increased with automated surgeries was with surgeon VD med/surg supply costs who did not use cement in traditional surgeries but did use cement for automated surgeries which increased med/surg costs for those surgeries. The technology may have helped the OR staff more clearly understand the surgeon’s preferences in real time rather than using more static EMR based preference cards. The technology is more closely linked with the details and nuances of each surgeon’s preferences and behavior and is actively curated by the surgeon and the OR staff thus being more clinically relevant than established older platforms and workflows. Because the preference card is integrated into the actual surgical workflow, stakeholders are incentivized to maintain its accuracy and fidelity. Additionally, the knowledge transfer between stakeholders is dynamic, reducing the need to have dedicated teams or senior staff to provide surgical support.
The technology changed the role of the traditional medical device representative model, allowing the OR staff to manage and make more independent standardized decisions with the support of the technology. The medical device representative was an integral component of the hospital team but utilized in a much different context. They were able to remotely monitor inventory, train hospital staff, facilitate movement of items between hospitals, help manage surgical data within the technology, and serve as backup support. They interfaced with the surgeons and OR staff at regular intervals to monitor quality and efficiency and facilitated improvements and deployment of new instruments and new implant technology. Because all stakeholders collaborated on a surgeon specific digital guide, the trust and accuracy of the information was continually enhanced. The feedback loop and the ability for all stakeholders to collaborate using a foundational technology allowed the staff to feel empowered to make independent decisions without needing traditional in person outside support. The medical device representative was in constant communication and available when needed both remotely and in person.
The technology provided the OR staff with a visual real time reference of supplies and steps of the surgery to allow junior most scrub techs to manage a knee replacement surgery with autonomy and remain multiple steps ahead of the surgeon creating improved efficiency and quality (Figure 2a-d) (Ahmad et al. 2018). It was deployed in cases using a specific implant which was used in lower demand older patients based on surgeon consensus. Despite the older patient cohort, length of stay between the 2 groups was not clinically significant. One would expect a much longer length of stay difference in the older patient cohort. In addition to many other factors, research has shown that length of stay is correlated with surgical time (Ahmad et al. 2018). By improving surgical efficiency to shorten surgical times, there is potential to reduce length of stay which may explain why the older patient cohort had better than expected length of stay than the health system average.
Limitations of this study include lack of in-depth demographic and clinical data to ensure the traditional patient cohort was similar to the automated cohort except for age. OR times were not available in this cost data set and generally have poor accuracy at the minute level thus would not be as discriminatory as needed. This analysis will need to be done as a prospective time study. Additional prospective research on the impact of additional implant selections and surgeons across a wider range of patient cohorts is needed to validate these pilot findings.
