

Introduction
Chronic lower back pain (CLBP) is a common finding with significant health care costs and economic implications (Katz 2006). The treatment of CLBP can be a frustrating process for the patient, clinicians, and third-party payers who all have an interest in successfully treating CLBP at the lowest possible cost (Haldeman and Dagenais 2008). CLBP is first treated conservatively with combinations of pharmaceuticals, physical therapies (like massage, physiotherapy, exercise, etc.), and psychological therapies (Savigny et al. 2009). If unsuccessful, more invasive options like steroid injections, nerve blocks, radiofrequency ablation (RFA), and surgery can be utilized (Leggett et al. 2014).
Zygapophyseal (facet) joints are a common source of CLBP (Manchikanti et al. 2020). Interventional treatment options aim at addressing the facet joints or their associated sensory nerve innervation. RFAs, an increasingly used treatment, target the two medial branches of the primary dorsal rami at and above the pathological facet joint level to block the sensory nerve impulses traveling to the central nervous system. The RFA functions by creating a high-frequency electrical current at the tip of a needle, burning a small lesion within the sensory nerve to disrupt the signal pathway (Akgul and Akgun 2022; Moussa, Khedr, and Elsawy 2020). While a commonly used treatment, the evidence for RFA use is mixed (Leggett et al. 2014; Akgul and Akgun 2022; Moussa, Khedr, and Elsawy 2020; Maas et al. 2015; van Wijk et al. 2005).
Opposite of thermal damage from RFAs, cryoneurolysis is the application of extreme cold to damage nerve tissue, disrupting sensory signaling from the periphery to the central nervous system. Modern advances in hand-held cyroneurolysis devices and the widespread use of ultrasound or fluoroscopic guidance allow for targeted treatment with the ice balls formed at the needle tip from the devices. The induced Wallerian degeneration does not damage the epineurium, perineurium, muscles, or vessels, creating a reversible secondary axonotmesis on the Sunderland Classification Scale (Suputtitada et al. 2023). Cryoneurolysis has been successfully used in perioperative scenarios for acute pain management in thoracotomies, mastectomies, total knee arthroplasties, and shoulder arthroplasties (Biel et al. 2023; Ilfeld and Finneran 2020). Cryoneurolysis has more recently been used to address chronic pain conditions like knee pain, temporomandibular disorders, neuropathic pain, and phantom limb pain (Biel et al. 2023). Although advancements in cryoneurolysis have allowed its use in acute and chronic pain, its use to address facet related CLBP is a novel idea.
The Case
A 67-year-old female presented to the clinic with three years of lower back pain with some radiation into the glutes and upper hamstrings. Patient noted having mild weakness in both extremities and morning lower back stiffness, but she denied any leg numbness and tingling. Her pain had previously improved with rest, physical therapy, and modalities. The pain was worse with extension, rotation, and twisting as well as with gardening. The pain was described as sometimes sharp and sometimes an achy, dull pain. Pain was rated as a seven out of ten. The patient did not elicit warning signs like bowel or bladder changes, changes in balance, recent history of falls, or saddle anesthesia.
She had previously completed PT, used over-the-counter medications like Tylenol, and had received trigger point injections. She had not had any interventional treatments like manipulations, radiofrequency ablations, or surgery and personal history was negative for cancer.
Physical exam showed mild thoracolumbar scoliosis and relative mild tenderness to palpation of the bilateral L4-S1 spine and thoracic spine. Patient had decreased range of motion in lumbar extension, rotation, and side-bending secondary to pain. No abnormalities were seen in flexion. Patient had 4+ strength throughout without focal weakness, normal L2-S1 dermatomes, and 1+ bilateral lower extremity reflexes. Positive facet maneuvers were noted bilaterally. Patient had negative bilateral straight leg raises, log roll, FADIR, and FABER testing. Gait was antalgic.
Patient’s radiographs showed degenerative changes at L4-S1 with mild scoliosis in the thoracolumbar spine. Her MRI showed degenerative changes at the lumbar spine, worse in the L4 to S1 region.
Treatment options of medications, physical therapy, and interventional options were discussed with the patient. She subsequently went to a neurosurgeon to discuss the possibility of surgical correction of the scoliosis. It was determined she had degenerative scoliosis and should be managed conservatively.
She returned to our clinic four months later with no change in her symptoms. In the interim, she had been referred by her PCP to a chiropractor without benefit and had declined medication management offered from a pain clinic. At this visit, she agreed to restarting physical therapy and undergoing diagnostic medial branch blocks. Two subsequent bilateral L4-S1 medial branch lidocaine blocks each gave 100% immediate symptomatic relief. Radiofrequency ablations were discussed at a follow-up appointment, but she endorsed concern for any potential low back weakness from the RFAs and asked about an alterative. After we discussed the risks and benefits, she elected to pursue cryoneurolysis of the medial branches of the dorsal roots of L4-S1 bilaterally.
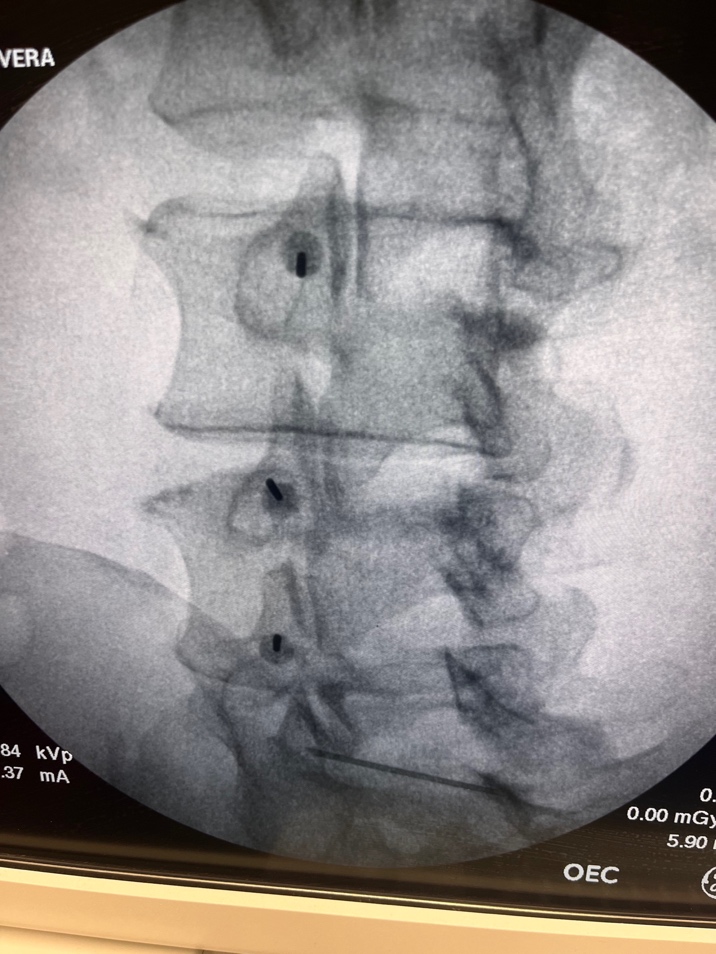
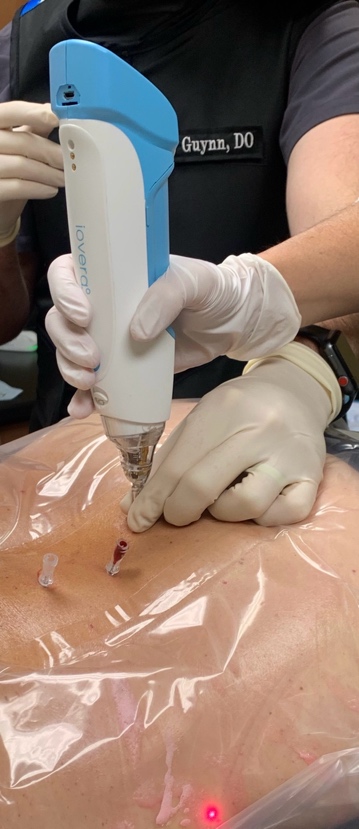
Subsequently, bilateral L4-S1 medial branch cyroneurolysis was performed under Fluoroscopic guidance (See Figure 1 &2). Using the fluoroscope and typical spine injection sterile cleaning protocol with hibiclens and draping and after anesthesia with 1% lidocaine, 18-Gauge, 6.35 cm echogenic introducer needles were placed at the L5 dorsal rami on the sacrum and L3,L4, as well as L5 medial branch locations on the pedicle bilaterally. 1 cc of 1% preservative free lidocaine was administered around the nerves followed by two rounds of cryoneurolysis administered by the iovera device. Patient noted immediate relief in facetogenic pain.


At a three week follow up, her original pain of score of 7 was report to be 0 at rest and 1 with movement which she described as muscular pain. She reported that 100% of the deep pain with extension, rotation, and side-bending was gone. Within one week of the procedure, she was able to get into her yard and do gardening. She started physical therapy after the treatment to address weak glute muscles and her posterior chain with the therapist and returned at six month follow up with continued pain relief.
Discussion
Cryoneurolysis is a proven modality for both acute and chronic pain in peripheral nerves involved in joint pain and neuropathic pain.
As with any interventional treatment, there are risks in the use of cryoneurolysis. Nonspecific risks include bleeding, bruising, and rarely infection. Other risks include distress to the patient secondary to pain during the procedure and damage to surrounding tissue if the cryoprobe is moved away from the nerve during the application. Additional risks include hyper and hypo-pigmentation of the skin and alopecia at the site of the injection. Some devices include a warm at the skin level to minimize risk of skin and hair damage (Ilfeld and Finneran 2020; Ilfeld, Gabriel, and Trescot 2017). Though there are rare reports of transient neuritis, there are no published cases of permanent nerve injury or neuroma (Biel et al. 2023; Ilfeld and Finneran 2020; Ilfeld, Gabriel, and Trescot 2017). Lastly, there does not appear to be negative effects of multiple cryoneurolysis applications following full axonal recovery in the same location (Ilfeld, Gabriel, and Trescot 2017). In the case, the patient did not experience any of the highlighted risks other than minimal bleeding at the injection site.
Cryoneurolysis has relative contraindications like other percutaneous needle treatments including bleeding disorders, current infection, and immunosuppression. Specific contraindications include Raynaud’s disease, cold urticaria, cryoglobulinemia, cryofibrinogenemia, and paroxysmal cold hemoglobinuria (Biel et al. 2023; Ilfeld and Finneran 2020; Ilfeld, Gabriel, and Trescot 2017). In this case, none of the contraindications were present.
While further research is needed to address the use of cyroneurolysis, there are some additional benefits seen when compared to other pain treatments. One, published literature suggests a safety level superior to traditional local anesthetic peripheral nerve blocks (Ilfeld, Gabriel, and Trescot 2017). Second, sedation is not required like in some RFA procedures. This takes away the additional anesthesia risk and reduces cost for pain relief (Ilfeld and Finneran 2020). Third, this has the potential to provide another avenue of pain management avoiding the use of opioid medications. The third reason has significance in our case, as the patient declined opioid management from a pain clinic prior to the second office visit. She, like many patients and clinicians, avoid opioid prescription and use whenever possible.
While there is concern that regeneration of the Axon requires regular follow up treatments, this provides a possible advantage over radiofrequency ablations. RFAs are also a reversable nerve injury and often necessitate repeated ablation procedures (Choi et al. 2016). It is seen in radiofrequency ablations that collateral sprouting diminishes returns with retreatment. The lack of collateral sprouting in cryoneurolysis may provide sustained efficacy with each repeated freeze. Further investigation is needed to see what the long-term outcome is of single cryoneurolysis and subsequent freezes.
While pain was successfully relieved in this patient, one limitation to broad use of cryoneurolysis in the treatment of CLBP is the length of the needle. The patient was relatively thin, allowing the needle to penetrate deep enough to freeze the medial branches of the nerve. Even in the lean patient, the needle was at its max depth. A longer, yet still effective cryoprobe needle would need to be made to treat patients with average or larger body habitus.
Overall, this case presents a novel approach to CLBP with some questions left unanswered. First, it is not known the long-term efficacy of cyroneurolysis in CLBP. Second, though results have been positive, there is a lack of large-scale studies using cryoneuolysis to understand its effectiveness and complication profile. Third, there needs to be effective lengthening of the cryoprobe to treat the medial branches of the dorsal root ganglia in a broad spectrum of patient body habitus.
Conclusion
Cryoneurolysis was successfully used as a novel approach to facet mediated CLBP in a 67 year old female with concerns about other interventional options. Significant reduction in pain was experienced immediately and office visits at three weeks and six months post treatment. This case sparks further exploration in the use of cyroneurolysis and investigation into its chronic efficacy.