
**_a_cementless__tapered_fluted_femoral_stem._b)_note_the_longitudinal_splines_along_t.tiff)
**_explanted_fluted_stem._note_the_bone_ongrowth_throughout_the_stem_length._d__e)_b.tiff)
_case_1**__a)_plain_pelvic_radiographs_of_a_42-year-old_female_who_presented_with_re.tiff)

Introduction
Whenever indicated, extraction of a well-fixed femoral stem is a challenging procedure that may lead to iatrogenic femoral cortical fractures with an incidence ranging from 12-82.8%. (Masri, Mitchell, and Duncan 2005; Matthys, Van Meirhaeghe, and Pattyn 2021). To reduce the risk of iatrogenic fracture, it is essential to carefully identify the reason behind the revision and plan for the utilized surgical technique. Accordingly, the particular stem type selected as well as the tools and implants used will be taken into account. (Barrack and Burnett 2005; Haynes et al. 2016).
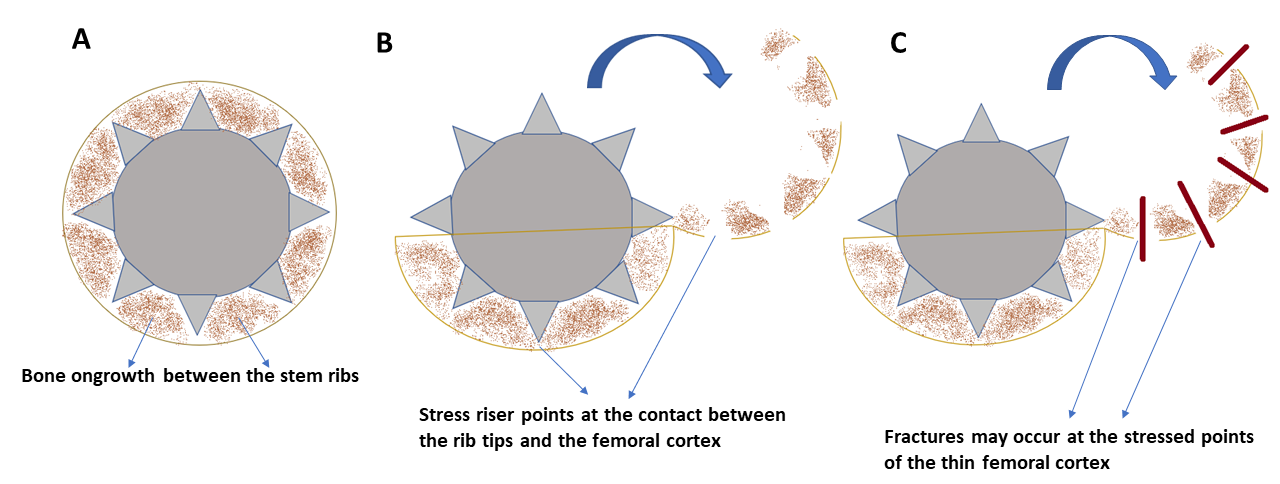
Cementless fluted, tapered femoral stems were introduced to allow for rigid primary stability, provided by the roughened surface and the longitudinal splines along the stem (Figure 1) and secondary stability through osseointegration (bone ongrowth) along the stem, in revision hip arthroplasty (Abdel et al. 2017). Since its introduction, several studies reported excellent survival results (Masri, Mitchell, and Duncan 2005; Zang et al. 2019; Otero et al. 2020; Park et al. 2021) despite their various designs. The reported adequate osseointegration with these stems (Figure 2), providing long-term implant stability (Park et al. 2021), has rendered them the implants of choice in revision hip arthroplasty among many surgeons (Wagner and Wagner 2000; Otero et al. 2020; Park et al. 2021).
**_a_cementless__tapered_fluted_femoral_stem._b)_note_the_longitudinal_splines_along_t.tiff)
**_explanted_fluted_stem._note_the_bone_ongrowth_throughout_the_stem_length._d__e)_b.tiff)
Given these stem characteristics and the remarkable osseointegration, extraction of fluted, tapered cementless stems during revision surgery can be technically demanding. The stem splines may have already created several stress risers at their contact with the femoral cortex. Unplanned insertion of osteotomes/ chisels in the stem-bone interface, and unplanned extended femoral osteotomy (King et al. 2008) in these settings may lead to iatrogenic perforations and fractures of the femoral cortex (Figure 3, 4A-G), which can compromise the stability of the new revision femoral stem.
**_conceptualized_cross-section_of_a_tapered__fluted_stem_with_bony_integration_betwee.png)
Despite the presence of several reports that discuss how to revise femoral stems (Burstein et al. 2004; Masri, Mitchell, and Duncan 2005; Laffosse 2016; Khan et al. 2015), there is only one study that discussed in detail the K-wire drilling technique for extraction of cementless femoral stems in general (Hafez 2017). The purpose of this study is to revisit the K wire extraction technique, particularly for the tapered fluted cementless stems, giving their unique design. We believe this technique is simple and reproducible and does not require specific advanced surgical instruments.
TECHNIQUE
The patient is positioned, and surgical exposure is performed through the approach of the surgeon’s discretion. After exposure of the proximal portion of the stem, a trial of stem extraction using the stem applicator and back hammering may be attempted if the stem is felt to be loose. In cases where it is well fixed, further exposure of the proximal portion of the stem is performed using burrs, fine bone rongeurs and/or chisels until clearly viewing the proximal portion of the flutes or splines of the stem. This may necessitate performing bone trimming around the proximal, non-ridged portion of the stem in order to visualize the splines (ridges) and flutes.
At this stage, after proper exposure of the proximal portion of the stem, until viewing the proximal end of the splines, multiple forward and backward longitudinal drills were passed through the flutes between the splines downwards, guided by the C arm. Repeated drill passages are performed from proximal to distal until completing all the holes between splines (see Video 1 in the Supplementary Materials). Either a 1.8-2.2mm K-wire or 2-2.5mm drill bit is used and longitudinal drilling is performed along the 8 holes (Figure 4 I,J). The drill bit or K wire may be tilted between the splines during drilling. Additionally, a fine chisel may be then used in the same manner between the splines from proximal to distal to further free the stem. At this stage, the stem is almost loose and can usually be extracted utilizing the applicator and back hammering, or through an extended trochanteric osteotomy that should leave a single, intact femoral cortex (Figure 4 K). This is followed by fixation of the osteotomy with cerclage wire (Figure 4 L) and insertion of a spacer or revision THA stem as planned. A longer and larger, diaphyseal fitting stem is usually utilized when revising a fluted stem, and utilization of a stem with distal transfixing screws is a viable option.
_case_1**__a)_plain_pelvic_radiographs_of_a_42-year-old_female_who_presented_with_re.tiff)
Expected Outcomes
The longitudinal drilling technique can assist the surgeon in extracting a well-fixed, fluted cementless femoral stem while decreasing the risk for iatrogenic femoral fracture.
Complications
Potential complications include iatrogenic femoral metaphyseal and femoral shaft perforation with the wire, drill bit or wire breakage inside the femoral canal. Careful placement of the wires or drill bits inside the flutes through proper proximal exposure may decrease the chance of iatrogenic perforation or hardware breakage.
Discussion
This study describes a reproducible method for extraction of well fixed, uncemented, fluted conical stems. Although this technique is utilized by many surgeons it has only been described once in detail for uncemented femoral stems in general (Hafez 2017). Given the unique design of fluted stems, we believe this technique is particularly useful in such stems and we aimed to add to the existing literature for more popularization of the technique. The presence of flutes and splines in such stems can guide the drilling technique while decreasing the chance of femoral cortical perforation and K wire bending or breakage.
Extraction of well-fixed cementless stems in revision THA is a technically challenging procedure. Preserving a well-fixed original stem during revision surgery, when acetabular-side revision alone is adequate, has the potential to reduce time, blood loss, and minimize the risk of additional tissue injury and bone damage (Hafez 2017). However, stem removal is performed for multiple indications during the revision surgery, including infection, recurrent instability due to stem version and offset defects, stem breakage, taper damage, limb length discrepancy due to stem subsidence or mal insertion causing lengthening, femoral osteolysis, taper mismatch with the revision system, bony ankylosis, or during the revision of excessively medialized or mispositioned cup (Laffosse 2016; Randhawa et al. 2009; De Thomasson et al. 2001; Wahl et al. 2021; Reina et al. 2013).
Given the unique stem design and bone ongrowth, unplanned stem removal may result in unexpected bony damage. The proposed technique of axial drilling allows for a more predictable stem extraction, minimizing bone damage. Since it does not require specific instruments and could be tried in a timely fashion, we believe this technique is reproducible and helpful to be performed whenever extraction of a fluted, tapered stem is required.
Conclusion
The longitudinal drilling technique along the stem flutes is a reproducible technique that allows for partial loosening of well-integrated, fluted cementless tapered stems. This technique allows for easier stem extraction minimizing the risk of significant bony comminution or damage.
Conflicts of Interest
None to declare.