





INTRODUCTION
State-of-the-art design advancements in Total Knee Arthroplasty (TKA) carry significant importance in enhancing patient outcomes and implant longevity. These advancements, often incorporate innovative materials, improved biomechanics, and patient-specific instrumentation, aim to address limitations of previous designs, such as wear, instability, and the need for revision surgeries. Cutting-edge TKA designs not only seek to optimize implant survival and functional restoration but also strive to accommodate the unique anatomical variations of each patient, ultimately leading to improved kinematics and overall patient satisfaction. Furthermore, state-of-the-art TKA designs play a pivotal role in shaping the landscape of orthopedic surgery, driving continuous improvement, and setting new benchmarks for clinical excellence in joint arthroplasty.
Intermediate to long-term (10-year) follow-up in total knee arthroplasty (TKA) holds significant importance in providing valuable insights into the continued performance, durability, and patient outcomes associated with TKA systems (Patil et al. 2015; Ranawat and Boachie-Adjei 1988; Ranawat et al. 1993; Rodriguez, Bhende, and Ranawat 2001). As TKA is intended to offer lasting relief and functional restoration, a decade-long assessment allows for comprehensive evaluation of implant survivorship, potential complications, and patient-reported satisfaction. This extended follow-up period is essential for identifying any late-onset complications, assessing the need for revision surgeries, and gaining a deeper understanding of the natural history of TKA implants over time. Moreover, it enables the comparison of long-term outcomes between different TKA systems, guiding orthopedic practitioners in selecting the most suitable implants for optimal patient care. By examining the 10-year data, orthopedic surgeons and researchers can make informed decisions, better understand implant longevity, and contribute to the ongoing refinement of TKA systems, ultimately enhancing patient care and clinical outcomes.
There exist long-term TKA studies through various post-operative landmarks that yielded multiple intermediate publications (Walker, Ranawat, and Insall 1976; Ranawat, Rose, and Bryan 1984; Ranawat, Rose, and Rich 1984; Ranawat 1986; Ranawat, Flynn, and Deshmukh 1994). In all, these study series have revealed successful “performance and reliability of a surgical procedure”. Of the few long-term continuous reports, the publication series on the cemented Total Condylar prosthesis (Johnson & Johnson, New Brunswick, NJ; Howmedica, Rutherford, NJ) spans 20 years (Ranawat and Boachie-Adjei 1988; Ranawat et al. 1993; Rodriguez, Bhende, and Ranawat 2001; Insall et al. 1976), and the Press-Fit Condylar (DePuy Orthopaedics, Warsaw, IN) has been reported through 25 years (Patil et al. 2015). In addition, Young, et al, reported on 30-year results of the cruciate-substituting Insall-Burstein I (n=54), Insall-Burstein II prostheses (n=50), and eight constrained condylar cases (Zimmer, Warsaw, IN) in a younger population of TKA patient candidates (average age at surgery: 51 years) (Long et al. 2014). The authors reported survivorship at 30-years of 82.5% for femoral or tibial aseptic failure only, and 70.1% for any all causes. Interestingly, all IB-I patients were implanted with a monoblock tibial design of which 15 were all-polyethylene tibial components. Despite these excellent 30-year results, may alternative primary TKA designs have been introduced since and even evolved regarding modularity and levels of constraint.
As the field of orthopedic surgery continues to evolve to encourage shorter in-hospital recovery times, the relevance of long-term clinical data cannot be overstated. A thorough understanding of the longevity and functional outcomes of TKA systems is crucial for guiding clinical decision-making, enhancing patient counseling, and advancing implant technology. Moreover, the insights derived from long-term follow-up studies are instrumental in identifying potential modes of failure, refining surgical techniques, and informing the development of next-generation TKA systems. However, in most long-term results of TKA systems, there has been either significant changes in component design or discontinuation of the component being reported (Scott et al. 2019).
To advance the knowledge of the long-term results of the Freedom TKA system, the original patient population identified in previously published studies was monitored through their 10-year anniversary landmark (S. Durbhakula and Rego 2016; S. D. Durbhakula and Durbhakula 2019). The purpose of this study was to advance the knowledge base of the design performance and survivorship of the Freedom Knee system through the continuous monitoring of a previously reported early series TKA patient population.
MATERIALS AND METHODS
As was previous reported at the two- and five-year post-operative follow-up, between November 2010 and December 2013, the senior author performed 176 consecutive primary TKAs in 172 patients, without selection, utilizing the posterior stabilized (PS) Freedom Total Knee® system (MAXX Orthopedics, Inc., Plymouth Meeting, Pennsylvania) (FIGURE 1) (S. Durbhakula and Rego 2016; S. D. Durbhakula and Durbhakula 2019). The Freedom Total Knee system was originally introduced in 2007 and is manufactured from cast cobalt chromium (ASTM F-75 CoCrMo), and the articular bearing surfaces use ram-extruded UHMWPE (GUR 1020). When introduced, multiple “state of the art” design considerations was unique to this component design and remains highly relevant to the success of primary TKA, and unchanged to this date.
_freedom_total_knee_.png)
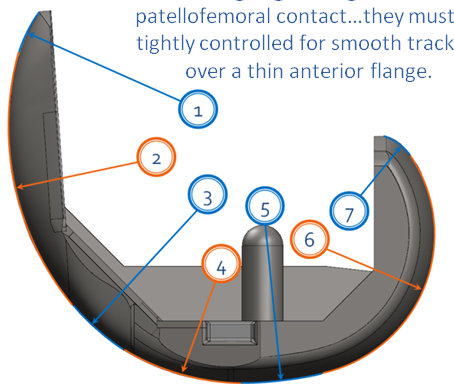
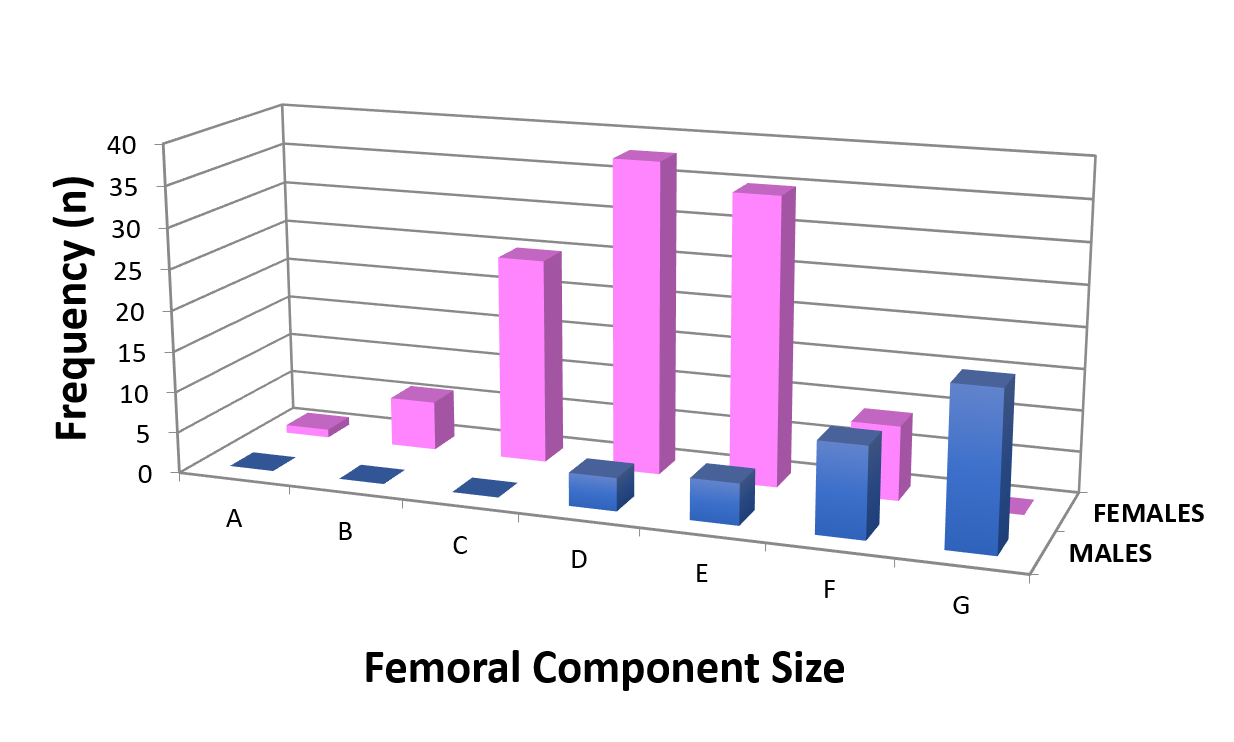
The Freedom Total Knee system was also designed with the intent to address bone conservation through reduced anterior and posterior femoral flanges, while allowing optimal high-flexion motion up to 155 degrees such as seen in frequent and prolonged squatting and kneeling, especially in the Pan-Asian patient populations. To achieve high-flexion, the femoral component was engineered utilizing a multi-radius design in which seven tangential radii were incorporated to accommodate smooth changes in rollback to avoid mid-flexion instability across the available surface through the transition from walking through deep flexion (FIGURE 2). In addition, development of femoral component sizing was optimized to include both the anthropomorphic dimensions of Western and Pan-Asian patient populations (Tanavalee et al. 2011). (FIGURE 3) Additionally, to accommodate deep flexion while maintain the quadriceps lever arm, a deepened 6-degree trochlear groove was incorporated into the femoral design. The tibial component was designed to minimize tibial bone resection for the tibial baseplate and low-profile tibial keel. The tibial baseplate also incorporates a five-point polyethylene locking mechanism, designed to prevent polyethylene insert micromotion (Lapaj et al. 2017; Sisko et al. 2017). Lastly, the system design (1) optimizes tibio-femoral conformity, (2) allows rotational laxity in flexion, (3) minimizes polyethylene contact stresses.


Of the 172 patients originally studied, there were 129 females (75.0%) and 43 males (25.0%) with an average patient age at surgery of 69.7 ±7.6 years (range: 52.3 years to 98.6 years). The average age of the female patient (69.3 years) when compared to the male patients (70.7 years) was not significantly different (p=0.311) (Table 1). In this continuous series, four female patients underwent bilateral TKA under the same anesthesia. In this set of patients, the pre-operative diagnosis was predominantly degenerative joint disease (DJD) in 170 knees (96.6%) and rheumatoid arthritis (RA) in 6 knees (3.4%). The surgical side was evenly distributed across all patients with 86 left (48.9%) and 90 right (51.1%) knees (Table 1). In all cases a tourniquet was used and a standard deep-vein thrombosis (DVT) prophylaxis of Lovenox® implemented (Sanofi-Aventis, Bridgewater, NJ). Additionally, summary of the previously 2- and 5-year reported data is listed in TABLES 1 and 2.
At a minimum of ten-years post-operatively, patients / patient families were contacted by phone to determine any changes or current adverse events, if the component was intact or revised, or if the patient was deceased. If there were any indications of adverse outcomes (pain, function, symptoms related to sepsis), the patients were encouraged to have a full clinical and radiographic assessment with the senior author. Lastly, if the patient was seen by their general practitioner or another orthopedic surgeon for their operated leg, or what would be indicated as “related to their operated knee,” we would ask to identify the physician so that we could request any clinical and/or radiographic information to update our survivability data. Following data collection, descriptive statistics were performed, and Kaplan-Meir survival rate method applied.
RESULTS
All 172 originally studied patients had post-operative assessments at a minimum follow-up of 2-years (average 3.8 ±0.9 years, range: 2.2 years to 5.3 years), and again at 5-years (average 6.5 ±0.9 years, range: 5.0 years to 8.1 years). For this study, all patients / patient families were contacted for their ten-year post-operative anniversary (avg: 10.5 years, range: 9.8 years to 11.4 years).
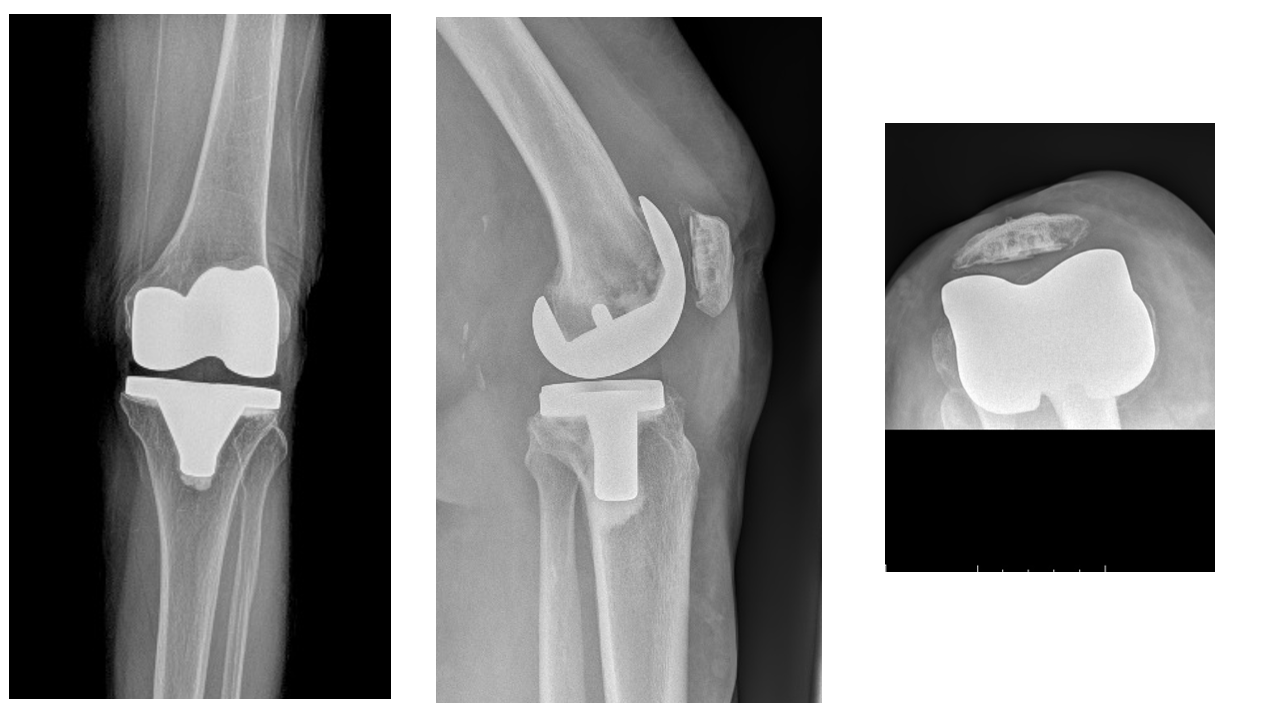
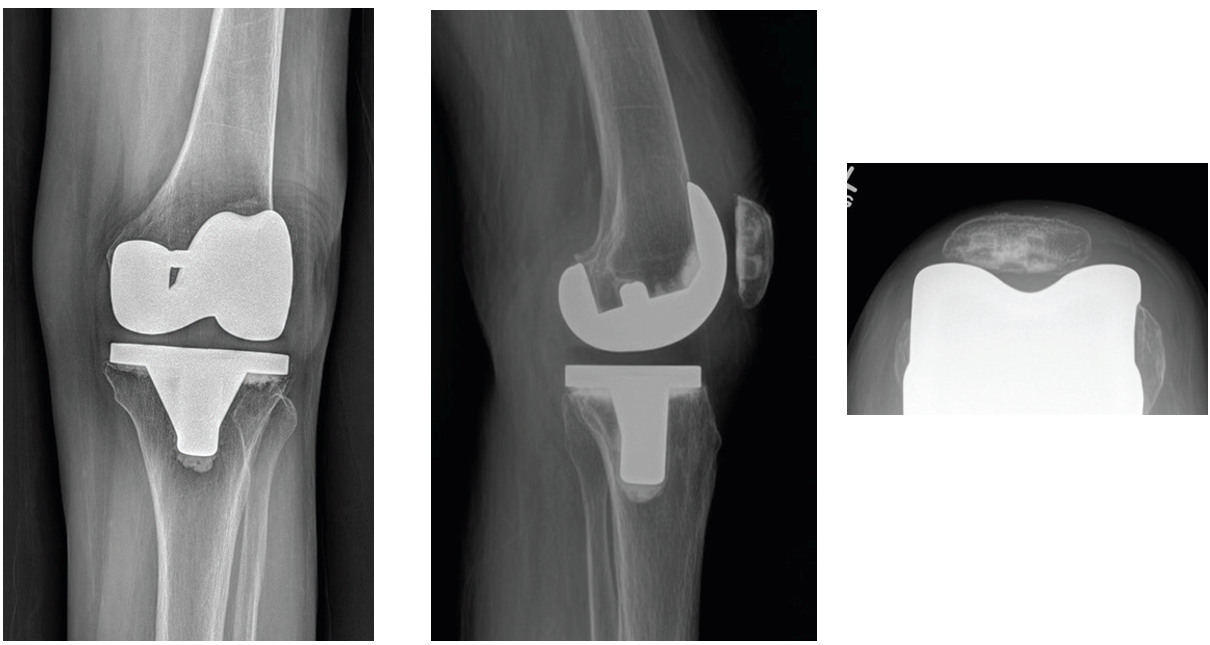
At ten-years post-operatively, all patients were accounted for. There was a total of ten (10: 5.8%) patients lost to follow-up, three (3: 1.7%) Patients deceased, and three (3: 1.7%) with early adverse events. Upon telephone follow-up, no patient reported any issues with pain, function or symptoms indicative of knee sepsis. Therefore, there were 160 TKAs in 156 patients available for inclusion in this study. Through the five years follow-up, there was no radiographic evidence of aseptic component loosening or osteolysis. However, there was one patient that was asked to return for a ten-year follow-up radiograph. This patient was originally imaged and included in the previous publications (FIGURES 5A-5D).

__lateral_and_skyline_patellar_knee_radiogra.png)
_after_primary_tka_with_the_maxx_freedom_knee_syste.png)
_after_primary_tka_with_the_maxx_freedom_k.png)
_following_primary_tka_with_the_maxx_free.png)
As was previously reported, two patients (1.1%) required subsequent incision and drainage surgery for superficial wound infections. Following these procedures both patients went on to successful clinical and functional outcomes through two and five-years post-operatively. No other patient had any subsequent infection through five-years. However, at 4.5-years post-index TKA, one female patient (<1%) with a previously well-functioning, Freedom Total Knee System prosthesis was involved in a motor-vehicle accident (MVA) that resulted in chronic pain and decrease of function involving the left proximal tibia. There was radiographic evidence of a proximal tibial stress fracture and tibial component loosening which were confirmed at the time of tibial component revision. Only the index tibial component and polyethylene insert were removed and a cemented Maxx Freedom® Knee Revision tibial baseplate (Maxx Orthopedics, Inc., Plymouth Meeting, Pennsylvania) with an extended tibial stem and PS polyethylene tibial insert were implanted without the use of any other adjunctive fixation hardware. The patient recovered without issue and at the most recent follow-up is well functioning without pain or ambulatory deficit.
Since there were 4 bilateral TKA cases in this study population, the Kaplan-Meier survival analysis was applied to all “knees” rather than patient count, calculated for an endpoint of revision, and showed a probability of survival of all TKA implants of 98.3% at ten-years follow-up (0.09% to 1.1%).
DISCUSSION
We report on the minimum ten-year follow-up of TKA survivorship of a single surgeon, non-randomized, consecutive case series of patients that received the Freedom Total Knee system. This is the third prospective follow-up report of the original population previously published (S. Durbhakula and Rego 2016; S. D. Durbhakula and Durbhakula 2019). The results of this current follow-up reveal continued optimum TKA performance without related complications, component failure or deterioration of the prosthetic composite. In addition, during the continued service life of the Freedom Total Knee System, there were no changes to the “state-of-the-art” design considerations included with its introduction for which are relevant today. Development and incorporation of femoral design characteristics that included deep flexion, dampening of mid-flexion instability, trochlear deepening while maintain distal femoral bone conservation are all relevant with today’s TKA designs and expectations.
Design considerations of total knee components have focused on the anthropometric dimensions common to western populations and factored for functional requirements of daily life prevalent in the western hemisphere. Overall, deep flexion TKA is achieved through lengthening the radius of curvature, increasing the posterior condyle offset and lengthening the trochlear groove (Long and Scuderi 2008). Addressing Asian and Middle Eastern populations that have increased societal expectation for achieving deep knee flexion (Long and Scuderi 2008; Tarabichi, Tarabichi, and Hawari 2010), Tarabichi concluded deep knee flexion up to 140° can be safely achieved without complications or component failure (Tarabichi, Tarabichi, and Hawari 2010). In 2007, the innovative design of the Freedom Total Knee System incorporated thinner condylar flange profiles that minimized the need for excessive condylar resection without sacrificing the component integrity. The condylar profile allowed for simultaneous deep flexion and rotation for high flexion activities and accommodated for a deep, 6° trochlear groove, which together maintained the quad lever arm during patellar tracking through deep flexion activities. Mid-Flexion instability is generally loss of articular congruity and partial loss of the flexion space and thus, joint stability (Stambough et al. 2019). The condylar anatomical profile of the Freedom Total Knee System incorporated 7-centers of rotation were designed to dampen the effect of mid-flexion instability and achieving a more normal knee kinematic and “feeling” during ambulation (Figure 2). Lastly, to address the Asian anatomic dynamic ration of medial-lateral / anterior-posterior (ML/AP) femoral components allowed for sizing pattern options for Asian populations (Figure 3).
The Freedom Total Knee System tibial baseplate was designed with a low-profile post and keel to minimize bone loss while maximizing component stability which is necessary through range of motion and into sustained deep flexion (Long and Scuderi 2008; Londhe et al. 2022; Brown, Lingampalli, and Hellman 2024). Following baseplate stability, the maintenance of minimal polyethylene insert micromotion required an advanced locking mechanism. In a study of micromotion between various tibial baseplates and corresponding polyethylene inserts, Engh, et al, reported on modularity instability to the “then” contemporary locking mechanisms with changes in physiological loading. The authors remark that deformation and repetitive motion attributes to increased wear, possibly inducing osteolysis and eventual tibial component loosening. The Freedom Total Knee System incorporates five peripheral points of snap-fit locks between the tibial baseplate and polyethylene insert. While eliminating all micromotion is impossible, it has been subsequently reported that a peripheral snap-fit capture in conjunction with a polished baseplate surface, performs better at minimizing micromotion and backside wear (Lapaj et al. 2017; Sisko et al. 2017). Overall, the tibio-femoral conformity design, restoration of condylar anatomy and maintenance of subsequent ligamentous constraint and laxity interactions through flexion minimizes polyethylene contact stresses and potential for adverse wear (Kappel et al. 2019).
Upon review of patients at minimum 10-years follow-up, one patient required revision of the tibial component following a motor vehicle accident (MVA) at 4.5 years post-operatively. At the time of revision surgery, use of the MAXX Freedom Knee Revision tibial component was used which allowed for retention of the well-fixed and functioning index primary femoral component. The MAXX Freedom Knee Revision tibial component is designed to allow for the use the MAXX modular polyethylene inserts, independent of component constraint and avoided the risks that are associated with any attempt to remove the well-fixed femoral component and reimplantation of an entire revision TKA system. In addition, a tibial stem was required to bypass the proximal tibial fracture. Following revision surgery this patient was well functioning but removed from further study.
As was identified in the earlier publications, this single surgeon, non-randomized consecutive case series had an imbalance of patients by gender (females n=129, males n=43) (S. Durbhakula and Rego 2016; S. D. Durbhakula and Durbhakula 2019). However, only femoral component size usage was significantly different, and expected. Additionally, the clinical outcomes measurements were not statistically different when comparing by gender. Also, there were 3 patient deaths and 10 patients lost to follow-up. The patient population age did range into the 80s and 90s and patient death and loss to follow-up was somewhat expected. While we are uncertain of the status of those patients lost to follow-up, according to the family members contacted, those patients that passed had no issue with their TKA at the time of death.
In this population Lovenox® (Sanofi-Aventis, Bridgewater, NJ, USA) was used in all patients as their DVT prophylaxis, which has been changed to aspirin due to current results in the literature. Also, the patients included were of a Western ancestry population, and unfortunately no comparative assessments to Middle Eastern or Pan-Asian populations were available. However, efforts are being made to capture a similar study data across various ancestral populations for comparative review with the currently presented study group.
While we are have attempted to revisit the previously published patient population and update results, we have also identified limitations in performing long-term follow-up studies even in a single surgeon setting. We decided to implement the telephone review for 10-years to assess any significant changes which would trigger a subsequent follow-up. This strategy may eliminate the scheduling and transportation burdens, especially in this elderly patient population, it does eliminate the continuation of measurable data upon follow-up. We thus sacrificed the continuation of the HSS scores and radiographic assessments at 10 years. Also, at the time of surgery, the extensive use of patient reported outcome measures (PROMs) were not implemented in the senior author’s practice. This has since changed but was not used as a single point at 10-years. Changes in patient record keeping to electronic medical records (EMRs) eliminates data that was originally collected in paper format. Large medical practices eliminated paper charts without archiving much historic information which renders any re-reviews of the data impossible. Nonetheless, we believe that current efforts in national registries will allow for more formal use of clinical assessments and PROMs to allow greater assessments of components, procedures and treatment strategies.
In conclusion, the results of this study of patients receiving the Freedom Total Knee System for primary TKA clearly support the original design considerations for anthropomorphic considerations while achieving an increased degree of ROM while minimizing bone resection. The study at 10-years included a large cohort (160 knees, 156 patients) of continuous non-selected series of patients accounted for with minimal loss to follow-up / death / adverse events. From these results we believe that continued use is recommended, and that further study is warranted to confirm achieving similar results across surgeons and to further study across multiple ancestral populations.
ACKNOWLEDGMENT
The authors wish to thank all the many contributing researchers, authors and especially the patients for their continued commitment and support of this research effort throughout the last ten years.