

Introduction
Robotic-assisted total knee arthroplasty (raTKA) has been increasingly utilized in recent years, with reports suggesting improved accuracy and reproducibility compared to conventional TKA, as well as reduced damage to surrounding bone and soft tissue (Rossi et al. 2023; Hampp et al. 2019; Kayani et al. 2019). Researchers have begun to explore the intra-operative data that can be collected during raTKA, particularly implant position, limb alignment, and flexion-extension gap balance. Examination of the relationships between these intra-operative factors and outcomes have fueled hypotheses that suboptimal mechanical axis restoration or soft tissue balancing may negatively impact patient recovery and reduce prosthesis stability and implant longevity (Saber, Marappa-Ganeshan, and Mabrouk 2023; Lonner et al. 2023).
The majority of research focused on the relationship between intra-operative decisions in raTKA and post-operative outcomes have utilized subjective indicators of procedural success, such as patient-reported outcome measures (PROMs), patient-reported satisfaction, or pain scores (Aunan et al. 2015; Kappel et al. 2019; McEwen, Balendra, and Doma 2019). Few studies have linked objective post-operative gait metrics, such as gait speed or stride length, which have been suggested as measures of recovery complementary to PROMs following arthroplasty (Kaufmann et al. 2023; Yocum et al. 2023). Knee implants containing sensors for continuous passive collection of these types of data have been recently cleared for use, providing visualization of post-operative mobility recovery to both clinicians and patients (Cushner, Sculco, and Long 2022). Connection of intra-operative data from robotic systems to these objective mobility data, along with PROMs, may prove valuable in underpinning the associations between surgeons’ decisions intra-operatively and outcomes following TKA. However, little is known to date regarding how intra-operative data may relate to patient perception of recovery and objective gait recovery. In the absence of large cohort studies, this case study aims to illustrate the use of an orthopedic intelligence platform collecting data from the robotic system intra-operatively, objective mobility from an implanted tibial sensor, and PROMs from a smartphone-based care management platform.
All patients provided written informed consent for the publication of details concerning these cases.
Case histories
Case One
Patient one is a 65-year-old male with a body mass index (BMI) of 40 and a history of back pain. He reports no prior history or current use of tobacco. The patient initially presented with bilateral knee pain, with greater pain in the left knee which was previously treated with diclofenac and cortisone injections. The patient ambulated with a cane pre-operatively. Radiographs demonstrated bilateral advanced tricompartmental osteoarthritis with joint space narrowing, osteophyte formation, and subchondral sclerosis. At the initial pre-operative physical therapy evaluation, the patient had a numeric pain rating score (NRS) of 4; active range of motion was 95° of flexion and 10° of extension. The left passive range of motion was 100° of flexion and 8° of extension, flexion contracture was noted. Pre-operative Knee Injury and Osteoarthritis Outcome Score for Joint Reconstruction (KOOS JR) was 52.47 three days prior to surgical intervention.
The patient elected to undergo left knee replacement, performed using the ROSA® Knee System (Zimmer Biomet, Montreal, Quebec, Canada) and Persona IQ® (Zimmer Biomet, Warsaw, IN, USA), a personalized implant with a novel tibial stem extension (Canary Medical USA LLC, Carlsbad, California, USA). Embedded within the stem is an inertial measurement unit pairing accelerometers and gyroscopes for passive collection of gait data (step counts, gait speed, stride length, and cadence). A smartphone-based care management platform (mymobility®, Zimmer Biomet, Warsaw, IN, USA) pairs with the implant to provide objective kinematic data within dashboards for physician and patient review of post-operative recovery of these metrics.
Under spinal anesthesia, left total knee replacement was performed without incident utilizing a medial parapatellar approach without tourniquet. Surgeon preference dictated femoral cut first, with tibial prosthesis placed and cemented first. Final state assessment recorded by the robotic system intra-operatively demonstrated a well-balanced implant with 0.2mm difference between medial and lateral laxity at full extension (0.6mm medial laxity and 0.8mm lateral laxity), and 0mm difference at 90° of flexion assessment. The final hip-knee-ankle (HKA) angle was 3.2° varus. During post-operative discharge assessment, the patient was able to ambulate using a walker and climb 4 steps with the aid of a handrail, meeting all requirements for same day discharge.
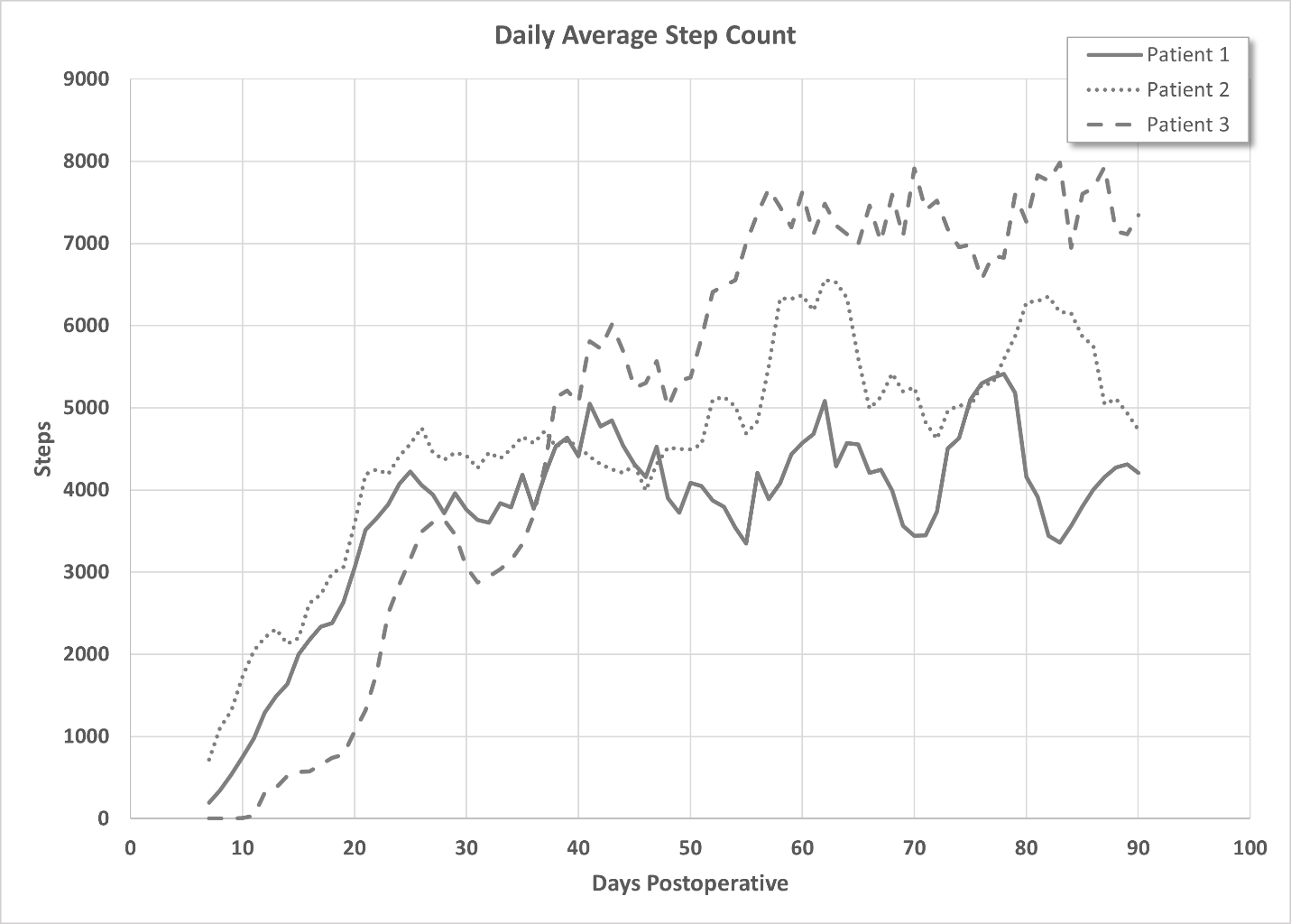
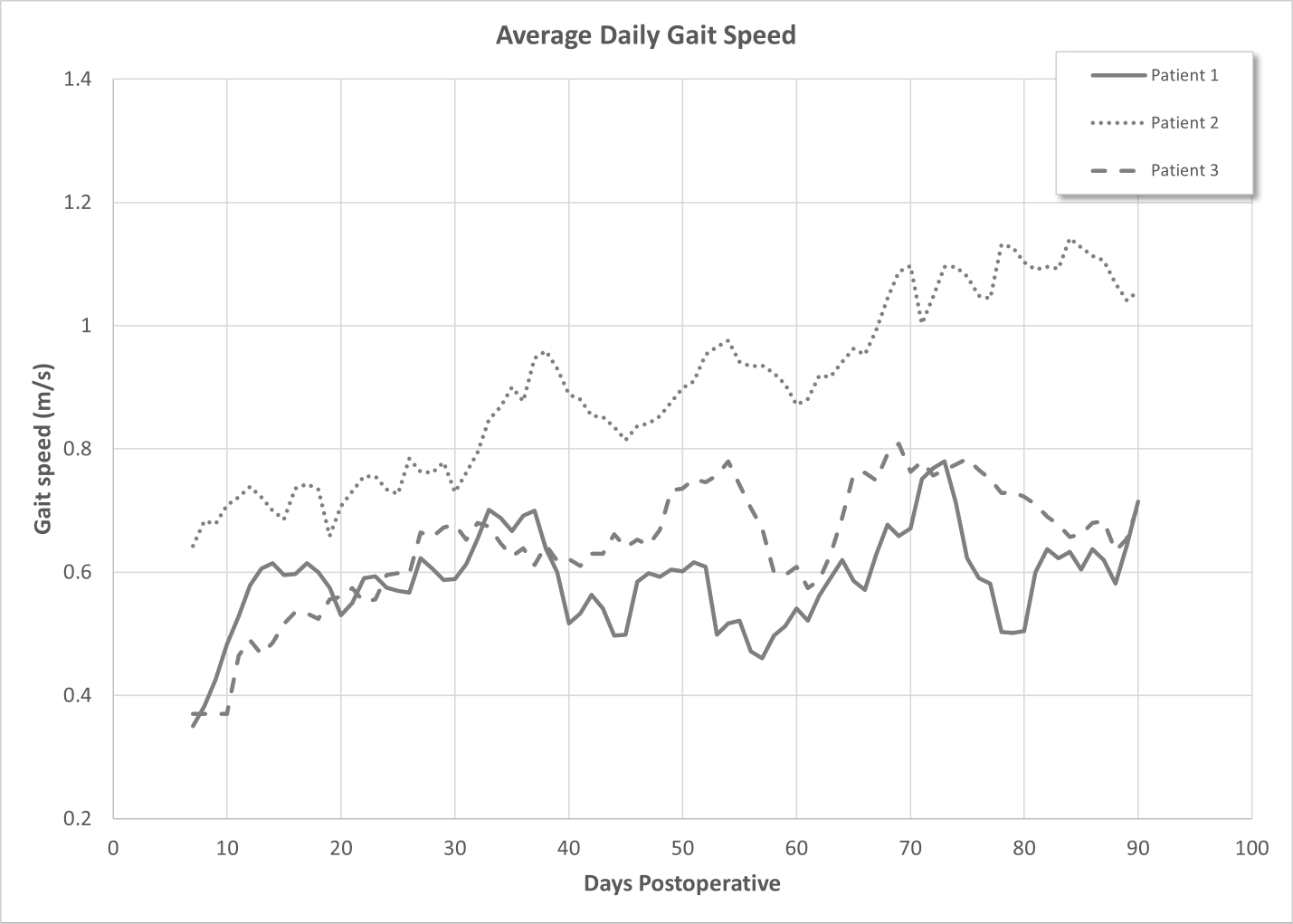
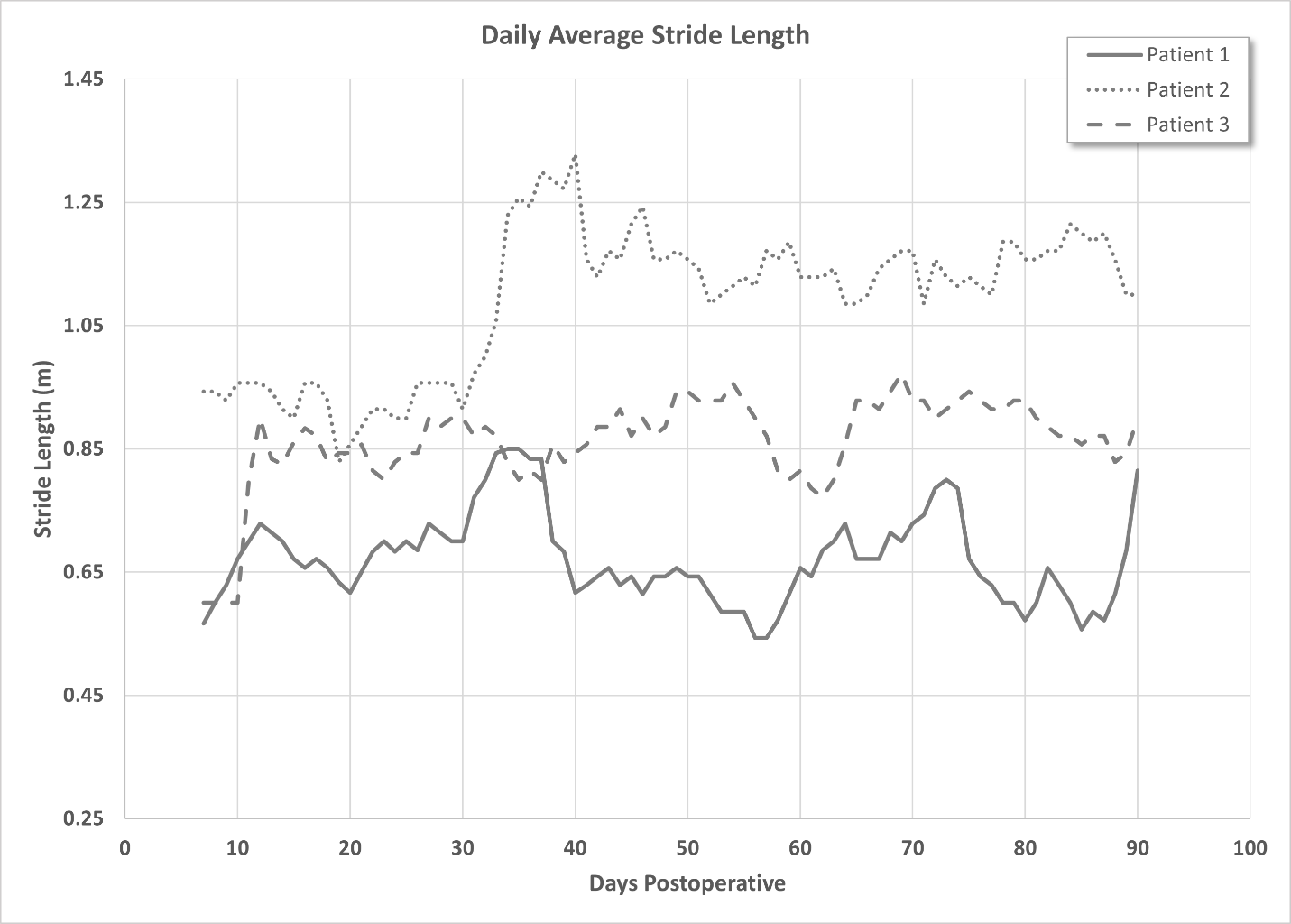
The patient achieved 0 - 106° total active flexion at two weeks post-operative and 0-129° flexion at five weeks post-operative. The KOOS JR score improved to 91.98 at five weeks. Radiographs taken at both visits demonstrated good positioning of implants. Gait metrics monitored post-operatively demonstrated gradual improvement of step counts, with a maximum of 9549 daily steps (7-day rolling average 4205 at 90 days post-operative, Figure 1). Gait speed also showed improvement in the post-operative period, improving from one-week post-operative of 0.35m/s to seven-day rolling average at 90 days of 0.71 m/s (Figure 2). Stride length improved from 0.56m at seven days to 0.81m at 90days (Figure 3). 96.6% data transmission from the tibial stem extension was achieved.

_as_recorded_by_the_implanted_t.png)

Case two
A 58-year-old female with BMI of 35.5 presented with severe left knee pain that had been increasing for a year, worsening with activity, and interfering with sleep. The patient had a history of anemia, noted moderate alcohol consumption, and reported no prior or current tobacco use. The patient X-rays showed left knee grade IV advanced tricompartmental osteoarthritis with joint space narrowing, osteophyte formation, and subchondral sclerosis. MRI, obtained approximately two years prior to the initial evaluation, revealed a medial meniscus tear and significant tri-compartment degenerative changes underestimated on X-ray. Clinical examination revealed flexion contracture with limited range of motion. The pre-operative KOOS JR score was 65.99.
The patient underwent robotically-assisted total knee arthroplasty with the same system as Case one and used the same implant including the tibial stem extension with embedded sensors. Surgery was performed under spinal block anesthesia, without tourniquet via medial parapatellar approach. The tibia was placed and cemented first under natural alignment, such that remaining HKA angles are present within the femoral component. The initial state assessment showed 1.2mm difference in laxity between medial and lateral compartments in full extension (0.9mm lateral) and 0.2mm at 90° of flexion assessment (0.7mm lateral laxity). Final state intra-operatively recorded values demonstrated a well-balanced knee with 0.2mm and 0.1mm differences in laxity between compartments at full extension and 90° of flexion, respectively. Final HKA angle was 2.1° varus. She was able to ambulate and ascend/descend steps post-operatively and deemed safe for same day discharge with no complications.
The patient was full weight-bearing at 3 weeks post-operative without use of assistive devices. At 6 weeks post-operative, the patient had returned to work and continued to ambulate independently. Active range of motion measured in the clinic was 1 - 124° total ROM. Physical therapy continued until 8 weeks post-operative, at which point the patient discontinued all narcotics and achieved 0 - 133° total active flexion. Radiographs demonstrated good positioning of implants. The KOOS JR score returned to a pre-operative level at 90 days post-operative which continued to improve out to six months post-operative with a score of 73.34.
Step counts as measured by the tibial stem extension showed gradual improvement over the first several post-operative weeks, with a seven-day rolling average of 4732 daily steps at 90 days post-operative (Figure 1). Gait speed also improved from 0.64 at 7 days post-operative to 1.06m/s at 90 days (Figure 2). Change in stride length was also observed (0.94 vs 1.1m at 7 and 90 days, respectively, Figure 3). Data transmission reached 100% for all gait metrics produced by the tibial stem sensor in this patient.
Case Three
Patient three is a 51-year-old male with a BMI of 26.8 and a three-year history of tobacco use. Additionally, the patient reported a history of patella fracture in high school. He initially presented with right knee pain; radiographs showed advanced tricompartmental posttraumatic osteoarthritis with joint space narrowing, osteophyte formation, and subchondral sclerosis with a KOOS JR score of 73.34. The patient had an active range of motion of 0 - 124° of flexion and elected for a robotically-assisted right total knee replacement and implant with the tibial stem extension sensor.
Surgery was performed under spinal anesthesia without the use of tourniquet. Median parapatellar approach was utilized, with placement and cementation of the tibia first. Data collected from the initial intra-operative knee state assessment during raTKA showed imbalance of the knee, with 4.3mm difference in laxity between the lateral and medial compartments at full extension (4.2mm laxity laterally) and 6.4mm difference at 90°flexion (5.9 mm medially). A Final knee state assessment demonstrated well-balanced compartment space with 0.2mm and 0mm difference in laxity at extension and 90°, respectively. The patient was able to ambulate and climb stairs post-operatively, meeting all requirements for the same day discharge.
The patient continued to recover without incident, using a cane for ambulation and reaching 0 - 91° of flexion at two weeks post-operative. He continued physical therapy for eight weeks post-operative at which point he reached 0 - 122° active flexion. Post-operative radiographs demonstrate good positioning of the implants. KOOS JR scores improved post-operatively reaching 63.78 at three-months post-operative.
Step counts improved from an average of 519 daily steps at two-weeks post-operative to 7344 at 90 days post-operative (Figure 1). Similarly, gait speed improved from 0.49m/s to 0.71m/s from 2 weeks to 90 days post-operatively (Figure 2). Stride length at 2 weeks was 0.825m, which increased to 0.9m at 90 days (Figure 3). Over the life of this implant to date, 96.9% data transmission from the stem sensor has been achieved.
Discussion
In these cases, we present three cases in which well-balanced knees were achieved with raTKA and who received a tibial stem extension with embedded sensors. Each patient attained at least 120° of active flexion within eight weeks post-operatively, and pre-operative KOOS JR scores were reached or exceeded by three-months post-operative. Objective measures of gait recovery indicate the majority of improvement occurred within the first six weeks following the procedure, similar to previous reports in the literature (Crizer et al. 2017; Twiggs et al. 2018). Of note, data transmission of the objective mobility metrics for all three cases ranged from 96% - 100%.
Technological advances have presented an array of opportunities within the field of orthopedics. Advances in machine learning and its potential to examine how intra-operative decisions might affect outcomes in arthroplasty may have significant implications in future practice. To capitalize on these advances, collection of a great volume of data across the episode of care is necessary, beyond that which could be reasonably collated by clinicians and their administrative staff. Further, that data must be able to be combined and integrated within singular platforms for effective analysis and discovery (Ramkumar et al. 2019).
We have presented examples of three patients in which high-volume, granular data collection was achieved and combined within a single platform to support this type of future analysis. PROMs were collected pre-operatively and throughout the episode of care without additional effort from clinic staff using a smartphone-based care management platform via mobile application or web-based portal. This type of electronic collection eliminates the need for clinic staff to transcribe paper responses for reporting, reducing errors and potentially improving completion rates (Muehlhausen et al. 2015). Of note, the application does not provide discrete daily step goals to patients but does encourage and remind users to walk 3-minute sessions three times per day in the first two weeks post-operative, increasing to 5-minute sessions three times per day after that. A progress feature in the application also presents an indication to users whether their current activity is low, on-track, or high compared to similar patients based on gender, age, and body mass index.
Robotic assisted arthroplasty lends itself to rich and complete data collection, capturing data relevant to the initial and final physical assessments of the knee, including flexion and extension, medial and lateral laxity during extension and flexion, HKA angles, and varus and valgus measurements during extension and flexion (Lonner et al. 2023). Further, implantable sensors as those described within the tibial stem extension within these cases, can collect post-operative mobility data over a long period of time with high fidelity.
There are a number of inherent limitations associated with this report. First, this is a small case series of three patients, such that statistical analyses are not possible. Additionally, only the feasibility of collection of pre-, intra- and post-operative data can be concluded from this report. It is not clear how other outcome measures, such as widely-accepted PROMs are correlated to these objective measures. Previous authors have suggested little correlation between these (Yocum et al. 2023), such that the measures should be considered together for a holistic view of patient recovery. Finally, the clinical significance of objective data gait and intra-operative balance and laxity information have not yet been established. Future studies to determine the importance of these data are needed.
A small case study of three patients cannot support statistical analyses to test hypotheses regarding the associations of intra- and post-operative data. However, this report demonstrates the ability to collect and connect a variety of large volume of data throughout the episode of care. Combinations of these types of data will support future investigations aiming to uncover relationships between pre- and intra-operative factors with post-operative outcomes and guide surgical decisions.
Summary
This case study demonstrates the ability to utilize a combination of new technologies in total knee arthroplasty to evaluate surgical decisions and perioperative outcome measures of pain, function, and mobility. The system was able to collect large amounts of data that could be visualized throughout the episode of care. Platforms that allow for collection of PROMs, intra-operative variables, and objective peri-operative mobility metrics and connect these data longitudinally could be a valuable resource for researchers and clinicians to understand TKA recovery and potentially predictors of both good and less preferred outcomes. Future studies need to focus on the relationship between pre-operative data and surgical decisions with post-operative outcomes using large datasets.