

Introduction
Reverse shoulder arthroplasty (RSA) has been used to improve shoulder joint mobility and reduce pain by medializing the center of rotation to recruit more deltoid fibers for forward elevation and abduction (Best et al. 2021; Boileau et al. 2005; S. H. Kim et al. 2011; Ma et al. 2021). RSA also increases deltoid length and tension, allowing for better deltoid function that compensates for the absence of a functional rotator cuff (Boileau et al. 2005). Despite these advancements, over-tensioning of the deltoid can lead to postoperative complications, such as acromial stress fractures and prosthetic instability from under-tensioning the deltoid (Boileau et al. 2005; Lädermann et al. 2012, 2009). Deltoid tensioning and intraoperative decision-making can impact perioperative complications after RSA, which is associated with increased length of hospital stay and revision surgeries, ultimately increasing hospital costs (Menendez et al. 2015; Ponce et al. 2015; Scott et al. 2019).
Radiographic measurements have been identified in the literature as predictors of clinical outcomes. Specifically, arm lengthening, a proposed radiographic objective measurement used to represent deltoid tensioning, has been correlated to postoperative function and outcomes (Boileau et al. 2005). Currently, intraoperative tension and stability assessments are used to evaluate muscle tensioning, but specific deltoid functioning continues to be determined by surgical experience (Boileau et al. 2005; Lädermann et al. 2009). Studies have been done to establish optimal deltoid tensioning by evaluating an optimal range of arm lengthening, with one study finding up to 15 mm sufficient to provide adequate deltoid tensioning and others suggesting less deltoid tensioning leading to increased anterior instability (Boileau et al. 2005). More so, arm lengthening has been used to evaluate the relationship of deltoid tensioning to postoperative outcomes. Recent evaluations of the influence of arm lengthening on functional outcomes have shown varied results, including the inconclusive relationship between arm lengthening and postoperative active forward elevation (Aydin, Capkin, and Yilmaz 2022; Jobin et al. 2012; Lädermann et al. 2012; Sabesan et al. 2016; Werner et al. 2017).
Additional radiographic measurements correlated with outcomes in RSA is the β angle, which is reflective of glenoid inclination and measures the angle between the floor of the supraspinatus fossa and the line of the glenoid fossa (Maurer et al. 2012). Superior inclination of the baseplate in RSA has been associated with an increased risk of scapular notching (Falaise, Levigne, and Favard 2011). The literature has shown significant correlations between scapular notching and lower functional outcome scores, lower postoperative range of motion and strength, and increased complication rates (Mollon et al. 2017; Simovitch et al. 2019; Wellmann et al. 2013). Therefore, scapular notching from the superior inclination of the baseplate places patients at increased risk for increased complications and suboptimal postoperative shoulder function. There have been mixed conclusions regarding the relationship between superior baseplate inclination and its association with the risk of instability after RSA (Bechtold et al. 2021; Tashjian et al. 2018). Few studies have demonstrated relationships between glenoid inclination and outcomes following RSA. This study evaluated the relationship between radiographic measurements, specifically AHD representing arm lengthening and postoperative β angle, and patient outcomes following RSA.
Materials and Methods
Study Design
This was an institutional review board-approved retrospective study of adults (aged ≥ 18 years) undergoing elective RSA by a single surgeon from a single institution from August 2017 to February 2020 with radiographic follow-up and a minimum clinical follow-up of 1 year. Patients were excluded with incomplete follow-up, a diagnosis of fracture, or revision surgery.
Patient Evaluation and Data Analysis
Two independent investigators retrospectively reviewed the electronic medical records (*initials blinded for peer review*) while data were prospectively collected. Patient demographics, including age at the time of surgery, gender, body mass index (BMI), ethnicity, and time to follow-up were collected. The primary endpoints were Constant score, patient-reported outcomes (Simple Shoulder Test (SST), American Shoulder and Elbow Surgeons (ASES), University of California at Los Angeles Shoulder Score (UCLA Shoulder Score), Shoulder Pain and Disability Index (SPADI), Shoulder Arthroplasty Smart Score (SAS)) and active range of motion (forward elevation, abduction, external rotation). All outcomes were collected preoperatively and at the last follow-up.
Radiographic assessment
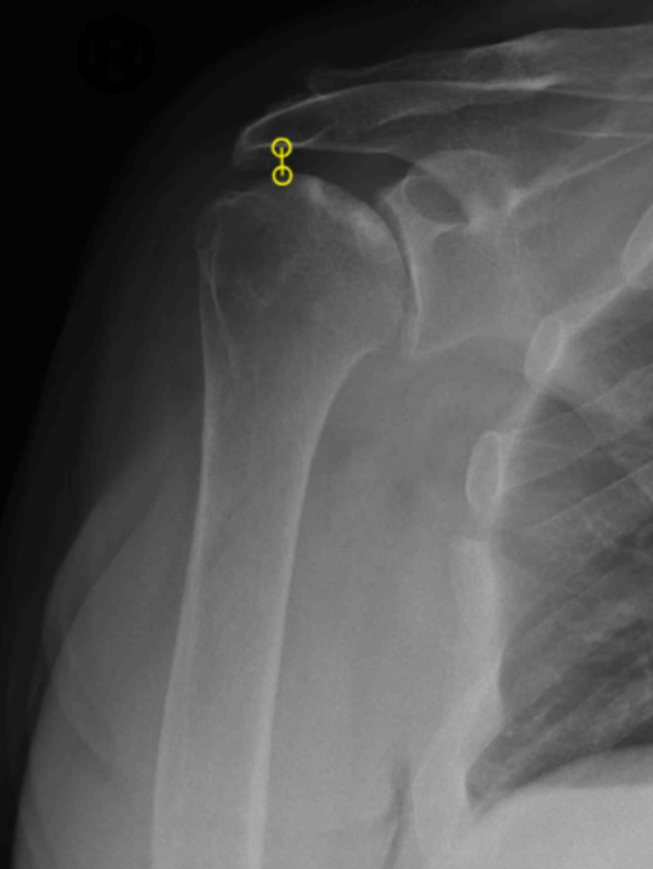
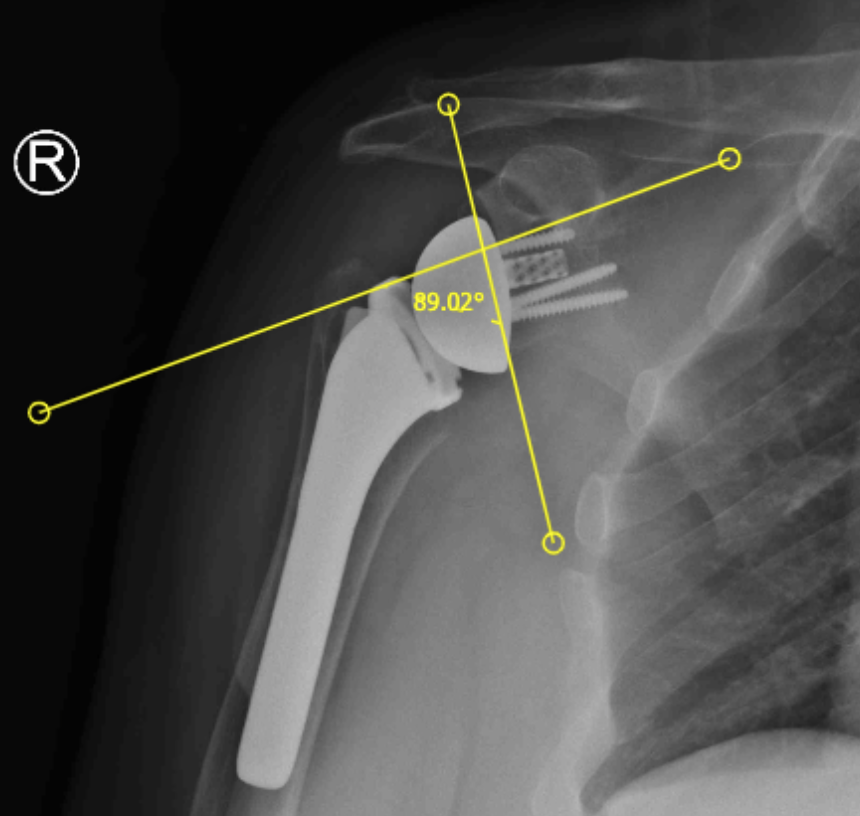
Standardized true AP shoulder radiographs were obtained for all preoperative and postoperative follow-up appointments. Preoperative AHD was measured using the most recent preoperative shoulder x-ray. Postoperative AHD and glenoid inclination angle, β-angle, were measured using shoulder radiographs at least three months from the surgery date. Arm lengthening, also known as AHDdelta, was defined as the difference between postoperative and preoperative AHD measurements. All radiograph measurements were taken according to the criteria outlined by Berthold et al (Berthold et al. 2021). More specifically, the AHD was measured by obtaining the perpendicular distance between the most lateral aspect of the acromion and the superior portion of the greater tuberosity (Figure I) (Berthold et al. 2021). In addition, the β angle was obtained by measuring the angle between the floor of the supraspinatus fossa and the line of the glenoid fossa, as outlined in Maurer et al. (Figure II) (Maurer et al. 2012).


Surgical Procedure
The operation was performed with a standardized technique with the Equinoxe Onlay Platform Shoulder System standard reverse prosthesis (Exactech, Inc., Gainesville, FL, USA) used in all subjects. A standard deltopectoral approach was used for all patients. After the implants were placed according to the manufacturer’s recommendation, the subscapularis tendon was repaired if deemed possible by the surgeon.
Statistical Analysis
The cohort demographics were summarized with means and interquartile ranges for continuous variables and frequencies for categorical variables. The intraclass correlation coefficient (ICC) was calculated to assess the interrater reliability of the radiographic measurements. Pearson correlation coefficient tests and linear regressions were performed to examine the association between radiographic measurements and clinical outcomes. Student’s t-tests were used to compare preoperative and postoperative outcome scores and range of motion. Scattered plots were used to illustrate the relationship of postoperative β angle to SPADI and SST scores. A subgroup analysis was performed comparing outcomes of patients with ≤ 2 cm AHDdelta versus > 2 cm AHDdelta. All data analyses were performed using R and statistical significance was defined as p-value < .05.
Results
A total of 63 patients (n=44 females, n=19 males), with a mean age of 73.3 ± 8.7 years and a mean BMI of 28.5 ± 5.8 kg/m2, were included in this analysis. There was a mean follow-up of 19 ± 7.3 months. Good interrater reliability was observed for the preoperative AHD (ICC: 0.88; CI: 0.69-0.96) and AHDdelta (ICC: 0.84; CI: 0.59-0.94) measurements. Postoperative AHD (ICC: 0.91; CI: 0.75-0.97) had excellent interrater reliability, whereas postoperative β angle (ICC: 0.39; CI: -0.14-0.75) showed poor reliability (Table I).
Radiographic measurements are summarized in Table I. A mean arm lengthening of 2.4 ± 0.9 cm and a mean postoperative β angle of 89.6° ± 10.6° were observed. Overall, participants experienced improvements in range of motion and patient-reported outcomes. Patients had a mean improvement of active forward elevation by 77° ± 28.9°, active abduction by 68.1° ± 36.4°, and active external rotation by 16.8° ± 21°. The Constant score improved by a mean of 32.3 ± 15.6 points, ASES improved by a mean of 40.5 ± 26.3 points (range, -53 to 87 points), UCLA by a mean of 16.7 ± 5.7 points, SPADI by -58.1 ± 29.1 points, SAS by 31.5 ± 13.9 points, and SST by 6.4 ± 3.5 points. Daily pain improved by -4.4 ± 3.6 points, worst pain by -5.1 ± 3.9 points, and shoulder function by 4.7 ± 2.8 points (Table II).
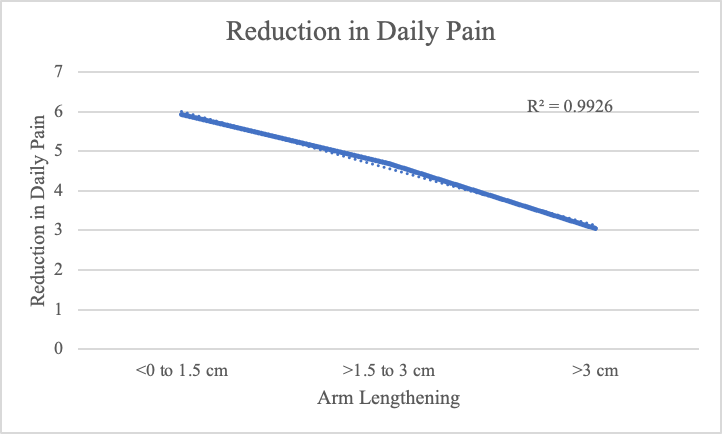
When assessing arm lengthening and its relationship to outcomes, a weak correlation was observed between arm lengthening and improvement of daily pain (r = 0.277, p = 0.030) (Figure III). The greatest improvement in daily pain was observed in arm lengthening from less than 0 to 1.5 cm. Whereas the lowest improvement in daily pain was observed in arm lengthening greater than 3.0 cm (Table III). When comparing outcomes of patients with ≤ 2 cm of arm lengthening versus > 2 cm of arm lengthening based on our subanalysis it was consistently observed that patients with an arm lengthening of ≤ 2 cm had a significantly greater decrease in daily pain than those with an arm lengthening of > 2 cm (-5.9 vs -3.8; p = 0.02) (Table IV). All other outcomes were similar between the two groups including active forward elevation (p=0.88), active abduction (p=0.47), active external rotation (p=0.07), passive external rotation (p=0.69), worst pain (p=0.85), Shoulder Function score (p=0.99), SST (p=0.46), Constant score (p=0.25), ASES score (p=0.39), UCLA score (p=0.22), SPADI (p=0.75), and SAS (p=0.25).

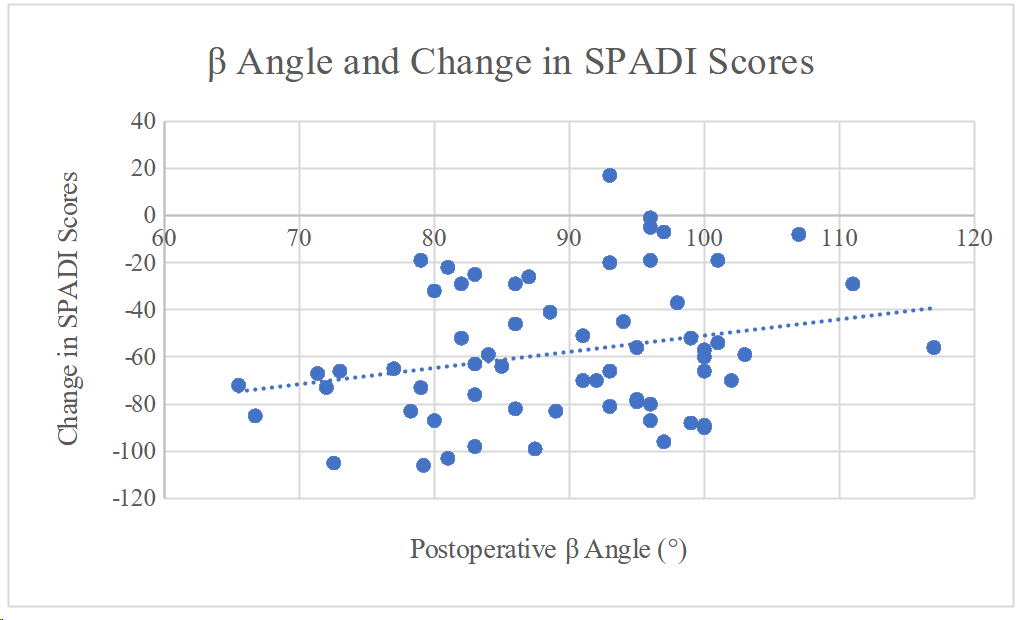
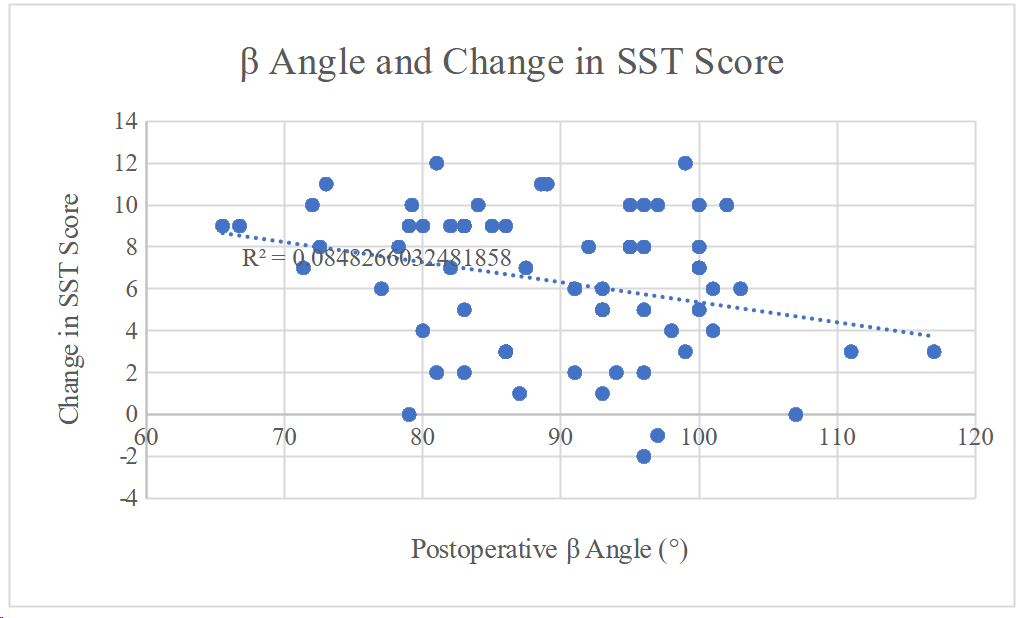
A weak correlation between postoperative β and improvement of SPADI scores was observed (r = 0.251, p = 0.047) (Figure IV). In addition, a weak negative correlation was found between postoperative β angle and improvement of SST scores (r = -0.291, p = 0.021) (Figure V). No other statistically significant correlations were observed between radiographic measurements and improvements in outcome measurements (Table V).


Discussion
Reverse shoulder arthroplasty (RSA) has grown exponentially due to its effectiveness in restoring clinical function and reducing pain. With this growth, the priority has been placed on expanding indications and optimizing outcomes while minimizing complications. Assessment of various factors, including radiographic measurements and biomechanical factors, have emerged as possible tools to predict and guide optimal outcomes. Our study evaluated two previously reported radiographic measurements to identify their utility in predicting clinical and functional outcomes after RSA. The principal purpose of this investigation was to identify optimal arm lengthening and postoperative β angles that could optimize patient-reported satisfaction after RSA. Our results demonstrated optimal improvement of daily pain was seen with arm lengthening ranging from 0 cm to 1.5 cm and improvement of SPADI and SST scores correlated with postoperative β angle.
We found, on average, for our cohort, there was 2.36 cm of arm lengthening, which was comparable with previously reported studies looking at lengthening after RSA in the literature (1.6-2.9 cm) (Jobin et al. 2012; Lädermann et al. 2012; Sabesan et al. 2016; Werner et al. 2017). Our study found that the greatest improvement in daily pain was observed in arm lengthening ranging from 0 to 1.5 cm. Subsequently, we performed a subanalysis to further delineate a relationship between the degree of arm lengthening and postoperative outcomes which found that patients with arm lengthening ≤ 2 cm had a more significant reduction in daily pain than those whose arm lengthened > 2 cm. This is similar to a study by Boileau et al (Boileau et al. 2005). that found that arm lengthening up to 1.5 cm was sufficient for deltoid tensioning.
Inadequate deltoid tensioning, however, has been shown to have a relationship with poorer postoperative outcomes following RSA. A study performed by Werner et al. demonstrated that arm lengthening had significant correlations to increased postoperative Constant scores (Werner et al. 2017). Our subanalysis of arm lengthening showed that arm lengthening between 1 and 2.5 cm correlated to the highest Constant scores. The literature supports that 1.5-2.5 cm of arm lengthening might be the optimal goal for postoperative pain levels and functional outcomes (Boileau et al. 2005; Jobin et al. 2012; Lädermann et al. 2012, 2009; Werner et al. 2017).
While arm lengthening is a proposed measurement reflective of deltoid tensioning, our results did not demonstrate this. It has been postulated that over-tensioning of the deltoid represents excessive arm lengthening and may predispose patients to permanent arm abduction, neurologic deficits, and acromial fractures (Boileau et al. 2005, 2006; H. J. Kim et al. 2020; Lädermann, Edwards, and Walch 2014; Lädermann et al. 2011, 2012, 2009). Few studies have found a significant relationship between arm lengthening and neurologic damage with recent studies suggesting anywhere from 2-4 cm of lengthening at increased risk of postoperative neurologic deficit (H. J. Kim et al. 2020; Lädermann, Edwards, and Walch 2014; Lädermann et al. 2011, 2012). There is yet to be a degree of excessive arm lengthening that coincides with an increased risk of acromial fractures or instability. Still, the literature has found that osteoporotic patients with over-tensioning of the deltoid can also increase the risk for acromial fractures (Boileau et al. 2005, 2006; Lädermann et al. 2009). Furthermore, those with inadequate lengthening and deltoid tension are at increased risk for joint instability. Yet, there is no specific range of quantitative values for inadequate lengthening that predisposes patients to this (Boileau et al. 2005, 2006; Lädermann, Edwards, and Walch 2014).
As for the β angle, our study found a mean of 89.6° ± 10.6° and no significant relationships with range of motion or most outcome scores. However, our study did observe a significant correlation between β angle and positive delta SST and negative delta SPADI scores. This indicates these patients had greater mobility and stability as well as less pain. A study by Kirsch et al (2021). found a similar postoperative β angle of 83 ± 8° and improvement in SST in a cohort of 44 patients that underwent primary RSA. This was further supported by Chalmers et al (2019). who found the gold-standard 3D β angle to be 83° ± 5°. Previous literature has been conflicted on the relationship between glenoid inclination and outcomes for RSA. Specifically, Bechtold et al (2021). reported no significant relationship between the postoperative beta angle and shoulder instability following RSA. The range of beta angles in their study (range, 63° - 100°) were similar to our study, providing some external validity to our measurement. A recent study by Tashjian et al (2018). found a negative correlation between instability and beta angle, and a published review by Favard et al (2017). recommended a beta angle at 90° in order to prevent notching and instability based on normal anatomical values. However, shoulder instability was not within the scope of our study. Overall, our finding of a positive correlation with postoperative beta angle and SST scores was supported by previous literature, and the literature seems to support the possibility of a target beta angle for shoulder arthroplasty, which would benefit from further investigation. Previous research has focused on shoulder instability, with minimal data on patient-reported outcomes.
Limitations
This study has several limitations. First, implant type and design influence results for RSA and this study included only one implant type using an onlay humeral component with humeral-sided lateralization. Although this provides for consistency and less variation impacting our radiographic measurements, the findings in this study may not apply to other implant design types and may be less generalizable. Second, the small sample size may limit the ability to assess and account for all factors impacting outcomes, which is a multifactorial variable. Larger sample sizes in future studies are needed to account for additional variance in patients and implant types and their impact on these radiographic measurements. Additionally, variations in radiograph quality and measurements can be seen with any radiographic outcome study. This was minimized as all radiographs were performed by two radiology technicians in two offices, and the views and techniques were standardized prior to this study. In addition, two reviewers were compared for intraobserver and interobserver reliability to verify our results’ accuracy. Inevitably, variations in views and imaging exist and can impact our measurements and conclusions.
Conclusion
The results of our study showed that AHD increased postoperatively after RSA and that less arm lengthening had the most significant decrease in pain and optimal glenoid inclination correlated with improved outcome scores.