

INTRODUCTION
Over the past two decades opioid use has risen at a disturbing rate in the United States (US), with the number of opioid prescriptions increasing from 76 million in 1991 to 207 million in 2013; a 272% increase (“DrugAbuseStatistics.Org,” n.d.). The distressing trends of opioid misuse led to a national health crisis that began in the mid-2010s (Mclellan 2017; Alghnam and Castillo 2017). From July 2016 to September 2017, the number of opioid-involved overdose emergency room visits in the US was 142,557. Opioid use has been linked to a higher risk of all-cause mortality compared with other common pain medications (Ray et al. 2016). In particular, use of long-acting opioid increases the risk of unintentional overdose deaths and has been associated with mortality from cardiorespiratory and other causes (Ray et al. 2016). In 2017 alone, over 60,000 opioid-related deaths were reported in the US (“DrugAbuseStatistics.Org,” n.d.). In response, the U.S. Department of Health and Humans services officially declared the opioid crisis a “public health emergency” in 2017 (Digital Communications Division, n.d.). In the two years following this declaration, the country witnessed heavy anti-drug ad campaigning which seemed to produce promising results as the number of deaths from prescription opioid overdose fell from 17,029 in 2017 to 14,139 in 2019 (“Ongoing Emergencies & Disasters,” n.d.). However, the number of deaths attributed to prescription opioid overdose increased yet again between 2019-2021, accounting for a staggering 16,706 deaths in the US (Digital Communications Division, n.d.). Additionally, the economic burden of opioid misuse continues to grow at an alarming pace. The US Joint Economic Committee reported that the opioid epidemic cost the US nearly $1.5 trillion in 2020, an increase of 37% from 2017 (n.d.). These unsettling trends are linked primarily to a marked increase in patient opioid prescriptions. Thus, more attention has been focused on reducing opioid prescriptions by managing pain via alternative methods.
Opioids are commonly prescribed for pain in the acute postoperative period following many orthopedic procedures with orthopedic surgeons noted to prescribe two times the quantity of opioids per prescription compared with other surgical specialities (Cron et al. 2020). Investigating new and innovative ways to manage postoperative pain is of keen interest in orthopedics. The objective of this study was to determine if cryoneurolysis within three months prior to total knee arthroplasty (TKA) resulted in reduced opioid consumption postoperatively.
METHODS
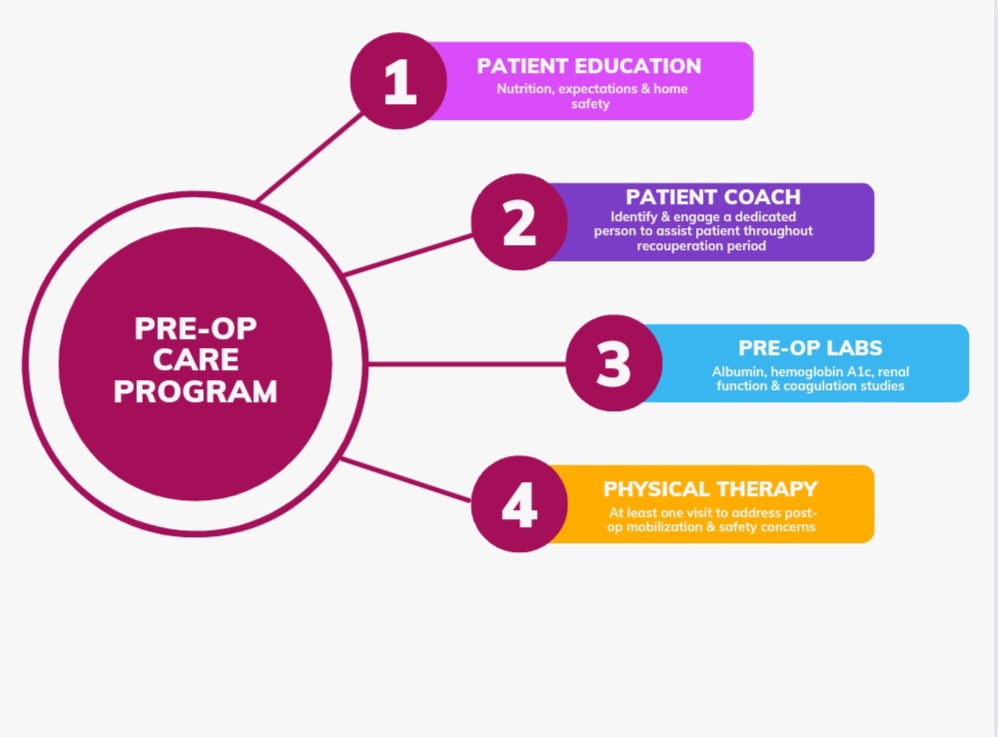
An IRB approved retrospective chart review of 183 patients undergoing primary TKA between August 2022 and February 2023 was conducted. Patients were excluded from review if they were prescribed opioids for a second joint replacement within 90 days of the index procedure to minimize the potential for increased opioid consumption related to overlap between the two procedures. All patients included in the study participated in the lead author’s previously published preoperative care protocol (Figure 1) (Stevenson and Wickline 2020). In addition to the preoperative care protocol, all patients were offered cryoneurolysis (iovera°, Pacira CryoTech, Inc., Fremont, CA, USA) therapy. The cryoneurolysis procedure consists of exposing a localized zone of the peripheral nerves to nitrous oxide at temperatures below -20°C forming a cold zone leading to Wallerian degeneration of the nerve axons resulting in long-acting nerve block (Mihalko et al. 2021). The lead author performed this procedure, per manufacturer guidelines, using anatomic landmarks to target the anterior femoral cutaneous nerve (AFCN) and two inferior branches of the saphenous nerve. Patients who provided consent to cryoneurolysis had this procedure performed within three months prior to the scheduled TKA surgery date. On the day of surgery, all patients, whether that had preoperative cryoneurolysis performed or not, received an injection of 10cc of long-acting liposomal bupivacaine in the adductor canal prior to being transported to the operating room and an additional 10cc of short-acting bupivacaine was injected in to the adductor canal immediately prior to the surgical procedure. The initial amount of opioid pills prescribed postoperative was based on preoperative evaluations and conversations between the lead author and each patient. All patients also participated in a postoperative rehabilitation plan which consisted of an at home therapy protocol of icing and elevating the affected limb for 40 minutes of each hour and performing 10 ankle pumps, 10 passive/active-assisted knee extensions, and 10 knee flexion exercises in a chair every 60 minutes during waking hours for the first two weeks following surgery. Patients were also encouraged to take a short walk daily to help prevent postoperative deep vein thrombosis and pneumonia. Patients who achieved less than 100° knee ROM and/or had lymphedema were referred to a Physical Therapist.

The following data was collected from the chart review: American Society of Anesthesiologists (ASA) class, body mass index (BMI), age, sex, 2-week and 6-week postoperative knee range of motion (ROM), preoperative and postoperative opioid medication use, preoperative use of medications prescribed for the treatment of a mood disorder, anxiety and/or depression, and whether the patient had consented to and had presurgical cryoneurolysis performed. Pre- and postoperative opioid medication use was determined using the New York State Internet System for Tracking Over-Prescribing (NYS I-STOP) database; data collected included the type of opioid medication prescribed, the total number of tablets dispensed, and number of refills requested by each patient throughout the first 90 days in the postoperative course. Patients were considered to be preoperative opioid users if they were actively prescribed/using opioids in the 3 months prior to their scheduled TKA. The preoperative prescription medication for treatment of a mood disorder was defined as patients who had been prescribed SSRIs, SNRIs, and/or NDRI in the 3 months prior to their surgery.
RESULTS
Baseline patient demographics and characteristics
A total of 183 patients were included in this retrospective review (Table 1). The mean patient age was 67.9 ± 7.9 years. A total of 21 patients (11.5%) had a history of chronic opioid use, defined as opioid consumption within 3 months prior to scheduled surgery. A total of 153 (83.6%) patients received cryoneurolysis within three months prior to undergoing TKA.
Postoperative opioid consumption
A total of 178 (97.3%) of patients filled their postoperative opioid prescription. Most of these patients (93.8%) were initially prescribed 10 opioid pills at the time of discharge. The greatest proportion of the 183 patients consumed between one and ten opioid pills (75.4%) or 11 to 30 opioid pills (17.5%; Table 2). Of the 178 patients who filled their postoperative opioid prescriptions, 31 (17.4%) requested at least one refill; the majority (n=23/31, 74.1%) of these patients initially received 10 tablets of Tramadol HCL 50 mg. Six (19.4%) of the patients who requested a refill on their medications were taking opioids preoperatively; 9 (29%) patients were being actively treated for mood disorders, including anxiety and/or depression. Three of the patients (9.7%) that requested a refill on their opioid prescriptions were being actively treated with both an opioid and at least one mood disorder medication prior to their surgery. Twenty-four (77.4%) of the patients who requested refills had received cryoneurolysis within three months prior to their scheduled surgery.
Postoperative Rehabilitation
Knee Range of Motion
Postoperative knee ROM was similar for patients who received cryoneurolysis prior to surgery compared with patients who did not receive cryoneurolysis prior to surgery (2.7 – 111 vs 2.6 122). At 6-weeks postoperative, patients who followed the home-based therapy as outlined and received cryoneurolysis achieved greater mean knee ROM compared with patients who followed the home-based therapy as outlined and declined preoperative cryoneurolysis (2-121vs 1 – 122; Table 6). Of note, a total of 15 patients did not have a 6-week ROM value recorded in their charts; therefore, the above information was obtained using the data of 168/183 patients.
Physical Therapy
Fifty-seven (31.1%) patients were referred to a Physical Therapist, including 2 who received physical therapy aid from friends and/or relatives that are Physical Therapists without a formal therapy referral. A total of 50 (87.7%) of the patients who received physical therapy had undergone cryoneurolysis prior to their TKA; three (6%) of these patients required manipulation at 6-weeks postoperative.
DISCUSSION
The use of opioid medications has skyrocketed in the U.S. and with it, opioid-overdose related deaths (Digital Communications Division, n.d.). Publication of guidelines on postsurgical opioid prescribing have been produced based on a limited level of evidence (Overton et al. 2018; Howard et al. 2018; Hill et al. 2018). As a result, some positive impact has been made on opioid prescribing practices, but it is not enough. Improved preoperative, perioperative, and postoperative strategies must be developed to prevent chronic use and dependence on opioid medication.
To date there is a paucity of research investigating the outcomes of multimodal analgesia and the impact seen on long-term opioid use following surgery. In a 2020 study, the lead author found that a novel perioperative protocol utilizing an adductor canal (ABC) continuous catheter and unique home therapy program was able to significantly reduce the amount of opioids needed for post-TKA management with 86% of patients needing 10 opioid pills or less through 90 days (Stevenson and Wickline 2020). Since this previous publication, the lead author has amended his practice to include a single shot adductor canal block with short acting and long-acting bupivacaine.
The results of a published study of 100 patients undergoing cryoneurolysis prior to TKA illustrated significantly shorter hospital stays, fewer opioid consumption, and decreased post-operative pain (Dasa, Lensing, Parsons, et al. 2016). However, when comparing opioid usage in the patients treated with an adductor canal block with short acting and liposomal bupivacaine with and without cryoneurolysis to the lead author’s previously published study results using ACB with catheter and large reservoir pain ball alone, the results are comparable. In the lead author’s prior study, 86.3% of patients used 10 opioids or fewer in the 12 weeks following TKA (Stevenson and Wickline 2020). This current study resulted in 78.1% of patients using 10 opioids or fewer post–operatively. Furthermore, in the current study, 77.4% of patients that requested a refill on their opioid medication did undergo cryoneurolysis within 3 months leading up to their TKA procedure. To assess whether a statistically significant difference exists between the number of opioids consumed post-operatively by patients that did receive cryoneurolysis in comparison to those that declined cryoneurolysis, a Mann-Whitney U test was conducted. The Mann-Whitney U test was used since the cryoneurolysis group did not satisfy assumptions of normality, as per the Shapiro Wilks test. As illustrated in Table 7, the Mann-Whitney U test has shown that there is no statistically significant difference in the number of opioid tablets consumed post-operatively between the two patient cohorts.
The Journal of American Geriatrics Society reported that the three most common surgeries performed on U.S. adults between the ages of 65 and 89 years were lens and cataract procedures, knee arthroplasties, and hip replacements (including total and partial replacements), respectively (Deiner et al. 2014). In 2021, the American Joint Replacement Registry reported that between the years of 2012 - 2020, approximately 1,223,300 primary TKAs were performed in the U.S (Siddiqi et al. 2022). Assuming an equal number of TKAs were performed annually, approximately 135,922 primary TKAs were performed per year. In 2016, Hernandez et al. published a study that reported the average number of opiates prescribed to patients status-post TKA at time of discharge was 74 pills (Hernandez et al. 2017). In 2019, a study by Huang et al. was published and indicated the average number of Oxycodone 10 mg tablets required to achieve successful recovery after a TKA was 78 (Huang and Copp 2019). In 2019, Hannon et al published that the average number of opioid pills taken by patients following a total knee arthroplasty ranged from 90-156 pills (Hannon et al. 2019). Although the addition of cryoneurolysis failed to produce a statistically significant decrease in post-op opioid use in this retrospective study, the lead author’s pre-operative treatment pathway, including a adductor canal block, has produced an overall reduction in opioid consumption compared to these three previously published studies (Hernandez et al. 2017; Huang and Copp 2019; Hannon et al. 2019). Thus, the results of this study demonstrate an important pattern in the overall reduction in post-TKA opioid consumption highlighting the utility of incorporating multimodal analgesia into orthopedic surgery pain management protocols.
Limitations
There are several potential confounding variables that may have influenced the study outcomes. The sample size of both groups was substantially different. Of the total 183 patients analyzed in this study, 153 patients (83.6%) received treatment with cryoneurolysis cryotherapy, whereas only 30 (16.4%) patients declined cryoneurolysis treatment. It is possible; therefore, that a portion of the 16.4% of patients who declined cryoneurolysis were outliers to this study. Additionally, it is possible that the overall health, lifestyle, and insurance coverage affected patients’ decision in choosing to receive cryoneurolysis therapy. Further studies may address these limitations.
CONCLUSION
Per the results of the one-tailed Mann Whitney U test it was determined that no statistically significant difference in the total number of opioids consumed was noted post-operatively between the patient cohorts. The results of this study indicate that cryoneurolysis is not necessarily linked to a reduction in post-operative opioid refill requests in patients undergoing TKA.
Acknowledgements
The authors would like to thank Valerie Marmolejo, DPM for her assistance in the development of this manuscript.