



Introduction
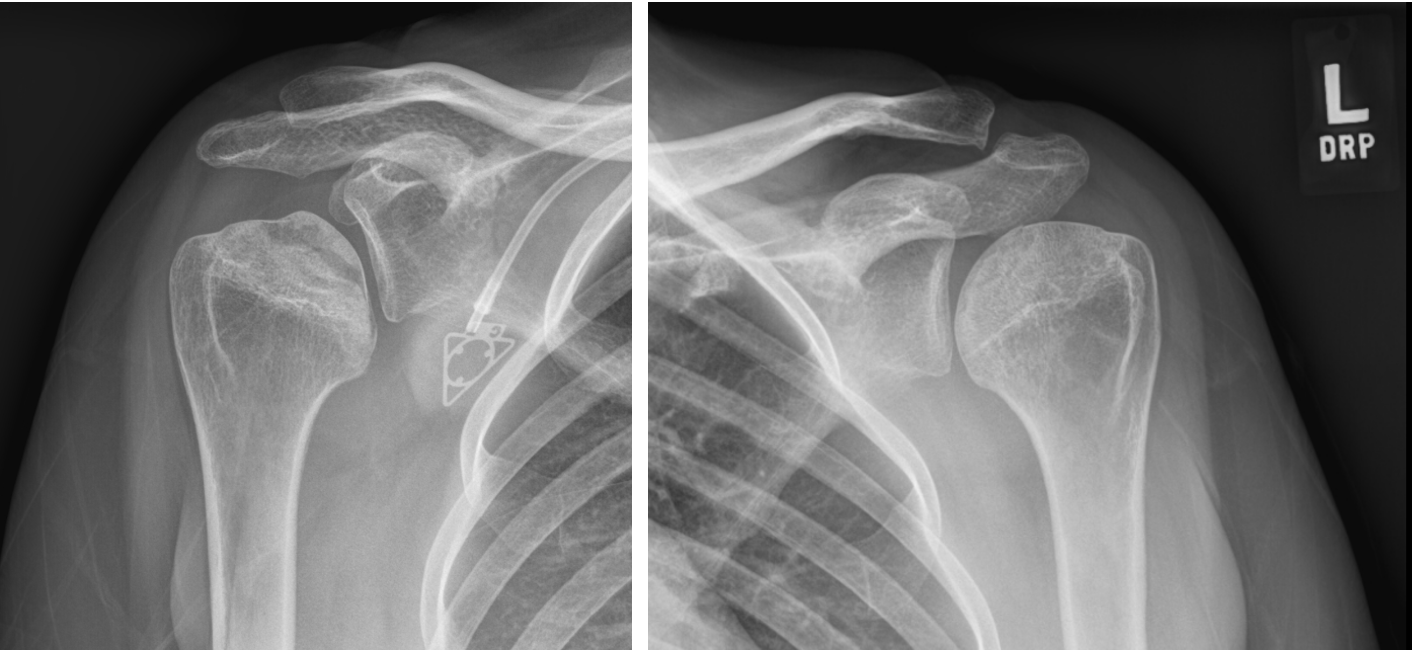
Surgical treatment of patients with glenohumeral arthritis who are young and active remains a challenge. After non-operative treatments are exhausted, the joint-replacement surgical options to address advanced glenohumeral joint arthritis include anatomic shoulder arthroplasty (TSA), hemiarthroplasty (HA), ream-and-run, and in some situations reverse shoulder arthroplasty (RSA). Shoulder HA remains an option for young patients (typically under 60 years old) with glenohumeral arthritis and intact rotator with significant activity demands that would be concerning for early glenoid wear in the setting of an anatomic shoulder arthroplasty. Shoulder HA can also be a treatment for patients with proximal humerus avascular necrosis (AVN) as seen in Figure I and II. Shoulder HA involves replacing the arthritic humeral head and allowing the metal humeral head to articulate with the native glenoid. The main bearing component of the humeral head has traditionally been metal, an alloy of cobalt-chromium (CoCr). However, pyrocarbon implants recently have been introduced as an alternative bearing surface to attempt to reduce native glenoid wear and erosion.
Pyrolytic carbon (Pyrocarbon) recently, has been used as an alternative bearing surface to metal humeral heads. It was initially introduced in the 1970’s in artificial heart valves (Bokros 1977). In orthopedics, it has been used successfully in hand and wrist arthroplasty (Daecke et al. 2006). Pyrocarbon has been shown to have high wear resistance, low friction and a modulus of elasticity similar to that of cortical bone (Bokros 1977). This review will focus on the use of pyrocarbon humeral heads in the setting of HA of the shoulder. We will discuss the indications of use, biomechanical properties of pyrocarbon, early clinical outcomes, and implant availability.


Indications for Hemiarthroplasty
An orthopedic surgeon has multiple tools available when it comes to managing patients with glenohumeral arthritis. Anatomic TSA is used for patients with intact rotator cuffs, and RSA is utilized in patients with significant glenoid deficits/deformity or massive irreparable rotator cuff tears (Walch et al. 1999). HA is primarily used for patients with healthy glenoid cartilage (Streubel et al. 2014; Wiesel, Nagda, and Williams 2013), and in younger patients that are active (Fevang et al. 2009). It is also commonly used in patients with irreparable proximal humerus fractures which would have an unacceptably high rate of AVN. HA is a procedure which involves resurfacing the humeral head while leaving the glenoid intact. This procedure was pioneered by Neer in the 1950s, and he popularized the use of a stemmed humeral head replacement for patients who had proximal humerus fractures and glenohumeral arthritis (Neer 1955). There are now multiple different options available for HA, which include partial humeral head resurfacing, stemless HA, and many different stemmed, modular components.
HA used to have broad indications and was commonly performed, but it has since more seldom been performed given the improved pain and functional outcomes associated with anatomic TSA (Padegimas et al. 2015). Additionally, younger patients frequently have lower satisfaction with shoulder arthroplasty than older patients (Sperling, Cofield, and Rowland 2004, 1998). HA theoretically is an advantageous option for a young patient with minimal to no glenoid-sided arthritic changes. It was initially thought of as a “bridge procedure” to buy patients time while their glenoid arthritis progressed before ultimately revising to an anatomic TSA. However, long-term concerns have arisen with the use of this procedure including glenoid erosion/bone loss, loss of joint space, and subchondral sclerosis leading to conversion to TSA, which then performed worse than the primary TSA patient population (Sperling, Cofield, and Rowland 2004; Carroll et al. 2004; Gartsman, Roddey, and Hammerman 2000; Maier et al. 2014). One study by Essilfie and Gamradt concluded that the best current indication for HA is a young patient with humeral head osteonecrosis and intact glenoid cartilage (Essilfie and Gamradt 2018).
There is an alternative technique which has been coined ream-and-run, described many times and involves performing an HA with concentric glenoid reaming (Saltzman et al. 2011; Lynch et al. 2007; Clinton et al. 2007). The advantage of this technique is that it addresses the glenoid without utilizing a polyethylene glenoid component which can wear and loosen over time, and it also avoids the complexities and risks associated with soft tissue interposition. In a study conducted by Saltzmann et al, they concluded it is critical that the humeral head component has a diameter of curvature which is 2mm smaller than the reamed glenoid. Additionally, they said surgeons should pay attention to the alignment of the humeral component within the glenoid to ensure there is no abutment in adduction or external rotation (Saltzman et al. 2011). Clinton et al demonstrated the ream-and-run procedure to have comparable functional results with TSA, but it took on average 12 to 18 months longer for the ream-and-run shoulders to reach a similar level of function (Clinton et al. 2007). Despite these promising results of this technique, the results in the literature are mixed with surgical revisions rate ranging from 2-25% (Matsen, Carofino, Green, et al. 2021).
Ultimately, there are a handful of commonly used techniques used in the management of the arthritic shoulder, each with their own advantages and disadvantages. Much of the decision making will come down to patient factors, surgeon preference, and risk profiles the patient may want to accept. HA is most often going to be considered in the young patient who leads an active and demanding lifestyle, with the knowledge that there is a risk of conversion to TSA if they develop glenoid bone loss, erosion, and subchondral sclerosis.
What Is Pyrocarbon
Pyrocarbon is a material which was initially created as a coating for nuclear fuel in the 1960s. After its hemocompatibility and ideal mechanical properties were discovered, the material was first trialed in the medical field in the 1970’s as a component of mechanical heart valves. As mentioned previously, it was initially being used with some degree of success in hand and wrist arthroplasty starting in the 1990s (Daecke et al. 2006; Beckenbaugh, Klawitter, and Cook 2006; Dickson et al. 2015). The material itself is composed of a coating of carbon deposited on a graphite substrate, which leads to its classification as a ceramic. The carbon is deposited by deposition of a vapor chemical at temperatures just over 1,500 degrees Celsius leading to thermal break down of a gaseous hydrocarbon (Bellemère 2018). The hemocompatibility is due to its hydrophobic nature, which allows for protein absorption at the surface of the implant. Since the proteins are not denatured, blood platelets are not activated, and fibrinogen is not converted into fibrin (Feng and Andrade 1995). There have been no toxic or allergic immune responses to pyrocarbon reported in the literature, and this is likely due to its stable and inert structure, which different from metal does not have free radical or ionic form. There have also been no reports of particles being transferred throughout the body hematogenously or infiltrating periarticular spaces (Bellemère 2018). Finally, the graphite in pyrocarbon allows for absorption of phospholipids which have a component called dipalmitoylphosphatidylcholine (DPPC) causing enhanced joint lubrication and reduction of friction between the component and the adjacent joint (Gale et al. 2007). All of the properties of pyrocarbon listed above contribute to it being a safe and effective material for usage in the HA patient population.
The material itself is poor in flexion, strong when being compressed, and it possesses ideal elastic properties (Stone et al. 2021). Pyrocarbon has a similar modulus of elasticity to that of cortical bone, and it also stimulates the expression of type II collagen promoting the formation of a cartilaginous matrix (Hannoun, Ouenzerfi, Brizuela, et al. 2019). The modulus of elasticity allows for the harmonious transmission of stress between the implant and bone minimizing the phenomenon of stress shielding (Hassler 2012). Metals have been reported to lose 30-50% of strength with repeated loading. Conversely, pyrocarbon has excellent fatigue resistance and there have been no fatigue fractures reported in mechanical heart valves in over 30 years of use (Bellemère 2018; Cao 1996). An in vitro comparison on wear properties of pyrocarbon and metal-on-bone shoulder HA has demonstrated bone volume loss rate, linearized bone penetration rate, and surface roughness of cobalt chromium test specimens to be 30 times greater than pyrocarbon implants (Klawitter et al. 2020). Another study performed by Cook et al. evaluated cartilage wear in the canine acetabulum with a variety of different HA components on the femoral side including pyrocarbon, CoCr, titanium, and aluminum. They found after 18 months that the acetabulum cartilage survival rate with pyrocarbon HA was 92% vs 20% for metal implants (Cook, Thomas, and Kester 1989). A different in vivo study of canine knees with osteoarthritis compared pyrocarbon implant versus CoCr implants and their ability to create fibrocartilage regeneration in the opposing joint surface. They found pyrocarbon to lead to fibrocartilage regeneration in 86% of cases versus 25% for CoCr (Kawalec et al. 1998).
Biomechanical Studies
As mentioned above, the use of pyrocarbon in joint arthroplasty has been described throughout the literature in recent years. However, the majority of studies have focused on the application of pyrocarbon in hand and wrist arthroplasty, with limited research in the context of shoulder arthroplasty. Due to its mechanical properties outlined above, including increased wear resistance and similarity to cortical bone, pyrocarbon implants have grown in popularity and are emerging as a topic of discussion for shoulder arthroplasty, especially in young active adults.
For example, in one study by Ramirez et al., looked at the wear characteristics of pyrocarbon humeral head implants coupled with polyethylene glenoid inserts after 5 million cycles using the Newcastle Shoulder Wear Simulator (Roberson, Bentley, Griscom, et al. 2017). This simulator mimics in vivo shoulder conditions and is fully programmable to include a wide variety of shoulder range of motion and dynamic loads. They then calculated the amount of wear on both the pyrocarbon humeral component and the polyethylene glenoid component by using gravimetric measurements, three-dimensional images with a non-contacting profilometer and scanning electron microscopy (Roberson, Bentley, Griscom, et al. 2017). They discovered that the mean roughness value of the polyethylene components decreased from 296 ± 28 nm to 32 ± 8 nm (P < 0.001), in contrast to the pyrocarbon humeral heads which remained in the same range from 21 ± 2 nm to 20 ± 10 nm (P = 0.855) (Roberson, Bentley, Griscom, et al. 2017). Importantly, they also found that there was no change of weight of the pyrocarbon implants, indicating no measurable form of wear following 5 million cycles in the shoulder simulator (Roberson, Bentley, Griscom, et al. 2017).
Mueller et al. evaluated the effect of ceramic versus metallic humeral heads on glenoid polyethylene wear in anatomic TSA (Park, Zhang, Chang, et al. 2023). They found that the average polyethylene wear rate decreased by 26.7% in the ceramic humeral head group when compared to the metallic humeral head group (Singh Jagdev et al. 2022). Although their study was evaluating the effect of different humeral components on polyethylene glenoid components in the setting of TSA, this lends to the thought process that a prosthesis with similarities to bone might reduce native glenoid wear in HA. This was demonstrated by another in vitro study that looked at the effect of pyrocarbon and CoCr humeral prostheses on wear of cortical bone in fresh bovine samples. During their testing, CoCr implants were only subject to roughly 320,000 cycles in the simulator due to complete bone consumption/destruction while pyrocarbon implants completed the 5 million cycles of testing (Klawitter et al. 2020). The difference in surface roughness between pyrocarbon and CoCr implants was also notable at 87 ± 55 nm and 3317 ± 1648 respectively (P < 0.05). Therefore, their results suggest that pyrocarbon implants were less damaged by bone and ultimately did significantly less damage to bone than CoCr prostheses.
Clinical Outcomes
As discussed above, the relatively recent adoption of pyrocarbon implants in the shoulder provides limited opportunity to understand long-term outcomes of HA with this material. Additionally, the limited outcome data available for pyrocarbon HA must be interpreted within the context of revision and failures rates of existing solutions for osteoarthritis and in the young, active patient. For example, TSA in young (<65 years) patients is associated with a 18% revision rate, with 54% of patients demonstrating glenoid lucency, which may limit options for revision surgery (Roberson, Bentley, Griscom, et al. 2017). Additionally, revision rates for traditional HA with metal implants may be twice that of anatomic total shoulder arthroplasty (Singh Jagdev et al. 2022), with progressive glenoid erosion or rotator cuff failure necessitating revision procedures. Consequently, conversion of failed HA or total shoulder arthroplasty to reverse total shoulder arthroplasty may be associated with scarred tissues plains, difficult glenoid exposure, and poor glenoid bone stock. As such, the use of pyrocarbon for HA can be viewed as a potential alternative to a clinical challenge with a myriad of imperfect solutions.
A systematic review of shoulder HA with pyrocarbon demonstrates significant improvement of range of motion and clinical outcomes, with a 4.8% rate of conversion to TSA at a minimum of two years (Park, Zhang, Chang, et al. 2023). Large registry studies do suggest that pyrocarbon HA have significantly lower revisions rates than tradition metal HA with conversion rate to TSA (McBride, Ross, Hoy, et al. 2022; Gao et al. 2023), and may offer similar or improved revisions rates when compared to anatomic TSA in younger patients (Gao et al. 2023). Additionally, in the event a pyrocarbon HA needs to be revised, the stem is designed to be press fit which is advantageous in the revision setting as there is no cement in the humeral canal. Despite this favorable data, total shoulder arthroplasty continues to demonstrate superior improvements in post-operative motion and shoulder function, when compared to both pyrocarbon (Gao et al. 2023) and metal HA (Garcia, Liu, Mahony, et al. 2016). As such, future justification of pyrocarbon HA will likely necessitate improved survivorship and/or relative preservation of the glenoid for subsequent conversion to anatomic or total shoulder arthroplasty, when compared to total shoulder arthroplasty.
Importantly, numerous studies demonstrate that the use of pyrocarbon does not eliminate the presence of glenoid erosion over time, as 20-50% of individuals with pyrocarbon implants will demonstrate some progression of glenoid erosion at intermediate-term follow-up (Park, Zhang, Chang, et al. 2023; Cointat, Raynier, Vasseur, et al. 2022; Garret et al. 2024). Of note, while the in vivo effect of pyrocarbon on glenoid erosion are unclear, pyrocarbon humeral heads are uniquely susceptible to implant fracture. While fracture of the humeral head is essentially non-existent in metallic implants, implant fracture may occur in up to 5% of patients with pyrocarbon HA (McBride, Ross, Hoy, et al. 2022). Therefore, due to their novel method of failure, surgeons must be thoughtful in their medical decision making when using these implants for clinical practice and appreciation of potential drawback of wide-spread adoption of pyrocarbon implants in shoulder arthroplasty.
Moreover, non-anatomic reconstruction of the humeral head is associated with worse clinical outcomes in patients undergoing HA with pyrocarbon implants. Non-anatomic reconstruction – typically related to overstuffing of the humeral head – is strongly associated with worse range of motion, clinical outcomes, glenoid erosion, rotator cuff deficiency, and revision rates (Cointat, Raynier, Vasseur, et al. 2022). Characteristics of morse taper designs in current implants has been postulated to contribute to oversizing of the humeral head, given additional implant thickness needed to support the pyrocarbon implant on a metallic tray (Cointat, Raynier, Vasseur, et al. 2022). Thus, the challenge of accurately restoring the humeral center of rotation and the impact of anatomic reconstruction on clinical outcomes, this technical aspect of pyrocarbon HA is of paramount importance as it is in anatomic TSA.
In summary, the clinical outcomes and survivorship or pyrocarbon shoulder implants is limited by the recent adoption of the material and the narrow indications for HA in modern shoulder surgery. However, HA with pyrocarbon implants demonstrate acceptable clinical outcomes and survivorship at intermediate-term outcomes, with some evidence to suggest favorable glenoid wear-rates and survivorship when compared to traditional metal implants. However, the material properties of the implant allow for humeral head fracture, which represents a unique cause for revision when compared to traditional metallic implants. Total shoulder arthroplasty likely provides superior clinical function and pain relief in younger patients with osteoarthritis, but the concerns regarding glenoid loosing and osteolysis in younger populations suggest pyrocarbon HA may possess a role in the management of osteoarthritis in the young patient with high activity demands or humeral osteonecrosis. Further longitudinal data is required to define long-term implant survivorship and delineate if pyrocarbon implants offer long-term benefits for glenoid erosion.
Implants Available
When it comes to utilizing these pyrocarbon implants in the United States, there is only one product which has been FDA approved. This is Stryker’s Tornier Pyrocarbon Humeral Head (Stryker, Mahwah, NJ, USA), and the first case was completed at the Denver Surgery Center in Colorado on March 20, 2023.
There are a variety of other pyrocarbon humeral head systems which have been developed and used frequently internationally but are not FDA approved. One commonly used prosthetic is the PyroTITAN system (Integra, Plainsboro, NJ, USA). This implant has had significant utilization internationally. In the Australian National Joint Registry, this implant demonstrated improved survivorship at 5 years follow up for patients under 55 years-old compared with all other classes of arthroplasty in this registry (McBride, Ross, Hoy, et al. 2022). Another frequently used implant is the INSPYRE pyrocarbon interpositional implant (Tornier/Wright Medical, Bloomington, MN, USA). This implant was evaluated in a prospective observational study by Barret et al. from France (Tsitlakidis, Doll, Westhauser, et al. 2021). Fifty-eight patients received this implant, and at mean follow up of 47 +/- 15 months, survival rate was 90% with 10% requiring revision to TSA (Barret et al. 2020). There are other products which have been developed by industry and are in the development process, but these three aforementioned systems are the most commonly discussed in the medical literature. There is much further work to be done from an industry, research, and approval process to make more of these implants available for daily use by orthopedic surgeons in the United States.
Additionally, the cost of pyrocarbon implants for HA is something that must be considered when selecting implants for patients. According to the Pharmaceutical Management Agency (PHARMAC) for New Zealand (2017), a 43-mm diameter CoCr humeral head implant cost $2,340, while the same component created in pyrocarbon cost $3,800 New Zealand dollars (Ramírez-Martínez et al. 2020). One limitation discussed with pyrocarbon implants in the wrist and hand is the increased cost profile compared to other implants due to the technologically advanced properties of the material (Daruwalla et al. 2012). Orthopedic surgeons have to evaluate for each patient clinical scenario if the heightened cost of the pyrocarbon is worth the possible benefit the implant may offer. The cost analyses and economic burden of the implant when it comes to the shoulder has not been studied extensively given the implant is relatively early in it clinical use. Further research will be needed to fully elucidate its cost effectiveness.
Future Directions
Management of severe glenohumeral arthritis in adults > 65 years old has been achieved and well documented with anatomic TSA. However, in the young patient (< 60 years-old), management of this disease process is quite limited due to factors including activity level, status of the rotator cuff and likelihood of future revision. The introduction of pyrocarbon in orthopedics as an alternative for wrist/hand arthroplasty and now shoulder arthroplasty has provided a solution for the management of glenohumeral arthritis in young adults. As mentioned throughout this review, the current literature indicates that the use of pyrocarbon humeral implants in the setting of HA has decreased wear of the native glenoid when compared to the most commonly used CoCr humeral implants (Klawitter et al. 2020; Tsitlakidis, Doll, Westhauser, et al. 2021). However, the use of these implants does not come without risks. As described above, there is a risk of implant fracture/failure when using pyrocarbon for HA at intermediate follow up. Thus, future studies are needed in order to address the concerns of implant failure and to assess short, intermediate, and long-term outcomes in young patient populations following HA with pyrocarbon implants. This is critical as implant fracture is a devastating complication and solutions to this problem could lead to easier adoption of pyrocarbon implants into clinical practice. Another important realm which needs studied is the cost effectiveness of these implants, as pyrocarbon implants are more expensive so cost benefit analysis must be weighed over time.
The use of pyrocarbon humeral implants in HA has been of interest in recent literature due to its mechanical properties that lend to a reported decreased likelihood of revision to TSA in the younger population. Moreover, due to its demonstrated pattern of increased wear resistance, some studies have evaluated the wear characteristics of pyrocarbon implants paired with polyethylene inserts in both TSA and RSA and were found to have statistically improved rates of wear compared to CoCr, as detailed above (Ramírez-Martínez et al. 2020; Mueller, Braun, Schroeder, et al. 2017). Therefore, due to its favorable characteristics, pyrocarbon implants may continue to emerge throughout the field of orthopedics. We think one potential field that could possibly be at the forefront of this emergence would be hip arthroplasty. Pyrocarbon would avoid the problems that come with metal prosthetics and limit osteolysis and accelerated wear patterns thus possibly leading to prolonged implant longevity, however; this has not yet come to the market.
Discussion
Treatment of glenohumeral joint osteoarthritis in young patients remains a challenge. This is due to the increased average activity level of this patient population as well as the necessity for implant longevity in the setting of joint arthroplasty. In young patients, due to the concern for native glenoid erosion with traditional metallic humeral components following HA, the role of pyrocarbon is being explored. With modulus similar to cortical bone, pyrocarbon has been introduced as an alternative to traditional metallic implants in joint arthroplasty. This review aimed to highlight the properties and indications of pyrocarbon in HA, as well as synthesize the clinical outcomes and available implants for use at this time.
Pyrocarbon has a similar modulus of elasticity of cortical bone and has the ability to form a cartilaginous matrix due to the expression of type II collagen (Hannoun, Ouenzerfi, Brizuela, et al. 2019). Klawitter et al. found that CoCr humeral implants resulted in significantly greater rates of bone loss and surface roughness when compared to pyrocarbon implants (Klawitter et al. 2020). This was also seen in a similar study that found complete loss/destruction of glenoid bone when paired with traditional metallic implants versus pyrocarbon implants when subject to continuous cycles of dynamic range of motion (Mueller, Braun, Schroeder, et al. 2017). Another study found that the cartilage survival rate was significantly higher with pyrocarbon HA (92%) versus metal implants (20%) (Cook, Thomas, and Kester 1989). One study detailed pyrocarbon’s ability to generate a cartilaginous matrix where they found that pyrocarbon led to cartilage regeneration in 86% of cases versus 25% for CoCr at the opposing joint (Kawalec et al. 1998). Additionally, Mathon et al. found glenoid wear to be less than 0.6-mm at 3 years follow up, which is 5 times less than metallic implants (Mathon et al. 2023).
Some studies have demonstrated lower revision rates with pyrocarbon components in HA when compared to industry standard metal implants (McBride, Ross, Hoy, et al. 2022; Gao et al. 2023). In their 2023 systematic review, Park et al. also had favorable revision rates and clinical outcomes with a significant improvement in post-operative range of motion (Park, Zhang, Chang, et al. 2023). However, TSA continues to demonstrate superior improvements in post-operative motion and shoulder function, when compared to both pyrocarbon and traditional metallic HA (Garcia, Liu, Mahony, et al. 2016).
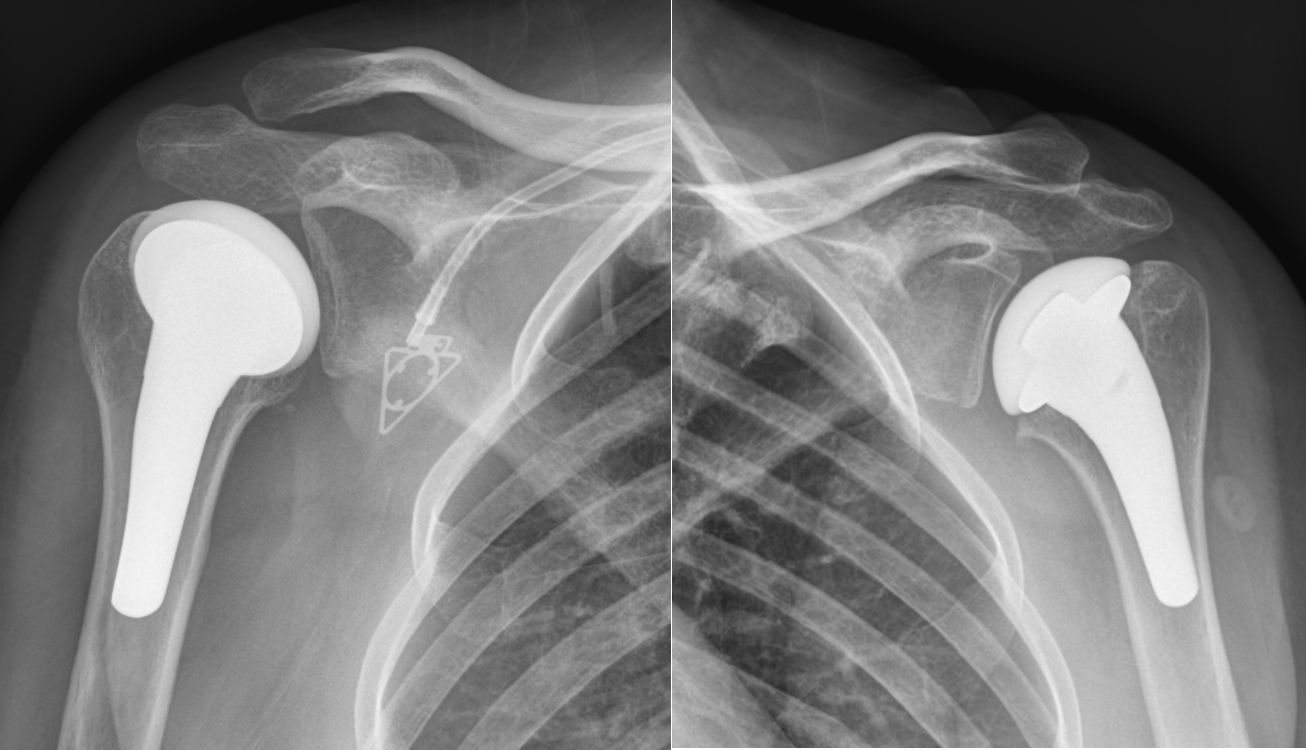
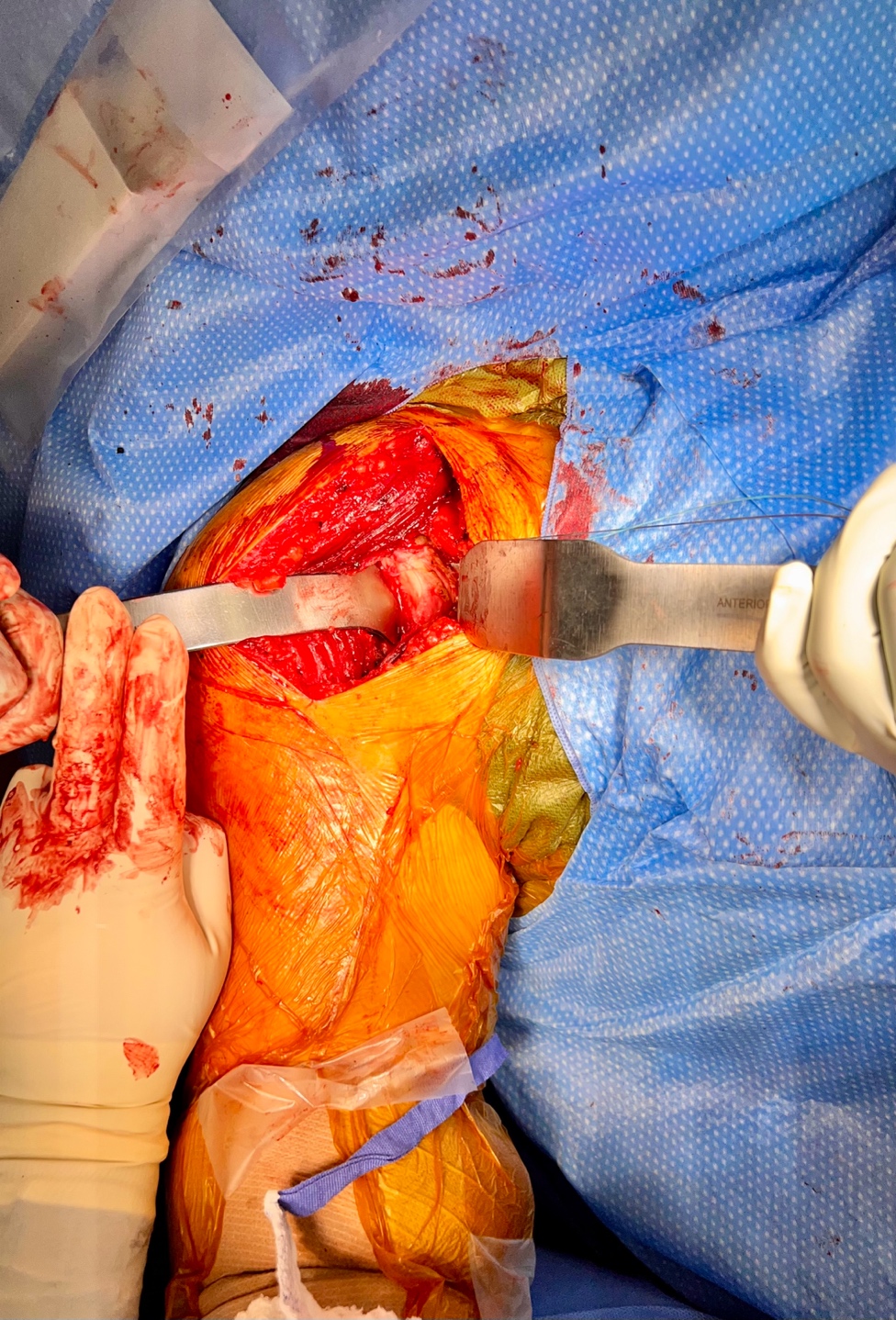
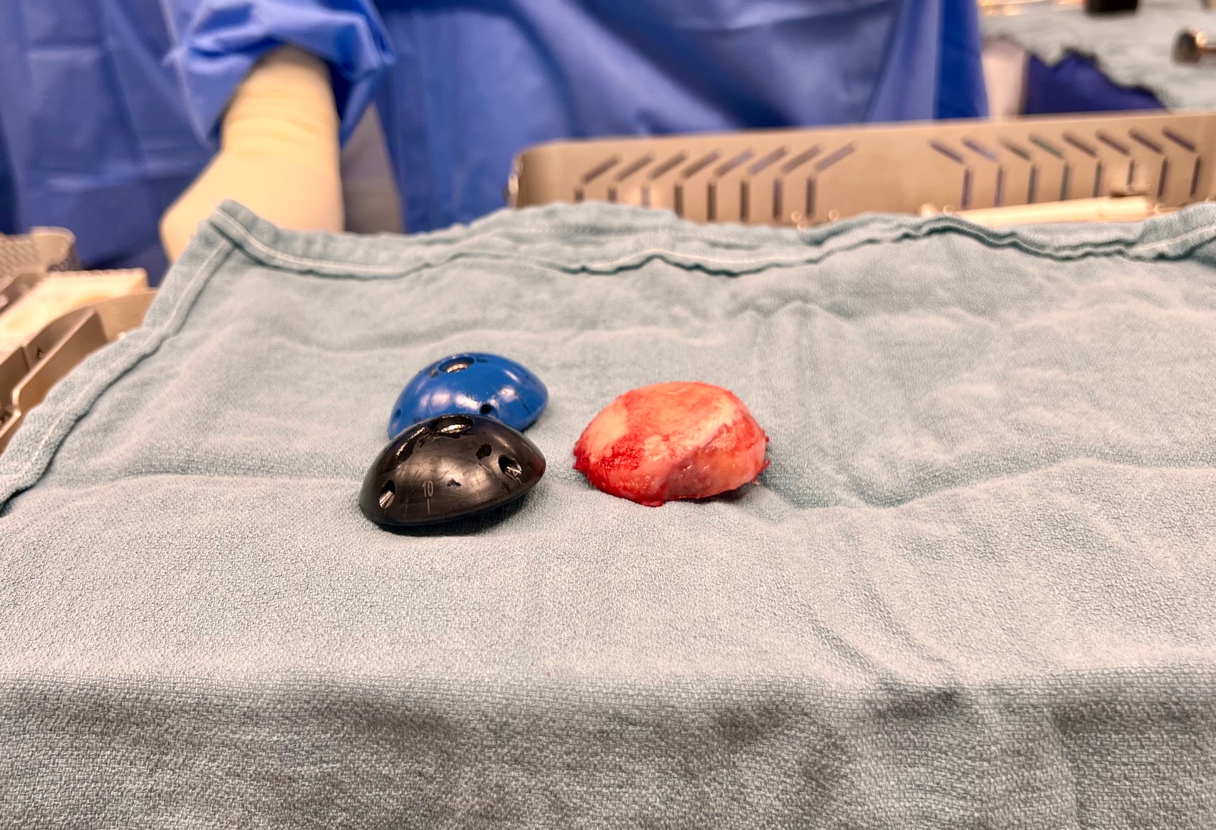
In our clinical practice, we have begun to incorporate pyrocarbon HA primarily for young patients with shoulder pain from proximal humerus AVN. In this setting usually, the glenoid is spared. Therefore, the use of the pyrocarbon head on the native glenoid cartilage can potentially have benefits in glenoid wear over-time compared to a metal head. There are also some situations that we consider pyrocarbon HA in young patients with glenohumeral arthritis and a high activity level. If these patients need to lift more than 30-40 pounds with their operative arm, then we consider a HA over an anatomic TSA due to the increased loads. In this patient population, we consider a pyrocarbon HA over a metal head to try to decrease the glenoid wear over-time. An example is seen in Figures III-VI of a 36-year-old male in active-duty military with right glenohumeral arthritis. Due to his high activity demands he underwent a HA with a pyrocarbon head (Stryker, Mahwah, NJ, USA). Figures III and IV demonstrate his significant humeral arthritic wear and osteophytes with moderate posterior glenoid wear. Figure V demonstrates the high offset and low offset trial heads compared to the anatomic head cut. We use the anatomic head cut as a template to match the implant diameter and offset sizing to avoid overstuffing. Figure VI shows the implanted pyrocarbon HA.




The most relevant limitation to this study is due to the limited amount of literature evaluating the use of pyrocarbon implants in shoulder arthroplasty, especially in vivo. Although some studies are described and mentioned above, follow up was limited to short-term follow up. Thus, it will be important for future studies to evaluate post-operative outcomes for patients undergoing HA with pyrocarbon implants. Although current research is in favor of decreased glenoid wear when using pyrocarbon versus traditional metallic implants for HA, future studies are needed to assess implant survival at 5 and 10 years due to the increased risk of implant fracture/failure with pyrocarbon. Lastly, the only pyrocarbon implant FDA approved for use in the U.S.A. is Stryker’s Tornier Pyrocarbon Humeral Head (Stryker, Mahwah, NJ, USA). As pyrocarbon implants evolve and new products are developed, further biomechanical studies should evaluate the survival of these implants compared to metal heads.
Conclusion
This study outlines the biomechanical properties of pyrocarbon as well as indications for use in HA in young adults with glenohumeral arthritis or AVN. Pyrocarbon is a promising product for this patient population with a majority of studies finding lower rates of revision, decreased bone destruction and decreased wear rates when paired with polyethylene components compared to industry standard metallic implants. Further research is required to assess intermediate and long term outcomes of these implants and to compare various pyrocarbon implants to other shoulder replacement techniques.
Ethics
This is an observational study. The Vanderbilt Orthopaedic Surgery Research Ethics Committee has confirmed that no ethical approval is required.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection analysis, and manuscript drafting was performed by River Fine, Jake Fox, Peter Chang, and Paul Inclan. Jed Kuhn and Lance LeClere were involved in manuscript revision. All authors read and approved the final manuscript.
Consent
No funding was required for this project
Funding
The authors did not receive support from any organization for the submitted work.
Financial and Non-Fianancial Competing Interests
The authors declare that they have no competing interests